Article Text

Abstract
Purpose To assess the extended efficacy and safety of suprachoroidal triamcinolone acetonide injectable suspension (CLS-TA) among patients with macular oedema (ME) secondary to non-infectious uveitis (NIU).
Methods Patients with uveitic ME were treated with suprachoroidal CLS-TA at baseline and week 12 of the Efficacy and Safety of Suprachoroidal CLS-TA for Macular Edema Secondary to Noninfectious Uveitis: Phase 3 Randomized Trial (PEACHTREE) study. Time to rescue was evaluated over 24 additional weeks for MAGNOLIA. Safety data, visual acuity and retinal central subfield thickness (CST) reduction were also evaluated. Of the 53 eligible patients (46 CLS-TA and 7 control), 33 patients were enrolled (28 CLS-TA and 5 control).
Results Over the entire 48-week period for PEACHTREE and MAGNOLIA, the median time to rescue therapy was 257 days versus 55.5 days for the CLS-TA and sham-control arms, respectively. Of 28 CLS-TA treated patients who participated in MAGNOLIA, 14 (50%) did not require rescue therapy through approximately 9 months after the second treatment. Among CLS-TA patients not requiring rescue, there was a mean gain of 12.1 letters and mean CST reduction of 174.5 µm at week 48. No serious adverse events related to study treatment were observed.
Conclusion Approximately 50% of patients did not require additional treatment for up to 9 months following the last CLS-TA administration.
- retina
- macula
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. This study was an extension of the PEACHTREE phase 3 clinical trial, and additional relevant information can be found in that publication, which can be found here: https://doi.org/10.1016/j.ophtha.2020.01.006.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Injection of pharmacotherapy into the suprachoroidal space, located between the sclera and choroid, is an alternative approach, which delivers higher drug concentrations to posterior ocular structures compared with other intraocular and periocular injection procedures.1 In pre-clinical ocular distribution studies, suprachoroidal injection of triamcinolone acetonide injectable suspension (CLS-TA), an investigational corticosteroid formulation of triamcinolone acetonide (Clearside Biomedical, Alpharetta, GA, USA), yielded low levels of the corticosteroid in the anterior segment and high levels in the posterior segment, detectable for over 3 months.1 2 This offers the potential for multi-month durability and decreased adverse events (AEs) such as cataracts and intraocular pressure (IOP) elevation.
The phase 3 PEACHTREE study (NCT02595398) of CLS-TA for macular oedema (ME) due to non-infectious uveitis (NIU) enrolled 160 patients, randomised 3:2 to CLS-TA or sham with 2 administrations delivered 12 weeks apart.3 In the CLS-TA arm, 47% of patients gained ≥15 Early Treatment Diabetic Retinopathy Study (ETDRS) letters in best corrected visual acuity (BCVA) versus 16% in the control arm (p<0.001), meeting the primary endpoint at week 24. No serious adverse events (SAEs) related to treatment were reported.
The primary objective of the MAGNOLIA extension study (NCT02952001) was to evaluate the efficacy of CLS-TA up to 24 weeks following exit from PEACHTREE, as shown by the need for additional (rescue) therapy for the signs or complications of uveitis. The secondary objective of MAGNOLIA was to determine the safety of CLS-TA, assessed as treatment-emergent adverse events (TEAEs), on-study AEs, changes in IOP and changes in cataract grading up to 24 weeks following exit from PEACHTREE.
Methods
Study design
MAGNOLIA was a multicentre, non-interventional extension study, conducted in the USA and India, of up to 24 weeks for patients successfully completing PEACHTREE3 without requiring any rescue treatment during the study period. The last visit of PEACHTREE was considered the crossover visit (day 0) of MAGNOLIA. Patient eligibility was established during the crossover visit. Follow-up visits were conducted every 6 weeks up to 24 weeks following the crossover visit or 48 weeks from PEACHTREE baseline. Study drug was not administered in MAGNOLIA; in order to evaluate the efficacy of CLS-TA without rescue therapy, patients were to be discontinued from MAGNOLIA if rescue therapy became necessary to treat uveitis in the study eye as part of the standard of care, therefore, lowering the number of patients in the study as it progressed. MAGNOLIA was planned and designed after the initiation of the PEACHTREE trial.
Patients
Sites with high enrollment in PEACHTREE were selected to participate in MAGNOLIA. Patients from these sites were eligible to enroll in MAGNOLIA if they completed PEACHTREE without requiring rescue therapy. MAGNOLIA patient eligibility was established during the crossover day from PEACHTREE to the extension study. The PEACHTREE trial was still masked when patients began enrollment into MAGNOLIA; therefore, treatment assignment was unknown at the time of study entry.
Patients provided written informed consent before the study commenced. Patients were not re-randomised to treatment or control at the beginning of MAGNOLIA because of its nature as an observational, non-treatment study. Patients could still receive rescue therapy, but would exit the observational study at that point. Among participating centres, patients who enrolled in MAGNOLIA were compared with those who did not enroll, to assess for selection bias; baseline characteristics, efficacy and safety outcomes were compared.
Efficacy endpoint assessments
The primary endpoint was time to rescue therapy relative to the date of the first of two quarterly treatments in PEACHTREE. Other endpoints related to efficacy included changes from baseline BCVA as measured by ETDRS letters read, changes from the baseline central subfield thickness (CST) measured by spectral domain optical coherence tomography, changes from baseline in signs of uveitis, as evaluated by the Standardization of Uveitis Nomenclature criteria (resolution of inflammation to a score of 0) for anterior chamber cells, anterior chamber flare and vitreous haze.4
Rescue therapy
If at any time during the study any of the following criteria were met in the study eye, rescue therapy was to be administered: loss of 10 letters or more in BCVA relative to previous two visits due to uveitis, CST of >320 µm, increase in CST from either of the previous two visits consisting of either ≥20% or ≥100 µm, or if, in the investigator’s medical judgement, the uveitic complications in the study eye had not improved and the conditions needed to be addressed. The specific rescue therapy implemented was left to the discretion of the investigator.3
Safety endpoint assessments
The safety population included all enrolled patients at the selected MAGNOLIA sites who successfully completed the crossover visit. In terms of safety, endpoints included the incidences of TEAEs, on-study AEs and SAEs. TEAEs were defined as any event that occurred post treatment in PEACHTREE or, if pre-existing, worsened after day 0 in MAGNOLIA. On-study AEs were defined as TEAEs that started on or after the crossover visit. Additional on-study endpoints included the percentage of patients with a change in IOP value ≥10 mm Hg from their own PEACHTREE baseline measurement, the percentage of patients with an observed IOP reading ≥30 mm Hg and the percentage of patients who required one or more additional IOP lowering medications following a clinically significant IOP elevation (≥10 mm Hg).
Statistical analysis
With respect to statistical power, based on a binomial distribution, a sample size of 30 subjects was chosen to provide an 80% probability of detecting at least two subjects with an IOP >25 mm Hg over the 24-week follow-up period if the true incidence was 10%. All data were summarised based on the safety population, which included all enrolled patients who successfully completed the crossover visit (day 0). Patients in the safety population were analysed according to their treatment arm in PEACHTREE. Baseline was defined as the measurement taken in PEACHTREE prior to administration of any study drug. Descriptive statistics were used to summarise continuous variables, while counts and percentages were used to summarise categorical variables.
The primary endpoint for MAGNOLIA was the time to rescue, defined as the number of days between the date of the first injection of study drug in PEACHTREE to the date of administration of rescue medication in the study eye during MAGNOLIA. Patients not receiving rescue were assigned a censored time to rescue equal to the total number of days follow-up at study exit. The number of patients who received rescue, and the time to rescue in days, were summarised by Kaplan-Meier (KM) survival analysis methods. Median time to rescue for each study arm was calculated. A log rank test was used to test for a difference between the KM survival curve distributions. Using data from PEACHTREE and MAGNOLIA, time to rescue from those patients enrolling into MAGNOLIA (48 weeks of follow-up maximum) were combined with the time to rescue from those patients who did not enroll into MAGNOLIA (24 weeks of follow-up maximum), in order to assess probability of rescue over the entire 48-week period. As KM analysis yields a survival function from the number of events and number of people at risk at each timepoint, it takes into account drop out or ‘right censored data’. The survival function between each timepoint’s observation is assumed to be constant. Consequently, if the patients in MAGNOLIA do not differ from those who did not participate in MAGNOLIA, then those who did not participate are treated as censored data at the time of exiting from PEACHTREE. In this post-hoc analysis, time to rescue was defined as the number of days between the date of the last injection of study drug in PEACHTREE (patients in PEACHTREE receiving rescue prior to the week 12 visit were not administered the second dose of study drug) to the date of administration of rescue medication in the study eye during PEACHTREE or MAGNOLIA. The number of patients who received rescue and the time to rescue in days were summarised using the same KM methods as described above. Time to rescue were plotted using the KM survival method.
With respect to functional and anatomic endpoints, mean changes from baseline in BCVA and CST were tested post hoc against a null hypothesis of no difference from zero using a one-sample t-test. Two-sided significance tests were used throughout, and a type 1 error rate of 0.050 was used in evaluating statistical significance.
With respect to safety, for all patients participating in MAGNOLIA, AE data collected in PEACHTREE and for MAGNOLIA were included in the analysis, as noted above. TEAEs were defined as any event occurring post treatment in PEACHTREE or, if pre-existing, worsening after day 0 in MAGNOLIA. The incidence of TEAEs, including cataracts, were summarised by MedDRA system organ class and preferred term. The incidence of endpoints based on the assessment of IOP during the MAGNOLIA extension study were summarised. IOP lowering medications were enumerated in those patients experiencing a clinically significant increase in IOP during the MAGNOLIA extension study.
Results
Baseline patient characteristics
The 22 sites participating in MAGNOLIA enrolled a total of 54 patients to the CLS-TA arm and 32 patients to the control arm of PEACHTREE. Forty-six CLS-TA patients from these 22 sites completed PEACHTREE without receiving rescue therapy (39 CLS-TA patients and 7 control patients) and were eligible to participate in the MAGNOLIA extension study; 28 of these 39 CLS-TA patients were enrolled. Although the primary objective of MAGNOLIA was to evaluate the efficacy of CLS-TA, five of seven eligible control patients from PEACHTREE were enrolled, because MAGNOLIA was initiated prior to the completion of PEACHTREE and the unmasking of the randomisation schedule.
Table 1 summarises patient demographics and baseline disease characteristics. Mean age at baseline was 49 years (range: 19–78 years), and 18 of the 33 patients were male (54.5%).Table 1 Anatomic location of uveitis in the study eye was classified as anterior uveitis (33.3%), intermediate uveitis (27.3%), posterior uveitis (36.4%) or panuveitis (21.2%), with some patients being included into more than one classification. Most cases of uveitis in the study eye were idiopathic in nature (84.8%), persistent in duration (84.8%) and chronic in development (63.6%). Fourteen CLS-TA and 2 control patients completed the week 48 assessment of MAGNOLIA without rescue therapy. For discontinued patients, the most common reason was need for rescue therapy.
Demographics and baseline disease characteristics
For the 28 patients in the CLS-TA arm enrolled in MAGNOLIA, mean BCVA in the study eye was 55.1 letters (20/80 Snellen approximation) at the PEACHTREE baseline and 71.9 letters (20/40 Snellen approximation) at the crossover visit. All patients were diagnosed with ME at PEACHTREE baseline, with an average duration of 55.5 weeks. For the 28 patients in the CLS-TA arm enrolled in MAGNOLIA, the mean CST in the study eye was 470.6 µm at the PEACHTREE baseline and 292.5 µm at the crossover visit. The baseline mean BCVA and mean CST at crossover was comparable to the overall PEACHTREE population. The CLS-TA and control arms had baseline mean BCVA of 54.7 letters and 53.5 letters and mean CST of 480.9 µm and 525.4 µm, respectively.
To assess for selection bias, among participating centres, CLS-TA patients who enrolled in MAGNOLIA were compared with those CLS-TA patients who did not enroll. There were no substantial differences identified in the baseline characteristics or efficacy and safety outcomes of those who did or did not enroll in MAGNOLIA. Most importantly, eligible subjects from the participating sites who enrolled compared with those who did not enroll, respectively, showed similar age (48.57 vs 48.83 years), gender (50%:50% vs 33.3%:66.7% male:female), uveitis aetiology (89.3% vs 77.9% idiopathic), pretreatment BCVA (55.1 vs 55.1 letters, p=0.999), BCVA at MAGNOLIA enrollment (71.9 vs 72.9 letters, p=0.788), pretreatment CST (470.6 vs 477.6 µm, p=0.873) and CST at MAGNOLIA enrollment (292.5 vs 287.6 µm, p=0.792).
