Article Text

Abstract
Aim: To determine the prevalence and identify associated risk factors for dry eye syndrome in a population in Sumatra, Indonesia.
Methods: A one stage cluster sampling procedure was conducted to randomly select 100 households in each of the five rural villages and one provincial town of the Riau province, Indonesia, from April to June 2001. Interviewers collected demographic, lifestyle, and medical data from 1058 participants aged 21 years or over. Symptoms of dry eye were assessed using a six item validated questionnaire. Presence of one or more of the six dry eye symptoms often or all the time was analysed. Presence of pterygium was documented.
Results: Prevalence of one or more of the six dry eye symptoms often or all the time adjusted for age was 27.5% (95% confidence interval (CI) 24.8 to 30.2). After adjusting for all significant variables, independent risk factors for dry eye were pterygium (p<0.001, multivariate odds ratio (OR) 1.8; 95% CI 1.4 to 2.5) and a history of current cigarette smoking (p=0.05, multivariate OR 1.5; 95% CI 1.0 to 2.2).
Conclusions: This population based study provides prevalence rates of dry eye symptoms in a tropical developing nation. From our findings, pterygium is a possible independent risk factor for dry eye symptoms.
- dry eye symptoms
- pterygium
- smoking
- population based study
Statistics from Altmetric.com
Dry eye represents a multifactorial, heterogeneous disorder of the preocular tear film, which results in ocular surface disease. The tear film and ocular surface form a complex and stable system that can lose its equilibrium through numerous disturbing factors.1
Reduction in quality of life is inevitable when symptoms of dry eye occur. These symptoms range from mild transient irritation to persistent dryness, burning, itchiness, redness, pain, ocular fatigue and visual disturbance. In the United States alone, approximately 7–10 million Americans require artificial tear preparations, with consumers spending over $100 million/year.2
Reported prevalence of dry eye is diverse, with questionnaire based surveys documenting rates ranging from 14.4% to 33% of the population sampled.3–6 Studies which also involve tests of tear function including Schirmer’s test, tear break up time, fluorescein staining, or rose bengal staining for determination of dry eye have found generally lower prevalence rates.6,7 Limitations in comparisons of studies in different populations include different age distribution of the population, definitions of dry eye, or methodology. Most studies of dry eye are confined to developed nations and older populations, with resultant lack of ethnic diversity.5–8
We aimed therefore to report the prevalence of dry eye symptoms in Sumatra, Indonesia, and to identify possible associated risk factors.
MATERIALS AND METHODS
Study population
A large population based prevalence survey of general health, respiratory symptoms, and vision was conducted in five rural villages (Kuala Terusan Baru, Pelalawan, Delik, SP7, and Segati) and one provincial town (Pangkalan Kerinci) of the Riau province, Sumatra, Indonesia, in people 21 years or older during the period April to June 2001. The region of study was District Pelalawan, a tropical area with secondary forests near the Kampar river and the nearest large city is the capital of the Riau province, Pekan Baru.
All houses in each village were individually mapped and assigned a number by an enumeration team. A one stage cluster sampling procedure was conducted whereby 100 households (as there were only a total of 60 households in Delik, all 60 were assessed) were randomly selected from a sampling frame of the total number of households in each village. Of these, 216 subjects recruited from Kerinci, 231 subjects from Kuala Terusan Baru, 229 from Pelalawan, 120 from Delik, 233 from SP7, and 181 from Segati were above 21 years of age (total = 1210). Non-contactables were defined as individuals who were not contactable on three occasions and refusals defined as individuals who declined to participate in the study.
Training of team members and a pilot study of 16 subjects in SP7 were conducted in April 2001, 2 weeks before the survey proper. Before the examinations, meetings were held with the village leaders to explain the purpose of the study and to obtain cooperation from the community. Informed verbal consent was obtained from the subjects and all subjects were treated in accordance with the tenets of the Declaration of Helsinki. Approval for the study was obtained from the ethics committee, Singapore Eye Research Institute.
Questionnaire
A validated six item questionnaire of ocular symptoms relating to dry eye was used9,10 which included the following questions (1) Do your eyes ever feel dry? (2) Do you ever feel a gritty or sandy sensation in your eye? (3) Do your eyes ever have a burning sensation? (4) Are your eyes ever red? (5) Do you notice much crusting on your lashes? and (6) Do your eyes ever get stuck shut?
Presence of a symptom from the dry eye questionnaire was further graded as rarely (at least once in 3–4 months), sometimes (once in 2–4 weeks), often (at least once a week), or all the time. Information about sex, age, current occupation, current cigarette smoking status, and household fuel use was also collected. Main occupational groups were classified as agricultural (fishermen, farmers, rubber tappers, wood collectors), factory workers, homemakers, and others (students, shop keepers, and office workers). Primary fuel used for cooking was divided into gas/kerosene and charcoal/firewood categories.
The questionnaire was translated to Bahasa Indonesia and back translated to English for checking. Trained interviewers administered the questionnaire. Pilot testing showed that the questionnaire was understandable, easily administered, and socioculturally acceptable.
Eye examinations
Pterygium was examined for in those 21 years or above. It was defined as an interpalpebral radially orientated fibrovascular lesion crossing the nasal or temporal limbus.11 Autorefraction measurements in the right and left eye were performed using one of two hand held autorefractors, the Retinomax K-plus (Nikon, Tokyo, Japan).12,13 The team members performing the eye examinations were masked to dry eye information from the questionnaire.
Data analysis
The prevalence rates and 95% confidence intervals (95% CI) of dry eye symptoms using these definitions for subjects with different characteristics were calculated, allowing for clustering. Age adjusted prevalence rates were derived using the Indonesia 1990 census population as the reference standard. For subsequent statistical analysis, one or more of the six dry eye symptoms reported often or all the time was positive.10
The crude and multivariate OR with 95% CI were calculated using logistic regression, denoting the associations between the various lifestyle variables, and one or more of the six dry eye symptoms reported often or all the time. Multivariate adjusted odds ratios were obtained from multiple logistic regression models, allowing for clustering. In these analyses, age was a continuous variable. All statistical analyses were performed using the commercially available software stata version 7.0.14 A p value of <0.05 was considered statistically significant.
RESULTS
Participant characteristics
Of the randomly selected 1251 participants, 1058 (553 women and 505 men) completed the dry eye questionnaire. The overall participation response rate was 84.6%. The mean age was 37.0 (SD 13.0) years. The mean age of the men was 38.4 (13.2) years and of the women, 35.8 (12.7) years. The median age of the participants (34.0 years) and non-participants (33.0 years) was not significantly different (p=0.21). All participants were of Indonesian extraction.
Symptom frequency
Figure 1 represents the distribution of each dry eye symptom by frequency of response (never, rarely, sometimes, often, or all the time), in participants of this survey. Participants complained of any sensation (rarely, sometimes, often, or all the time) of burning most often (59.1% of subjects). Severe symptoms of grittiness (0.9% of subjects) and of red eyes (0.9%) were reported most frequently compared with the other dry eye symptoms. Frequency of response for each symptom is inversely correlated with increased persistence of that symptom.

Frequency of dry eye symptoms (dryness, grittiness, burning, redness, crusting, and eyes stuck shut) in the population (n=1058 for each symptom).
Number of symptoms
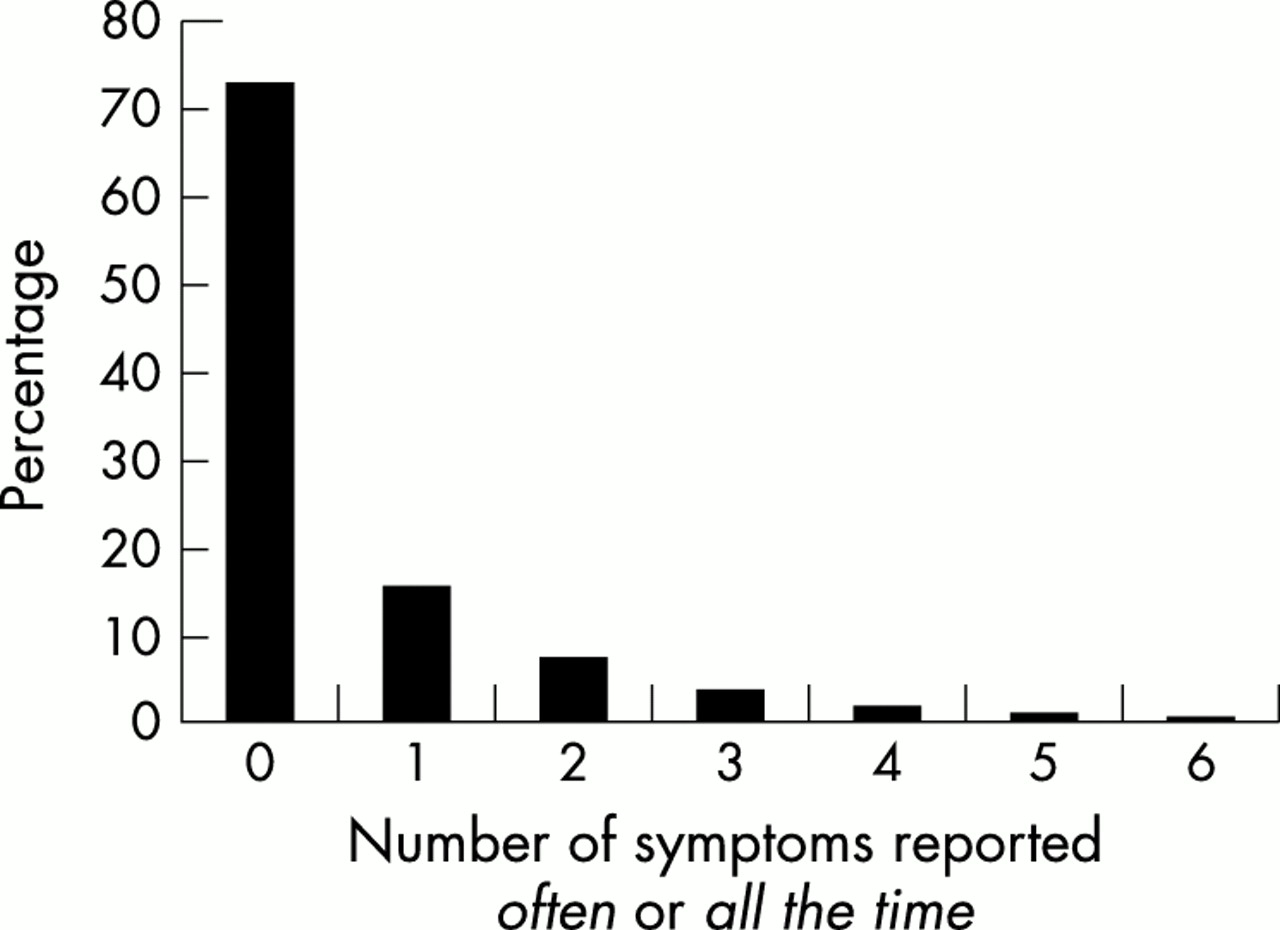
Figure 2 illustrates the distribution of the number of symptoms reported as often or all the time by a participant; 15.4%, 6.9%, 3.3%, 1.3%, 0.5%, and 0.1% of the participants reported 1, 2, 3, 4, 5, and 6 of the six dry eye symptoms often or all the time respectively. Thus, 27.5% of subjects reported at least one of the six dry eye symptoms often or all the time.
{kind=link}
{kind=link}
Number of symptoms reported as often or all the time (n=1058).
Prevalence of dry eye symptoms by age and sex
The crude prevalence rate of one or more of the six dry eye symptoms reported often or all the time was 27.5% (95% CI 24.6 to 30.4) (Table 1). Age adjusted prevalence rates to the Indonesia 1990 census population was similar. The 40–49 year age group reported most dry eye symptoms (37.6%), although a significant increase in dry eye symptoms was found with increasing age (p for trend <0.001). The prevalence of dry eye was 1.4 times higher for men than for women.
Prevalence rates of one or more of the six dry eye symptoms present often or all the time in six villages in Sumatra, Indonesia (n=1058)
Risk factors for dry eye
The risk factors found to be associated with one or more of the six dry eye symptoms often or all the time are shown in Table 2. A multivariate logistic regression model with dry eye symptoms as the outcome and sex, age, occupation, smoking, and pterygia as the covariates was conducted. Pterygium in either eye was significantly associated with one or more of the six dry eye symptoms often or all the time after adjusting for other correlates (p<0.001, OR 1.9; 95%CI 1.4 to 2.6). A borderline association was found between dry eye symptoms and current smoking history (p=0.051, multivariate adjusted OR 1.5; 95% CI 1.0 to 2.2).
Age and multivariate adjusted odds ratios (95% confidence intervals) for associations between sex, age, occupation, smoking history, and pterygium, and presence of one or more of the six dry eye symptoms present often or all the time
The crude odds ratio for the association between dry eye symptoms and increasing age (p<0.001, OR 1.02; 95% CI 1.00 to 1.03) was significant. However, after multivariate adjustment, a borderline association with age remained (p=0.069, OR 1.01; 95% CI 0.99 to 1.01). A protective effect of female sex (p<0.001, OR 0.6; 95%CI 0.5 to 0.8) and occupation as homemakers (p=0.007, OR 0.6; 95%CI 0.4 to 0.9) was found in relation to dry eye symptoms. These relations did not remain significant after multivariate adjustment.
Occupations in either agricultural or industrial areas were not associated with the risk of dry eye symptoms, nor did the use of various types of household fuel or history of passive smoking in the home. Refractive error, whether myopia (spherical equivalent at least −0.5 dioptre) (p=0.806) or hyperopia (spherical equivalent great than +0.5 dioptre) (p = 0.307), was not significantly associated with one or more of the six dry eye symptoms often or all the time.
DISCUSSION
This population based study in a developing nation has found that the age adjusted prevalence of one or more of the six dry eye symptoms often or all the time was 27.5%. Dry eye symptoms increased with age, male sex, current smoking history, and presence of pterygium. After adjusting for confounders, pterygium and current smoking history were found to be independently associated with dry eye symptoms.
Population based studies evaluating dry eye differ in the choice of dry eye questionnaire and objective tests, definitions of dry eye and the selection of the study population. Comparisons between the studies are thus difficult (see Table 3). The Salisbury Eye Evaluation study (SEE Study),6 utilising the same validated questionnaire to evaluate and define dry eye symptoms, found 14% of participants reported one or more of the six dry eye symptoms often or all the time. Dry eye prevalence decreased to 2.0% when rose bengal tests were added.6 Although the participants of the SEE study were 65 years or over, the prevalence of dry eye symptoms in our subjects 60 years or over was still twice as high (30.0%). Possible explanations for prevalence differences include ethnic extraction (15% blacks, majority whites), participation rates (98.5% for the SEE Study v 84.6% for our study), and environmental conditions. As our study was conducted in Indonesia, an equatorial region, increased sunlight exposure and ambient temperature may increase the frequency of dry eye symptoms, whereas high humidity could be protective.
Population based studies on dry eye alone
In the Beaver Dam Study,5 dry eye was defined as a positive response to the question: “For the past 3 months or longer have you had dry eyes?” with further prompting: “foreign body sensation, with itching burning, sandy feeling, not related to allergy?” if required. They found an overall prevalence of dry eye of 14.4%. In a study conducted in Melbourne, Australia,7 5.5% of subjects reported any severe symptom of dry eye including discomfort, foreign body sensation, tearing, dryness, or photophobia and 10.8% by rose bengal staining.
Other studies using self administered questionnaires to determine dry eye have found generally similar rates (28.7% for the Canadian Dry Eye Epidemiology Study (CANDEES)3 and 33% for a Japanese population based study4). In these studies, poorer response rates (15.6% for CANDEES and 23% for the Japanese study) and the use of self administered questionnaires would have contributed to selection and reporting bias respectively. However, the demographics of the Japanese study4 resemble our own with the mean age being 35.2 years and the participants being predominantly Asian.
Increased age and dry eye has been demonstrated previously5,7 although Schein et al10 found no age correlation to exist. In our study an association with age was found on univariate analysis, but was not significant after adjustment for all other variables. Although dry eye is thought to be more prevalent in women3,5,7,15,16 compared with men, we did not find any sex differences in the prevalence of dry eye in our study. Deficient tear secretion from oestrogen deficiency in menopausal women has been hypothesised to explain sex differences, although studies have found that women on hormone replacement therapy may have an increased risk of dry eye.16,17
Dry eye symptoms in our population were around 1.5 times more prevalent in current cigarette smokers than non-smokers, with borderline significance after multivariate adjustment. The Beaver Dam Eye Study,5 which first reported cigarette smoking as a risk factor for dry eye, found a 1.4 times increase in dry eye in current cigarette smokers. They proposed that cigarette smoke acts as a direct irritant in the eyes, and represents a modifiable risk factor for dry eye.
We found a twofold increased risk of dry eye symptoms in participants with pterygium. A recent case-control study18 has found an association between pterygium and a shortened tear break up time and Schirmer’s test, and a decreased tear function index.18 Although these findings are supported by an earlier study,19 conflicting results have also been documented.20–22 Proposed mechanisms include pathological conjunctival, corneal, or eyelid changes in pterygia leading to disturbed tear film function1 or, conversely, an unstable tear film in dry eye contributing to the initiation of pterygium.18 Pterygium may possibly be a distant surrogate for the environmental factors associated with dry eye, such as ultraviolet light quantities and dusty polluted environment of outdoor work, which have also been implicated in pterygium formation.23
Strengths of our study include use of a six item questionnaire to determine dry eye symptoms designed and validated in a large population based study in Salisbury, Maryland, United States.1,6,10,24 Trained interviewers administered this questionnaire to reduce reporting bias. In accordance with studies using this six item dry eye questionnaire,6,11 subjects who experienced symptoms were categorised by similar symptom patterns and by frequency of symptom occurrence, reportedly better than calculating severity scores alone.9 As alleviation of dry eye symptoms is of primary importance in dry eye treatment,9,25,26 identification of dry eye symptoms can be regarded to be as important as dry eye tests.
The main limitation of our study is that it lacks objective dry eye tests because local sociocultural sensitivities precluded an interventional study. Objective studies of dry eye commonly involve Schirmer’s test, rose bengal staining, and tear break up time; however, these tests lack sensitivity and underestimate dry eye compared with self reported symptoms.5,7,10 Moreover, fluorescein itself can reduce the break up time of tear film19 and individuals can test positive for rose bengal and Schirmer’s tests without having symptoms of dry eye.4
Also, documented risk factors of dry eye such as arthritis, caffeine use, thyroid disease, gout, total to high density lipoprotein cholesterol ratio, diabetes, and multivitamin use5 were not investigated in this study.
Consensus on the most appropriate diagnostic criteria, role of subjective assessment, and interpretation of results has not yet been reached.25 Although a diagnostic set of dry eye features include dry eye symptoms, ocular surface damage, reduced tear stability, and tear hyperosmolarity, these features cannot be equated to aetiology.25,27 Dry eye has been defined by two mutually exclusive and functionally diverse categories: tear deficient and evaporative dry eye.25,27 It is increasingly recognised that the correlation between subjective and clinical findings is poor,10,7,15 and could be due to the multifactorial nature of dry eye problems.25 Thus, a well designed and validated questionnaire to evaluate symptoms of dry eye and functional lifestyle has been advocated as the best method to determine clinical efficacy of dry eye treatment.25
CONCLUSION
Our prevalence survey of dry eye in a developing country in South East Asia has been valuable in identifying several relevant factors. We have shown that dry eye occurs in indigenous populations residing in Indonesia, previously anecdotal in nature, and that the prevalence rate of one or more of the six dry eye symptoms often or all the time was 27.5%, almost two times higher than expected compared with other communities. Increased odds for dry eye were found in current cigarette smokers, and a positive association in subjects with pterygium. Further studies evaluating the use of dry eye treatment in this population would be of value.
Acknowledgments
This project was funded by the SERI grant (R 209/01/2001-PG) and the National Medical Research Council (NMRC), SERI/MG/97-04/0005, Singapore. We would like to thank the staff of PT Riau Andalan Pulp and Paper and Yayasan Putra Bangsa, Indonesia. We would also like to express special thanks to the Indonesia health survey team (team leaders were Nimit Nico and Juwendi Jamal) and the myopia team, especially Anwar, Zakaria, Darneli, and Said. We thank Angela Cheng, National University of Singapore, for assistance in data collection and management.
Commercial interests: None.
REFERENCES
Footnotes
Series editors: W V Good and S Ruit