Article Text

Abstract
Background/aims To investigate the clinical features of Chinese patients with seropositive myelin oligodendrocyte glycoprotein antibody (MOG-Ab) optic neuritis (ON) and patients with seropositive aquaporin-4 antibody (AQP4-Ab) ON.
Methods In this retrospective observational study, sera from patients with demyelinating ON were tested for MOG-Ab and AQP4-Ab with a cell-based assay. Clinical characteristics were compared between MOG-Ab-related ON (MOG-ON) and AQP4-Ab-related ON (AQP4-ON), including visual performances, serum autoantibodies and features on MRI.
Results A total of 109 affected eyes from 65 patients with demyelinating ON (20 MOG-ON and 45 AQP4-ON) were included. The onset age of MOG-ON was younger than AQP4-ON (MOG-ON: 20.2±17.4 years old, AQP4-ON: 35.6±15.7 years old, P=0.001). Onset severity was not different between these two groups (P=0.112), but patients with MOG-ON showed better visual outcomes (P=0.004). Half of the MOG-ON had a relapsing disease course. Nineteen per cent of patients with AQP4-ON presented coexisting autoimmune disorders, but there were no coexisting autoimmune disorders among patients with MOG-ON. Optic nerve head swelling was more prevalent in patients with MOG-ON (P<0.01). Retrobulbar segment involvement of the optic nerve were more common in patients with MOG-ON according to our MRI findings (P<0.01). Patients with MOG-ON showed longitudinally extensive lesion in 30% and chiasm and optic tract involvement in 5%.
Conclusions MOG-ON is not rare in Chinese demyelinating patients. It underwent a severe vision loss at onset but had relatively better visual recovery than patients with AQP4-ON. MOG-ON might have an unique pathogenesis different from AQP4-ON.
- optic neuritis
- myelin oligodendrocyte glycoprotein antibody
- aquaporin-4 antibody
- clinical features
- visual performances
- magnetic resonance imaging
Statistics from Altmetric.com
- optic neuritis
- myelin oligodendrocyte glycoprotein antibody
- aquaporin-4 antibody
- clinical features
- visual performances
- magnetic resonance imaging
Introduction
Optic neuritis (ON) is one of the most common types of acute optic neuropathy in young individuals, especially under age of 45 years old. It has been associated with demyelinating diseases.1 Many studies have demonstrated that the pathogenesis of ON could be related to specific autoantibodies that damage the integrity of myelin surrounding the optic nerves, resulting in severe visual impairment.2
Demyelinating ON is the main manifestation of central nervous system (CNS) inflammatory demyelinating diseases (IDDs) in ophthalmology. Neuromyelitis optica (NMO) is the more common CNS IDD in Chinese population.3 ON was the initial feature in approximately 50% of patients with NMO.4
Aquaporin-4 antibody (AQP4-Ab) has been known as the most important biomarker for NMO.5 However, about 10%–20% of patients with NMO were serological AQP4-Ab negative.6 Recently, myelin-oligodendrocyte glycoprotein antibody (MOG-Ab) was discovered in some AQP4-Ab-negative NMO patients, and a better prognosis was reported in this subset of patients.7–10 In contrast, a multicentre study conducted by the Neuromyelitis Optica Study Group (NEMOS) reported that 64% MOG-IgG-positive patients initially presented with isolated ON and showed predominantly a relapsing and frequently aggravated disease course.11 The study of Hacohen et al 12 found that 35% of patients with childhood acquired demyelinating syndrome (ADS) were MOG-Abs-positive and 52% of MOG-Abs-positive patients were ON. One study of Chinese patients with CNS IDD found that ON was the most frequent clinical presentation at onset (75.0%) or during the whole disease course (83.3%) in MOG-Ab-associated IDDs.13 Some previous studies involving patients with NMO spectrum disorders (NMOSD)14 observed retinal neuroaxonal damage in MOG-Ab-positive patients, with or without ON.