Efficacy
Of the 28 CLS-TA patients, a total of 11 (39.3%) received rescue during MAGNOLIA and 3 were discontinued from the study due to AE. In the control group, three patients (60%) received rescue during MAGNOLIA, and two patients completed the study.
Based on the KM analysis of median time to rescue, patients in MAGNOLIA were similar between CLS-TA and control arms (344.0 days vs 332.0 days, respectively), with a lower proportion of patients in the CLS-TA arm (11/28 patients, 39.3%) receiving rescue during the 24-week follow-up period of MAGNOLIA compared with 3/5 patients (60.0%) in the control arm. This difference was not statistically significant (p=0.562).
In order to assess probability of rescue over the entire 48-week period, the KM analysis included patients enrolled into MAGNOLIA (weeks 24–48, n=33 patients) and those not enrolled into MAGNOLIA (PEACHTREE baseline to week 24, n=127 patients). This analysis demonstrated that median time to use of rescue medication relative to the last dose of study drug was longer in the CLS-TA arm compared with the control arm (257.0 days vs 55.5 days, respectively), and the survival time distribution curves were statistically significantly different (p<0.001) (figure 1).

Kaplan-Meier survival plot of the time to rescue medication. Error bars represent 95% CIs. Log rank test: p<0.001. CLS-TA, triamcinolone acetonide injectable suspension.
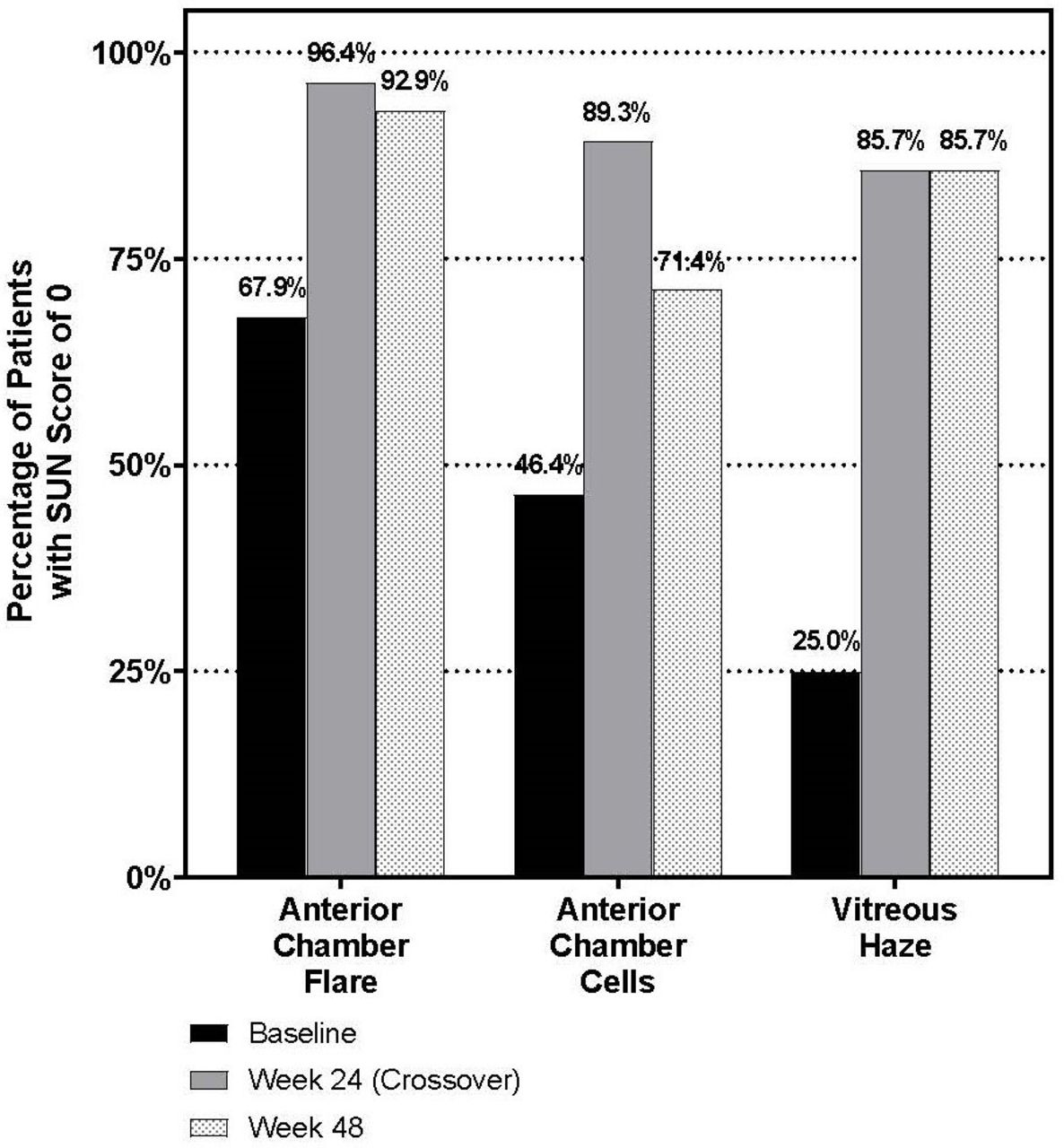
BCVA and CST results showed little change over time in patients who were enrolled into MAGNOLIA. In CLS-TA patients, a mean gain of 16.8 letters at the crossover visit (p<0.001) and 12.1 letters at week 48 (p=0.004) were noted, as shown in figure 2; mean CST reduction was 178.1 µm at the crossover visit (p<0.001) and 174.5 µm at week 48 (p=0.001), as shown in figure 2. Figure 3 shows the percentage of patients with scores of 0 for anterior chamber flare, anterior chamber cells and vitreous haze at baseline, week 24 and week 48. This summary includes only patients not receiving rescue therapy and demonstrates a trend in improvement between baseline and week 24, with stability for anterior chamber flare and vitreous haze between week 24 and week 48.
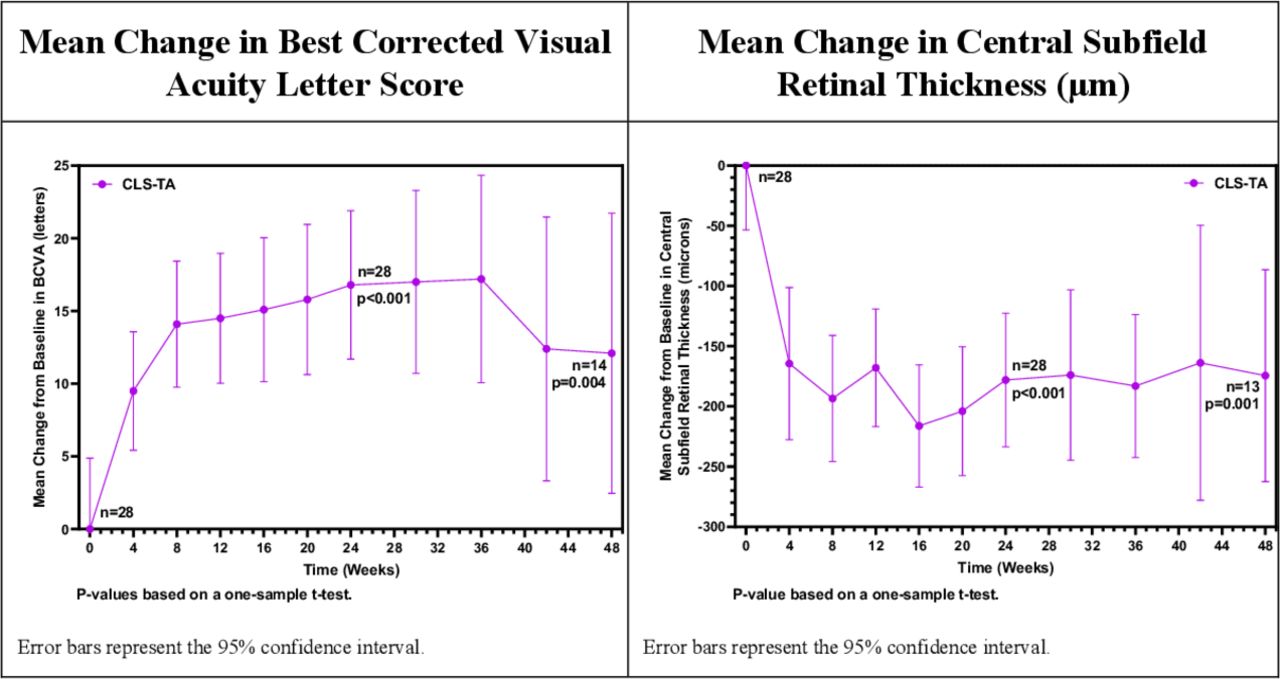
Mean change from baseline in best corrected visual acuity letter score and mean change from baseline in central subfield retinal thickness (µm). Error bars represent 95% CIs. 13/14 patients completing the study had gradable optical coherence tomography images.

{kind=link}
{kind=link}
{kind=link}
Percentage of patients with Standardization of Uveitis Nomenclature scores of 0 for anterior chamber flare, anterior chamber cells and vitreous haze at baseline, week 24 (crossover) and week 48.
Safety
TEAEs over the 48-week period encompassing both PEACHTREE and MAGNOLIA are summarised in table 2. Overall, 21 patients (63.6%) had at least 1 ocular TEAE in the study eye (64.3%, CLS-TA; 60.0%, control) and 5 patients (15.2%) had at least 1 non-ocular TEAE (14.3%, CLS-TA; 20.0%, control). One (3.0%) patient (CLS-TA arm) had 10 non-ocular SAEs over the 48 weeks of follow-up. No deaths occurred during either study. Nineteen MAGNOLIA patients (57.6%) had at least 1 ocular on-study AE in the study eye (57.1%, CLS-TA; 60.0%, control) and 3 (9.1%) patients had at least 1 non-ocular on-study AE (7.1%, CLS-TA; 20.0%, control). Subcapsular cataract was the most frequently reported on-study AE in the study eye.
TEAEs, over 48 weeks
In the CLS-TA arm, 4 patients (14.3%) had at least 1 IOP assessment that was an increase from baseline ≥10 mm Hg in the study eye during MAGNOLIA (vs 0% in the control arm). One patient experienced an IOP increase for the first time during MAGNOLIA while the other three patients experienced an IOP increase during PEACHTREE that persisted during MAGNOLIA. Two patients in the CLS-TA arm had an absolute IOP ≥25 mm Hg in the study eye, and 1 patient had an absolute IOP ≥30 mm Hg; no patients had an absolute IOP ≥35 mm Hg. One patient had an IOP assessment of 32 mm Hg 12 weeks into MAGNOLIA prompting the investigator to report a TEAE that was considered unrelated to study treatment. No other cases resulted in the investigator reporting IOP elevation as a TEAE.
Two (7.1%) patients in the CLS-TA arm were receiving IOP-lowering medication at the crossover visit, day 0, of MAGNOLIA following a clinically significant increase in IOP ≥10 mm Hg. Separately, one patient (3.6%) required an IOP-lowering medication during MAGNOLIA, after the crossover visit. None of the patients in the control arm required additional IOP-lowering medications. No patients, in either arm, underwent surgery for elevated IOP.
A total of 8 patients, 7 (25.0%) in the CLS-TA arm and 1 (20.0%) in the control arm, had a TEAE related to cataract in the study eye during the 48 weeks of follow-up. Four of the cataract-related TEAEs were reported during MAGNOLIA. Two patients in the CLS-TA arm required surgery in the study eye for cataract; outcomes included the expected improvement in visual acuity, CST remaining improved versus baseline and no significant increases in signs of inflammation.
Discussion
In preclinical studies, suprachoroidally delivered CLS-TA rapidly achieved high levels of drug in the choroid and retina with multi-month durability,1 2 which could partially account for the statistically significant and clinically meaningful functional and anatomic improvements in patients with ME due to NIU. Overall, the efficacy and safety results of the 24-week MAGNOLIA extension study in selected sites support the findings of PEACHTREE and indicate that the efficacy and safety profiles of CLS-TA were maintained in 50% of these patients for up to 9 months following CLS-TA treatment during PEACHTREE.
With respect to safety, when used to treat uveitic ME, suprachoroidal delivery of CLS-TA may impact IOP to a lesser extent compared with intravitreal corticosteroids. Cross trial comparisons are problematic due to differing designs, but the recent PeriOcular and INTravitreal Corticosteroids for Uveitic Macular Oedema Trial (POINT)5 study (NCT02374060), an NIH-funded prospective clinical trial, provides some context. This study compared three commonly administered local corticosteroids for uveitic ME. The 6-month results reported rates of IOP elevation (IOP increase >10 mm Hg) with the use of intravitreal triamcinolone acetonide was 26%,5 compared with the 14.3% rate observed at the conclusion of MAGNOLIA. In the POINT study, approximately 24%–33% of patients in each arm required IOP-lowering medication, versus 10.7% of patients by the conclusion of MAGNOLIA. Likewise, cataract AEs in MAGNOLIA occurred at an acceptable rate and compare favourably to other intravitreal corticosteroids assessed over a similar time period (YUTIQ fluocinolone acetonide intravitreal implant prescribing information). These IOP and cataract data support the unique compartmentalisation and ocular distribution inherent to the suprachoroidal administration of CLS-TA. Preclinical studies investigating suprachoroidal administration support this assertion, demonstrating low corticosteroid exposure within the anterior chamber and trabecular meshwork.2 6
Limitations of this trial include its small sample size, due in part to the limited number of sites selected to participate and its design, which included only those patients not receiving rescue medication during PEACHTREE. In addition, the small sample size precludes complete long-term assessment of safety. Also, the date of the first masked study treatment administration was used as the starting point for time to rescue, rather than the last administration of study drug. Site selection also favoured those with the highest enrollment and patients with ongoing follow-up. However, among participating centres, patients who enrolled in MAGNOLIA showed no substantial differences from those who did not enroll, with respect to the baseline characteristics or efficacy and safety outcomes after receiving the two PEACHTREE protocol-mandated CLS-TA treatments. These lack of differences also support the cross-study KM survival analysis of rescue therapy, which assessed the number of patients at risk at each timepoint, appropriately accounting for those who did not participate as censored data. Overall, PEACHTREE and MAGNOLIA support suprachoroidal CLS-TA as a new treatment option for patients with ME associated with NIU These results also suggest that suprachoroidal administration could enhance delivery of therapies for a variety of ophthalmic conditions, in which anatomically precise drug delivery may yield safety, efficacy and durability benefits over current therapies.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. This study was an extension of the PEACHTREE phase 3 clinical trial, and additional relevant information can be found in that publication, which can be found here: https://doi.org/10.1016/j.ophtha.2020.01.006.
Ethics statements
Patient consent for publication
Footnotes
Twitter @ThomasCiullaMD
Contributors The investigators collected the data, and the sponsor conducted the data analyses. All authors had full access to the data; there was an agreement between the investigators and the sponsor to not disclose any trial information that was not publicly available. All authors reviewed and provided feedback on the manuscript drafts and made the decision to submit the manuscript for publication; the sponsor also reviewed and approved the manuscript. All authors vouch for the completeness and accuracy of the data and analyses and affirm that the trial was conducted and reported with fidelity to the protocol.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests RNK reports receiving consulting fees from Allergan, Genentech and Regeneron. He also reports receiving grant support from Allergan, Chengdu Kanghong, Clearside Biomedical, Roche and Santen. PM reports receiving consulting fees from Eyepoint, Alimera and Allergan. She also reports receiving grant support from Clearside, Gilead, Santen and NEI. SY reports receiving consulting fees from Clearside Biomedical and Santen. He also reports receiving grant support from Bayer. ES reports receiving consulting fees from Clearside Biomedical, Abbvie, Eyegate, Eyepoint and Gilead. He also reports receiving grant support from Aldeyra. MRB reports receiving consulting fees from Allegro, Allergan, Alimera, Bausch and Lomb, Genentech, Novartis and Regenxbio. EU reports receiving consulting fees from Abbvie, Novartis, Eyepoint, Regeneron, GlaxoSmithKline and Bausch and Lomb. He also reports receiving grant support from Novartis and Roche/Genentech. CRH reports receiving consulting fees from Clearside Biomedical. MS reports receiving grant support from Clearside Biomedical. RCW has nothing to disclose. TC and BK are employees of Clearside Biomedical and hold stock in Clearside Biomedical.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance