Article Text

Abstract
Purpose To evaluate the long-term outcome of autologous graft of retinal pigment epithelium (RPE) in patients with geographic atrophy.
Methods Ten patients with progressive geographic atrophy underwent translocation of an autologous graft of RPE, Bruch membrane and choroid. The visual acuity (VA), reading performance, microperimetry, optical coherence tomography (OCT), fundus autofluorescence, fluorescein angiography and indocyanine green angiography were assessed.
Results No recurrence of RPE atrophy was seen. All but one transplant were revascularised. Vascularisation persisted throughout the 3 years' follow-up. Spectral-domain OCT in some cases showed intact photoreceptors or intact outer nuclear and outer plexiform layer overlying the graft. In three cases, the grafts were positioned eccentrically; these patients did not benefit from surgery. The mean VA decreased from 20/80 (range: 20/800 to 20/40) at baseline to 20/200 (range: perception of hand movements to 20/32) at last follow-up. In two patients, VA were stable from 20/50 to 20/32 and 20/40 at the last follow-up, respectively. Postoperative complications included retinal detachment due to proliferative vitreoretinopathy, macular pucker, iritis, branch retinal vein occlusion and secondary ocular hypertension.
Conclusions Some patients benefit for at least 3 years from a functioning RPE-choroid graft. Functional outcome in most patients, however, was limited due to complications and unfavourable patient selection.
- Age-related macular degeneration
- geographic atrophy
- retinal pigment epithelium
- treatment surgery
- retina
- macula
- choroid
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
- Age-related macular degeneration
- geographic atrophy
- retinal pigment epithelium
- treatment surgery
- retina
- macula
- choroid
Introduction
Geographic atrophy accounts for severe vision loss and blindness in about 40% of the patients with age-related macular degeneration (AMD).1 Therapeutic approaches are limited to vitamin supplementation and modifications of rheological parameters to slow down the progression of the disease. To date, there are no therapeutic strategies to stabilise or improve visual acuity.
Full macular translocation, a surgical approach to geographic atrophy, is usually complicated by rapid onset of RPE atrophy at the new location of the macula. Other strategies that inject suspensions of viable pigment epithelial cells (autologous iris pigment epithelium) into the submacular space have also failed possibly because the individualised cells did not reattach.2 Sheets of autologous retinal pigment epithelium (RPE), Bruch membrane, and choroid (patch transplants) have been successfully applied for exudative AMD with promising functional outcome similar to the results after full macular translocation.3–7
In a previous study with a relatively short-term follow-up period, autofluorescence was found to be present in patch transplants, and central visual acuity was maintained in patients with geographic atrophy over 6–12 months.8 In the present study, we examined the long-term outcome to rule out rapid onset of RPE atrophy as reported to occur within 1 year after full macular translocation.9 10
Methods
Patients
In this prospective, non-randomised case series, 10 patients with geographic atrophy secondary to AMD were included. All patients had recently (within 3 months) experienced visual loss caused by progressive RPE atrophy. This study was approved by the Ethics Committee of the Medical Faculty at the University of Cologne and was conducted in accordance with the Declaration of Helsinki. All patients were informed about the experimental nature and potential benefit and complications of the surgical procedure. A written informed consent was obtained from each patient prior to surgery.
Measurements
Patients were examined at baseline, at 6 months and at ≥2–3 years after surgery to evaluate the functional and anatomical outcome. The best-corrected visual acuity (VA) was measured using the Early Treatment of Diabetes Retinopathy Study (ETDRS) protocol, and the reading performance was assessed using Radner reading charts.11 Fixation and retinal sensitivity for light stimuli were tested using microperimetry (scanning laser ophthalmoscope, Rodenstock, Munich, Germany, and MP1 microperimeter, Nidek Technologies, Padua, Italy). Colour fundus photography (Canon CF-60 DSi, digital fundus camera, Canon, Haag-Streit Deutschland GmbH, Wedel, Germany), autofluorescence imaging, fluorescein and indocyanine green (ICG) angiography (Heidelberg Retina Angiograph 2, Heidelberg Engineering GmbH, Dossenheim, Germany), and time domain optical coherence tomography (OCT) (Carl Zeiss Meditec Model 3000 equipped with software version 4.0, Zeiss-Humphrey, Zeiss, Oberkochem, Germany) were performed in all patients at each study visit. At the last follow-up examination, spectral-domain OCT (Heidelberg Engineering GmbH, Dossenheim, Germany) imaging was performed in seven patients.
Autofluorescence measurements were performed in eight patients at month 6, 1-year and 2-year visits. The mean grey values of the transplant and the peripheral RPE were measured using ImageJ (National Institute of Health, Bethesda, Maryland). The mean of 10 measurements was calculated for each patient and each visit, and values were compared over time. Autofluorescence analysis was used using the mean grey value ratio of the graft compared with the mean grey value of the peripheral RPE. This was done to minimise the illumination effect. Statistical analysis included the paired t test, and p values <0.05 were considered statistically significant. Patients were pseudophakic at all time points.
Surgery
Patients underwent surgery between April 2004 and July 2005. The technique of autologous translocation of the choroid and RPE was previously described in detail.4 As vitreous tamponade, 20% SF6-gas was used in one patient. Eight patients received heavier-than-water silicone oil (1300 cSt., Densiron, Fluoron GmbH, Neu-Ulm, Germany), and one patient received 5000 silicone oil (Siluron 5000, Fluoron GmbH, Neu-Ulm, Germany). In patients with an excision area in the inferior quadrants, heavy silicone oil was chosen. We thereby intended to displace a potentially inflammatory aqueous vitreous environment from the wound of the lower retina to the superior circumference and intact retina.12 The silicone oil was removed after a minimum of 3 months. In all eyes, phacoemulsification was done at the time of the silicone oil removal or later. At the 2–3 years' follow-up, all eyes are pseudophakic. In five patients, the inner limiting membrane peeling was performed. All surgical procedures were performed by one surgeon (BK).
Results
Ten consecutive patients (n=10 eyes) were included in the study. Two patients were male, and eight were female. The mean age of the patients was 76.0±8.3 years. The mean follow-up time was 30±2 months (range: 25–42 months).
Functional outcome
Clinical data recorded before (baseline) and after surgery are summarised in table 1 (visual acuity, reading ability, and fixation). The mean VA decreased from 20/80 (range: 20/800–20/40) at baseline to 20/125 (range: 20/800–20/32) at 6 months and 20/200 (range: from perception of hand movements to 20/32) at 2–3 years after surgery. Between baseline and last follow-up, VA remained stable (±2 lines) in four cases and decreased (≥3 lines) in six cases. From 6 months to the last follow-up examination, VA was unchanged in six eyes (±2 lines), improved in one eye (+3 lines) and deteriorated in three eyes (≥3 lines).
Visual acuity, reading ability, fixation and complications of all patients
Prior to surgery, seven out of 10 patients were able to read with a mean reading vision of 1.09 logRAD (range: 0.5–1.14 logRAD) as compared with five patients at 2–3 years after surgery; one of these five patients had stable reading ability for up to 2 years, and one patient had even better reading ability than before surgery. Three patients lost their reading ability.
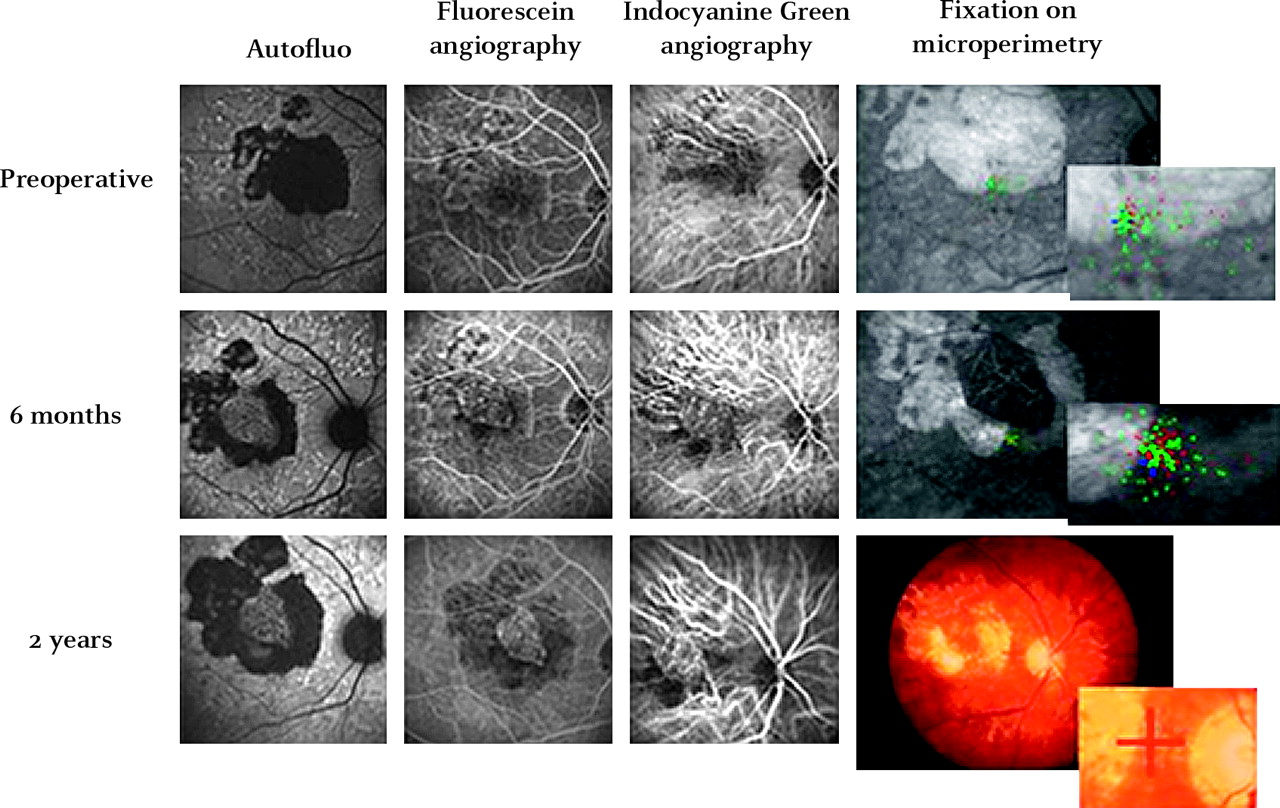
Microperimetry showed central fixation in five out of 10 eyes before surgery (table 1). Five patients used the graft for fixation at 6 months after surgery, and two eyes at 2–3 years after surgery. At last follow-up, eight patients used the area outside the graft for fixation. In one of these eight cases, the graft was not vascularised and could not be used for fixation. One case suffered a severe decrease in vision immediately after surgery, combined with postoperative complications such as branch retinal vein occlusion, recurrent iritis and PVR retinal detachment, and was not able to use the graft for fixation at any time. In three of these eight cases, the patients were able to use the patch for fixation at 6 months after surgery, but lost this ability during follow-up. In another three of these eight cases, the graft was positioned in an area with absolute scotomas and eccentric fixation prior to surgery. Retinal sensitivity in these areas could not be restored after surgery; therefore, these patients were not able to use the graft for fixation. One of these patients showed relatively stable fixation at the border of the geographic atrophy before surgery. The graft was positioned subfoveally in the area of geographic atrophy, and outside the point of fixation. At the 6 months' follow-up examination, fixation remained extrafoveal and outside the graft. At 2 years after surgery, the point of fixation had moved further away from the fovea, following the receding original RPE. The visual acuity continued to decrease from 20/50 to 20/160 (figure 1).

Patient demonstrating unfavourable positioning of the graft during surgery. In this patient (case no 7), an area underneath the geographic atrophy was used as the preferred retinal locus of fixation prior to surgery. The graft was placed within the area of the geographic atrophy. Two years after surgery, the geographic atrophy increased in size, causing the patient to change the fixation to a peripapillary area. This resulted in a decrease in visual acuity from 20/50 at baseline to 20/160 at 2 years after surgery.
Anatomical outcome
Autofluorescence of the graft was present in all eyes throughout the follow-up period. At 2–3 years' follow-up, no rapid recurrence of the geographic atrophy was seen. However, in some cases, the autofluorescence seemed to decrease slightly during follow-up. The mean grey value of the RPE of the graft was calculated and compared with the mean grey value of a presumably healthy area of RPE outside the graft. At 6 months, autofluorescence of the graft compared with healthy RPE was 71.33±12.24%; 1 year after surgery, the mean grey value remained stable with 71.49±12.35% compared with healthy RPE, but decreased at last follow-up to 65.35±16.71%. The changes in the mean grey values over time were not statistically significant (p=0.4941) (figure 2).

Mean grey value of the graft in comparison with peripheral, presumably healthy, retinal pigment epithelium. At last follow-up, the mean grey value was slightly reduced. The decrease in the overall mean grey value was not statistically significant (p=0.4941). The values are presented as mean±SD.
In nine patients, revascularisation of the graft was seen using ICG angiography as early as 3 weeks after translocation and persisted throughout the follow-up period. In one eye, the Bruch membrane was not deliberately damaged, leading to no revascularisation of the graft throughout the follow-up period. In another eye, the revascularisation was delayed and seen at 6 months after surgery.
In two patients (case nos 3 and 8), spectral-domain OCT imaging showed an intact outer nuclear layer, external limiting membrane and junction between photoreceptor inner and outer segments in the fixation area of the graft, indicating the presence of intact photoreceptors (figure 3A,B). Microperimetry showed retinal sensitivity in these areas, which could not be detected in areas in which the outer nuclear layer and the photoreceptor inner segment/outer segment junction were absent. In five of the eight cases without fixation on the graft, spectral domain OCT imaging was available at last follow-up. In those cases, areas with a preserved but thinned outer nuclear layer overlying the graft could be seen on spectral domain OCT scans, despite reduced or absent retinal sensitivity as detected on microperimetry. A photoreceptor layer could not be identified in those cases. No comparison between the preoperative and postoperative extension of areas with a preserved outer nuclear layers can be made because spectral domain OCT imaging was available only for the last follow-up.

{kind=link}
{kind=link}
{kind=link}
(A) Spectral domain optical coherence tomography showing the preferred retinal locus of fixation on the graft at 3 years after surgery. Case no 3. The red arrow points to an intact photoreceptor inner segment/outer segment (IS/OS) junction of the retina in the area of the graft, which is surrounded by an area of geographic atrophy (case no 3). The external limiting membrane can also be seen above the IS/OS junction. The microperimetry showed retinal sensitivity in this area. The visual acuity at this time point was 20/32. (B) Spectral-domain optical coherence tomography showing the preferred retinal locus of fixation on the graft at 3 years after surgery (case no 8). In this case, although the photoreceptor inner segment/outer segment (IS/OS) junction could not be identified clearly, an intact outer nuclear (yellow arrow) and outer plexiform layer (blue arrow) were visible. Microperimetry showed retinal sensitivity in this area. The visual acuity at this time point was 20/40.
As postoperative late complications, classic or occult choroidal neovascularisation (CNV) appeared in three eyes at the border of the graft. None of the CNVs affected the central area of the graft. At the last follow-up examination, the CNVs had spontaneously become scarred without any additional treatment. Epiretinal membrane formation with cystoid retinal oedema was confirmed by OCT in three eyes at the last follow-up examination; in these cases, no internal limiting membrane peeling had been performed. Other postoperative complications included retinal detachment due to proliferative vitreoretinopathy not involving the macula in three eyes, branch retinal vein occlusion and iritis in one eye, and transient ocular hypertension in two eyes (table 1).
Discussion
In this study, we examined the long-term outcome of 10 eyes with geographic atrophy following autologous translocation of RPE, Bruch membrane and choroid. With this surgical procedure, stabilisation of visual acuity and central fixation over 2–3 years could be achieved in two patients, indicating the possibility that a patch transplant can be useful in selected cases when central fixation is stable preoperatively. Using spectral domain OCT, we were able to demonstrate that an intact photoreceptor layer can be retained in the area of the graft. Microperimetry affirmed that retinal sensitivity was intact in those areas. RPE atrophy was not recorded. This is an important difference from the results of full macular translocation for geographic atrophy. Possibly the peripheral RPE—although aged like the central RPE—is more resistant to the metabolic demand of the macula than the posterior RPE adjacent to the atrophy. Still, the majority of eyes did not benefit from the RPE patch transplant. Possible explanations for their visual loss may be as follows.
Inadequate positioning of the graft
In patients with extrafoveal fixation before surgery, the graft was positioned subfoveally, aiming to regain central fixation. The graft, however, could not retrieve retinal sensitivity in areas with absolute scotoma prior to surgery, although ICG angiography showed perfusion of the graft, and the autofluorescence was intact.13 14 Therefore, even though a functioning and intact RPE cell layer was transplanted, patients with initially extrafoveal fixation have no benefit from the patch. Thus, preoperative microperimetry and spectral-domain OCT are essential to select patients with central fixation and intact photoreceptor inner segment/outer segment (IS/OS) junction.
Surgical trauma
In geographic atrophy, the macula is more adherent to the choroid compared with exudative AMD. Separating the macula intraoperatively from the choroid by means of a fluid jet or a spatula may damage the outer retina irreversibly.
Non-perfusion of the graft
The first patient in our study failed to develop reperfusion of the graft, presumably because the Bruch membrane had not been intentionally damaged. We speculate that a mechanical defect in the Bruch membrane is a precondition to allow choroidal vessels to connect to the graft. This hypothesis is based on the fact that all successful experimental models of laser-induced CNV require a rupture of the Bruch membrane (‘pop-effect’ from laser overtreatment).15 Vice versa, overexpression of VEGF in RPE cells alone is insufficient to create neovascularisation across the Bruch membrane.16 The Bruch membrane in eyes with geographic atrophy, unlike in eyes with neovascular AMD, is known to be histologically intact.17 18 Consequently, in all remaining eyes of the study, iatrogenic damage to the Bruch membrane was intentionally aimed for, and revascularisation of the graft was observed in all cases.
Retinal detachment due to proliferative vitreoretinopathy
The excision of peripheral full-thickness retina and choroid generates wound-associated inflammation, which probably stimulates proliferative vitreoretinopathy (PVR). Even though the macula was not affected by peripheral traction, retinal detachments were observed in three eyes of this study. The frequency of PVR induced by this type of surgery ranges from 8%19 to as much as 50%.4 It may be prudent to apply adjunct pharmacotherapy to suppress PVR stimuli resulting from iatrogenic trauma.20
Defects in the Bruch membrane in combination with elevated VEGF levels are thought to promote the development of neovascular AMD.21–23 Surgical trauma may induce an inflammatory response with a subsequent increase in VEGF levels. Consistent with the hypothesis of the Bruch membrane as an important barrier to neovascularisation, damaging the Bruch membrane allows not only reperfusion of the graft but also neovascularisation under and near the graft. In fact, in our study, leakage of classic or occult CNV was detected using fluorescein angiography in three of the 10 eyes during the follow-up period. The CNV was located at the borders of the graft in all cases and showed progressive scarring throughout the follow-up period. None of the eyes developed CNV originating within the central area of the graft that could impair vision and thus require treatment. This observation is in agreement with the findings of a recent study by Treumer and Roider 2007.24
In none of the patients in our study was rapid recurrence of geographic atrophy noted, in contrast to results of studies on macular translocation.9 10 A slow progressive decrease in the autofluorescence signal, possibly indicating RPE atrophy, seemed to occur in some cases. Autofluorescence may be an indicator of ongoing active RPE metabolism. A slow overall loss of autofluorescence intensity, however, seemed to be compatible with intact retinal function. On the other hand, autofluorescence was present in some of our cases over a long time period, despite absolute scotomata detected by microperimetry.
In conclusion, in selected patients with stable central fixation, translocation of autologous full-thickness grafts of the RPE, Bruch membrane and choroid may result in stabilisation of visual acuity and central fixation over a 2–3-year period. The functional outcome in this series, however, is limited due to unfavourable patient selection and postoperative complications, such as PVR.
References
Footnotes
Funding Supported in part by the RetinoVit Foundation Cologne.
Competing interests None.
Patient constent Obtained.
Ethics approval Ethics approval was provided by the Ethics Committee, University of Cologne, 50924 Cologne, Germany.
Provenance and peer review Not commissioned; externally peer reviewed.