As a different biomarker, MOG-Ab might predict a diseases course different from AQP4-Ab. It might play an essential role in the diagnosis and management of patients with ON. Few previous studies15 16 have focused on the MOG-Ab serostatus in patients with ON, and those were limited by a relatively small MOG-ON sample size.
The current study aimed to present the clinical characteristics of MOG-ON and compared with the features of AQP4-ON in Chinese patients.
Materials and methods
This was a retrospective observational study on patients diagnosed with ON in the Neuro-ophthalmology Department of the Chinese People’s Liberation Army General Hospital (PLAGH), between 1 May 2016 and 1 October 2016. The study protocol was approved by the institutional review board at the Chinese PLAGH and adhered to the tenets of the Declaration of Helsinki.
Diagnostic criteria
The diagnosis of demyelinating ON was based on the criteria established by the Optic Neuritis Treatment Trial (ONTT) Group: (1) acute vision loss involving one or both eyes with or without eye pain; (2) presence of a relative afferent pupillary defect or presence of visual evoked potential abnormalities; and (3) abnormal visual field consistent with optic neuropathy.17
Subjects who fulfilled any of the following criteria were excluded: (1) any secondary or other types of optic neuropathy, for example, compressive, vascular, toxic, metabolic, infiltrative or hereditary optic neuropathy; (2) corneal opacity, dense cataract and glaucoma, vitreous or retinal diseases; or (3) no positive response to serological tests of AQP4-Ab or MOG-Ab with cell-based assay.
Laboratory examinations
Results of blood tests on all study subjects were collected, including erythrocyte sedimentation rate and C reaction protein analyses, total antinuclear antibodies (ANAs) titre, Sjögren’s syndrome A (SSA)/B (SSB), proliferating-cell nuclear antigen, antineutrophil cytoplasmic antibodies, rheumatoid factor and major histocompatibility complex-B27 (HLA-B27). The thyroperoxidase antibody and thyroglobulin antibody was tested by chemiluminescence immunoassay. Additionally, results of cerebrospinal fluid (CSF) tests were also collected, including cell counts, levels of total protein, glucose and chloride, as well as oligoclonal band (OCB) examination. The criteria of elevation in CSF tests were defined as: white cell count elevated: white cell count >10/μL; protein elevated: protein >400 mg/L; IgG level elevated: IgG level >3.4 mg/dL.
AQP4-Ab and MOG-Ab assays
Patients with demyelinating ON underwent serum tests for anti-AQP4-IgG and anti-MOG-IgG with cell-based assay (CBA). The procedure of AQP4 antibody detection in living cells was described previously.18 In terms of MOG antibodies testing, live HEK-293 cells were transiently transfected with a plasmid containing full-length human MOG cDNA before it exposed to the patients’ diluted serum. Goat antihuman IgG labelled with Alexa488 was used as a secondary antibody. Two independent and masked evaluators identified the scores as positive or negative. The serums were titrated in 1:10 dilutions afterwards to determine the highest dilution level where scores remain positive.
Ophthalmic examinations and therapy
All subjects received a series of ophthalmic examinations, including the relative afferent papillary defect test, the slit-lamp biomicroscopy examination, intraocular pressure document and the fundus evaluation. Best-corrected logarithm of the minimum angle of resolution (LogMAR) visual acuity (VA) was performed on the standard table at 5 m distance. For those subjects who were unable to read letters at 1 m distance, they would be further examined by finger counts, hand movements or perceiving light. The retinal thickness was assessed by the high-definition spectral-domain optical coherence tomography (Carl Zeiss Meditec, Dublin, Ohio, USA). The orbit, brain and spinal MRI were also preformed and evaluated according to Paty criteria19 using MRI-3.0T (TW1WSPEED HDXT, Georgia, USA) with postcontrast T1-weighted conventional spin-echo (repetition time (TR)=680 ms; echo time (TE)=14 ms, field of view (FOV)=24, slice thickness=3.0, interleaved) at 5 min after the intravenous administration of 0.1 mmoL/kg gadopentetate dimeglumine. All patients were treated with intravenous methylprednisolone and oral steroids therapy in acute phase.
Statistical analysis
Differences of continuous data were compared by independent t-test (normal distribution) or Mann-Whitney U test (non-normal distribution). Normality of the data was tested using Shapiro-Wilk test. Categorical data were compared using Pearson χ2 test or Fisher’s test. A two-tailed P value <0.05 was considered statistically significant. All statistical analyses were performed using SPSS software (V.17.0).
Results
Demographic manifestations
A total of 65 patients (109 affected eyes) were recruited in this study, consisting of 20 patients (30.8%) with serological positive MOG antibodies (MOG-ON) and 45 patients (69.2%) with serological positive AQP4 antibodies (AQP4-ON). The patients with MOG-ON had a younger age of disease onset at 20.2±17.4 years old (range: 5–63 years old) compared with the AQP4-ON group with a mean age of onset at 35.6±15.7 years old (range: 8–72 years old) (P=0.001). In addition, MOG-ON group presented a higher percentage of juvenile patients (<18 years) (MOG-ON: 65%, AQP4-ON: 11% p<0.001). There were 70% (14/20) female patients in the MOG-ON group, whereas 90% (42/45) were female in the AQP4-ON group (P=0.034). Shorter observation time was noticed in MOG-ON group with 29.0±32.5 months (range: 5.0 months to 137.0 months), comparing with the AQP4-ON group with 51.0±65.9 months (range: 5.0 months to 220.0 months), but this difference was not statistically significant (P=0.076) (table 1).
Comparison of demographic characters between the patients with MOG-ON and AQP4-ON
Comparison of clinical features according to antibody status
Table 2 summarised the clinical features of the MOG-ON and AQP4-ON groups. Forty-five per cent patients presented bilateral involvement at initial onset of ON in the MOG-ON group, while 37.8% in the AQP4-ON groups (P=0.583). A slightly higher proportion of patients with MOG-ON (80%) presented optic disc swelling compared with the AQP4-ON group (20%) (P<0.001). Recurrent episodes occurred in half of the cases in the MOG-ON group and 71.7% of patients in the AQP4-ON group (P=0.100). The interval time from the first to the second attack was 28.6±30.1 months (range: 5–96 months) in the MOG-ON group, whereas 31.1±35.3 months (range: 3–132 months) in the AQP4-ON group (P=0.842). There was no significant difference in the number of eyes with severe visual loss (defined as best-corrected VA (BCVA) <0.1) at Nadir between the two groups. Interestingly, the visual acuity outcomes of patients with MOG-ON were significantly better than patients with AQP4-ON from the Nadir episode, representing fewer cases suffered from severe visual loss (BCVA <0.1) at the latest follow-up in the MOG-ON group (MOG-ON: 20%, AQP4-ON: 46.7%, P=0.004).
Comparison of clinical features between the patients with MOG-ON and AQP4-ON
Comparison of laboratory findings, according to antibody status
Comparison of laboratory findings between the patients with MOG-ON and patients with AQP4-ON was summarised in table 3. There were 42.2% of patients with AQP4-ON presented coexisting autoimmune disorders, including seropositivity of anti-SSA/SSB antibody, anti-ANA, HLA-B27 antibodies and thyroid-related autoantibodies, but no coexisting autoimmune disorders in patients with MOG-ON (P=0.001). In terms of the CSF tests, elevated protein levels occurred in 6.7% of patients with AQP4-ON, but not in patients with MOG-ON (P=0.547). White cell counts were raised in 11.1% of patients with AQP4-ON, and in 5% of patients with MOG-ON (P=0.748). There was one patient with MOG-ON responded positive for OCBs, whereas none in AQP4-ON samples (P=0.308).
Comparison of laboratory findings in the patients with MOG-ON and AQP4-ON
Comparison of MRI manifestation according to antibody status
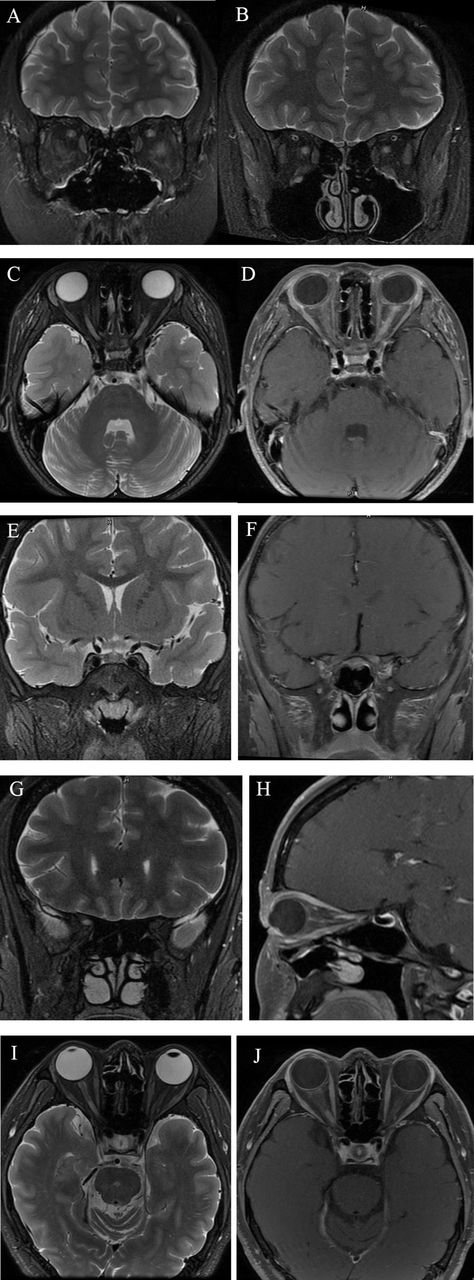
All of the involved optic nerves were revealed for T2 hyperintensity (with or without enhancement) through MRI. An example of abnormal findings on the MRI of optic nerve in a MOG-ON and a AQP4-ON patients were shown in figure 1. Table 4 summarised the comparison of MRI manifestations between the MOG-ON and AQP4-ON groups. Retrobulbar segment involvement on the optic nerve was found in majority of patients with MOG-ON (MOG-ON: 80%, AQP4-ON: 20%, P<0.001), whereas canalicular portion of optic nerve was involved more in patients with AQP4-ON (MOG-ON: 30%, AQP4-ON: 57.8%, P=0.039). In addition, the lesions on patients with AQP4-ON showed a higher portion of longitudinally extensive optic nerve lesion (57.8%) than MOG-ON (30%) (P=0.039). Besides, 15% of patients with AQP4-ON had optic chiasma and 5% had optic tract involvement.
Comparison of orbital MRI findings in the patients with MOG-ON and AQP4-ON
{kind=link}
Optic nerve abnormalities detected by MRI in patients with MOG-ON and AQP4-ON (A and B) coronal T2-weighted images from a 10-year-old girl with seropositive MOG-Ab relapsing ON. (A) Lesions in bilateral retrobulbar segment of the optic nerve on the first attack. (B) Lesions in bilateral retrobulbar segment of the optic nerve on the second attack, 1 year after the first attack. (C–F) Images from a 5-year-old girl with seropositive MOG-Ab bilateral ON showing longitudinally extensive bilateral optic nerve lesion extending from the chiasm. (C) Axial T2-weighted Image. (D) T1 postcontrast images. (E) Coronal T2-weighted Image. (F) T1 postcontrast image. (G and H) Images from a 41-year-old woman with seropositive AQP4-Ab ON. (G) Coronal T2-weighted image showing extensive T2 high signal in the right posterior portion of the optic nerve. (H) Sagittal Gd enhancement T1-weighted image, showing lesion in the right posterior portion of the optic nerve with marked postcontrast enhancement. (I and J) Images from a 51-year-old man with seropositive AQP4-Ab ON. (I) Axial T2-weighted image, showing extensive T2 high signal in the right posterior portion of the optic nerve. (J) Axial Gd enhancement T1-weighted image showing lesion in the right posterior portion of the optic nerve with marked postcontrast enhancement. AQP4-ON, aquaporin-4 antibody-associated ON; MOG-ON, myelin oligodendrocyte glycoprotein antibody-associated ON; ON, optic neuritis
Discussion
MOG antibodies have been reported to be associated with a variety of demyelinating diseases, such as NMOSD,7 ON and acute disseminated encephalomyelitis (ADEM).20 MOG has been considered as a conformational dependent antibodies for ADEM.21 About one-third of patients with childhood ADS were reported with serological-positive MOG antibodies, such as clinically isolated syndrome, multiple sclerosis and ADEM.22 In addition, about 17.8% of MOG-IgG-positive patients were reported as ADEM with ON or long extensive transverse myelitis, while 12.7% of them presented as NMO, 49.2% presented as ON. By contrast, among AQP4-IgG-positive patients, there were 47.1% presented as NMO, 9.5% presented as ON, but none presented as ADEM.23 Furthermore, evidence showed that the severity of disease in ADEM was associated with the titre of MOG-IgG.24 MOG antibodies could play an important role in ADEM clinically. Nevertheless, the patients recruited in the study were not having enough evidence to diagnosed as ADEM or NMO, conversion of the clinical subtypes should be confirmed in the further longitudinal study.
The differences in antibody assays often lead to non-specific results or false positives. Western blot and ELISA are traditionally used to detect MOG antibodies, but these assays may lead to conflicting results. The CBA is a universal method for MOG-Ab and AQP4-Ab detection and recommended by the International Panel for NMO Diagnosis.25 Twenty MOG-Ab-positive patients and 45 AQP4-Ab-positive patients were screened out by the cell-based assay in this study.
The patients with MOG-ON had younger disease onset with an average of 20.2±17.4 years old than patients with AQP4-ON with 35.6±15.7 years old in this cohort (P=0.001). This finding was consistent with previous reports that compared between MOG-ON (32.29±17.1 years old) and AQP4-ON (44.86±14.8 years old),8 MOG-ON (31 years old) and AQP4-ON (38 years old),10 MOG-ON (20±14 years old) and AQP4-ON (23±14 years old).26 More than half (65%) of our patients with MOG-ON had a juvenile (<18 years) disease onset, which was more than those reported by previous study showing about 12.5%,9 50%10 or 16.7%13 of MOG-Ab-positive patients with demyelinating diseases began during juvenile period. The age at MOG-ON onset ranged from 5 years to 63 years, and the age at AQP4-ON onset ranged from 8 years to 72 years. Both of MOG-ON and AQP4-ON could occur in children or in the elderly. This result was similar to previous reports.9 13
More than 90% of patients with AQP4-ON were female indicating a strong female predominance in patients with AQP4-ON. Similar female/male ratio was also observed in AQP4-Abs-positive demyelinating disease in the other studies.8 9 In contrast, patients with MOG-ON had a less female preponderance, 70% of MOG-ON patients were female; nevertheless, females still accounted for the majority among patients with MOG-ON in this study. However, the sex ratios were variable in the previous reports, female patients accounted for between 37.5% and 75%.8–10 26
Bilateral ON and optic disc swelling were commonly observed in our Chinese MOG-ON cohort, which was corresponding with those patients with MOG-ON in various ethnic groups.26 However, previous reports indicated that most of the MOG-Ab-positive patients presented as monophasic disease or had less relapsing rate,8 9 which was different from the current study demonstrating both patients with MOG-ON and AQP4-ON had high recurrent episodes. However, in some other studies, patients with MOG-ON were frequently associated with a recurrent disease course.14 This study indicated that Chinese patients with MOG-ON might also have a high tendency to relapse, so that long-term immunotherapy should be considered in relapsing patients with MOG-ON.
Most of the patients with MOG-ON in this study were suffered from severe vision loss at the first attack but had relatively good visual recovery by comparing with patients with AQP4-ON. The ONTT studies reported 50% of patients with idiopathic demyelinating ON could have visual recovery of 20/20 and 68% had 20/40 or better vision after 1 year.27 In our previous study, the BCVA in AQP4-Ab-negative ON eyes was better than AQP4-Ab-positive ON eyes.28 In NEMOS of Caucasian descent,14 the patients’ VA was less impaired in the MOG-ON subgroup than in the AQP4-ON subgroup after more than 3 months follow-up, but the difference was not significant. The results from our Chinese cohort showed that the onset episode severity of patients with MOG-ON was similar to AQP4-ON ones but had a better visual recovery for the former group of patients.
Coexisting autoimmune disorders were presenting in more than one-fourth (19/73) of our patients with AQP4-ON. This phenomenon was also observed in AQP4-Ab-positive NMOSD.29 By contrast, coexisting autoimmune disorders were absent in all of the MOG-ON patients in our Chinese cohort. It was in line with other studies that reported a lower frequency of concomitant autoimmune disorders in ‘AQP4-IgG-seronegative’ patients with NMOSD.30 The results indicated that MOG-ON might have less overlapping pathogenesis with autoimmune disorders than AQP4-ON.
Consistent with the study of Ramanathan et al 26 the MRI lesions showing on the patients with MOG-ON tended to involve the anterior optic nerve segment, whereas patients with AQP4-ON were involved the posterior optic nerve segment. Nevertheless, there were 3/20 (15%) of lesion on patients with MOG-ON involved optic chiasm, and 1/20 (5%) of the encountered lesions involved optic tract in the current study, which indicated that MRI manifestation of MOG-ON can be longitudinally extensive and affect the entire visual pathway.
Some limitations still exist in the current study. First, all of the recruited subjects were collected from the single neuro-ophthalmology centre in the northern China instead of a multicentre study. Second, because the patients presented ocular symptoms and visited ophthalmology clinic first, some MOG-Ab-positive patients with non-ocular demyelinating disorders could not be investigated. Larger investigations cooperation with neurology department and other institutes should be conducted in the further study. Third, longitudinal study should also be necessary in Chinese patients with MOG-ON to investigate the conversion rate of NMOSD or ADEM.
In summary, the clinical features of MOG-ON in Chinese demyelinating ON were not mild like most previous reports. Most of patients with MOG-ON underwent a severe vision loss at onset and had a high relapsing tendency. MOG-ON had some distinct clinical features with AQP4-ON, such as a high rate of optic disc involvement, less overlapping pathogenesis with autoimmune disorders and also a better visual recovery. We believed that MOG-ON might have its unique pathogenesis, which was different from AQP4-ON. MOG-Ab should be tested in patients with demyelinating ON as a serological clinical biomarker in clinical management.
Acknowledgments
We would like to thank all the participants in this study and Dr Mo Yang, Dr Shuo Zhao, Dr Hao Kang, Dr Dahe Lin, Dr Huanfen Zhou, Dr Chunxia Peng, Miss Mengying Lai and all participating optometrists and nurses at Department of Ophthalmology in Chinese PLA General Hospital, for their assistance.
References
Footnotes
YZ and ST contributed equally.
Contributors YZ and ST: study design, manuscript draft and revision, data collection and statistical analysis. TCYC: study design and manuscript revision. QX: study design and manuscript revision. JZ, DT and HF: study design and data collection. SW: study design, correspondence and manuscript revision.
Funding National High TechnologyResearch and Development Program of China (863 Program) 2015AA020511 and 59th China Postdoctoral Science Foundation 2016M592983.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The institutional review board at the Chinese PLAGH.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance