Article Text

Abstract
Herpes zoster ophthalmicus (HZO) is a common, vision and potentially life-threatening disease caused by the reactivation of the varicella-zoster virus (VZV) in the distribution of the first division of cranial nerve V. Although the rate of herpes zoster increases with age, over half of the people with zoster in general, including HZO, are under age 60. In addition, over 90% of people with zoster are immunocompetent, even though the disease is more common and severe in immunocompromised patients. The incidence of zoster is increasing worldwide for unknown reasons. The epidemiology has not yet been impacted by the zoster vaccine (ZV). The lack of a strong recommendation by physicians for this vaccine is a major barrier to its use. An unresolved dilemma regards the optimum timing for this vaccine. In the USA, the current recommendation by the Centers for Disease Control and Prevention (CDC) is for eligible people age 60 and older, despite its greater efficacy in reducing the incidence of disease and Food and Drug Administration (FDA) approval for age 50–59. Although there is a consensus regarding use of acute high-dose oral antiviral treatment to reduce ocular complications, there is limited evidence for prolonged treatment. The rationale for a proposed randomised controlled trial (RCT) of suppressive antiviral treatment to reduce chronic eye disease and postherpetic neuralgia (PHN) includes evidence that zoster is followed by chronic active VZV infection and similarities between HZO and herpes simplex virus (HSV) eye infection, where this treatment is effective and is the standard of care.
- Treatment other
Statistics from Altmetric.com
Introduction
Herpes zoster (HZ), also referred to as shingles, is caused by reactivation of the varicella-zoster virus (VZV) in people who have had chickenpox (varicella), the primary infection caused by VZV, typically resulting in a painful, unilateral, dermatomal, vesicular rash (figure 1). There are about one million new cases of HZ in the USA annually, of which up to 20% involve the first division of cranial nerve V (trigeminal) resulting in herpes zoster ophthalmicus (HZO). HZ affects approximately 30% of the population, increasing to 50% of people who live beyond age 85 years.1

View of the face of a 70-year-old man during an attack of shingles, also known as herpes zoster. A red rash with blisters has appeared on his forehead, and his eye is swollen. This rash is extremely painful and is due to herpes infecting the sensory nerves, in this case the ophthalmic branch of the trigeminal nerve. Shingles is caused by the chickenpox virus (varicella-zoster). Dormant viruses survive for years in humans until the immune system is weakened by illness or age. Credit: Dr P. Marazzi, Science Photo Library.
It is a common misconception that HZ is a disease of the elderly. Although the rate of HZ increases with age, the number of cases in general, including HZO, peaks in individuals age 50–79.2–4 The mean age of onset in the USA is approximately 52 years.5 That more than half of all cases of HZ occur in people under age 60 is not a new phenomenon, as 58% of patients were less than 60 in a paper published in 1971.6 Although postherpetic neuralgia (PHN), defined as chronic, often incapacitating, dermatomal pain persisting more than 90 days, affects primarily people with HZ onset age 60 years and older, younger-onset patients suffer from acute pain with a mean duration of approximately 1 month, and are at risk for other complications, including, but not limited to, vision-threatening chronic eye disease.7
The incidence of HZ has been steadily increasing in the USA since the year 2000 among people age 40 and older for unknown reasons.8 The incidence of HZ in North America, Europe and the Asia Pacific is comparable and increasing, and this trend started in the absence of varicella vaccination programmes against chickenpox.9 In developed countries, the age-adjusted rates of HZ are similar, and even higher in regions of the world with widespread HIV infection.9 ,10
Another common misconception is that healthy people are not at risk for HZ. Although HZ is more common and severe in immunocompromised people, 92% of people with HZ are not immunocompromised.4 Relatively young and healthy patients with zoster can develop serious sequelae, including neurological complications and probably coronary artery disease in addition to eye disease.11–13
A retrospective population-based cohort study in Hawaii found the incidence of HZO was 30.9 per 100 000 patient years.14 The incidence was highest in people age 65 and older (104.6 per 100 000 patients, compared with 42.2 in ages 45–64, 15.4 in ages 25–44 and 7.2 in ages 15–24), but similar numbers of cases occurred in people ages 45–64 (54 cases) and ages 65 and older (56 cases). Ocular involvement occurred in 35.1% of patients with HZO, with keratitis being the most common manifestation. Overall, PHN developed in 20.9% of patients, but occurred in 30% of patients with ocular involvement in comparison to 16% with only skin involvement (p=0.08). Patients age 65 and older were significantly more likely to have PHN than younger patients (p=0.009).
HZ can result in chronic pain, diminished quality of life, chronic eye disease, reduced vision and even death.15 ,16 Most studies find that women are affected significantly more frequently than men with regard to HZ incidence, hospitalisations and mortality.14 ,17 ,18 PHN persists for longer than 1 year in nearly half of the patients older than age 70.19–21 The direct medical cost burden of HZ may exceed US$1 billion annually in the USA.20 In patients with HZ who develop PHN, 1-year costs are more than five times greater than costs in patients with HZ without PHN.19 The negative impact of HZ and PHN on health-related quality of life is closely correlated with the severity of pain and persists as long as clinically significant pain.7 ,22 A population-based study shows that HZ is a risk factor for developing major depression.23 Notably, PHN has been reported to be the most common cause of suicide in chronic pain patients who are over age 70.24
Publications that compare HZO with HZ occurring in other locations point to the risk of PHN and stroke being greater after HZO than HZ elsewhere.22 ,25 PHN after HZO lasts longer and is more frequent than PHN after HZ in general, despite recommended acute antiviral treatment.21 ,22 ,25 Although potentially fatal strokes are an uncommon complication of HZ, patients with HZO have 4.5 times higher risk of stroke within a year after diagnosis compared with controls, and the adjusted HR of stroke after HZO is 4.3 compared with 1.3 after HZ in general.26 ,27 In a self-controlled, case-series, population-based study, the risk of stroke for 6 months more than doubled after HZO compared with HZ in general.28 Although the risk of stroke after HZ is greatest in the short term, increased risk continues beyond the first year, and is greatest in patients under age 40.29
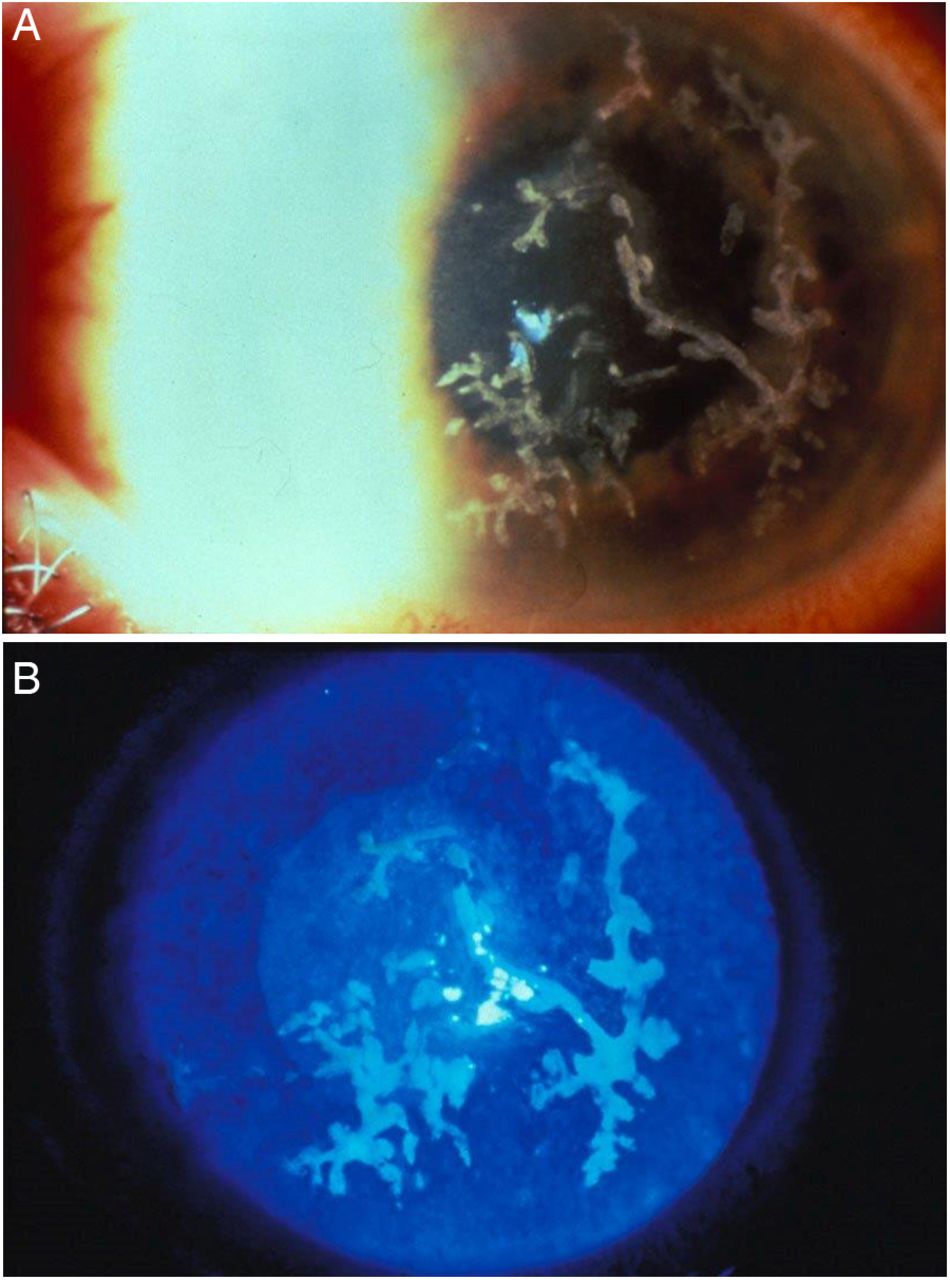
Disease manifestations of HZO vary with the age at onset of disease. In a retrospective study of over 100 patients with HZO, in which half of the cases had an onset under age 60 years, late dendriform keratitis occurred more often in patients who were under age 60 compared with those age 60 or older (36% vs 17%, p=0.03)3 (figures 2A, B). Younger patients averaged 3.2 episodes of recurrent inflammation, compared with older patients with 1.5 episodes (p=0.01). Complications, including PHN, neurotrophic keratitis and secondary infected corneal ulcers, were all significantly more common in older-onset patients (38% for those age 60 or older at onset vs 8% for those under age 60 at onset, p=0.001; 31% vs 9%, p=0.005 and 17% vs 3%, p=0.04; respectively).3

(A) Typical late dendriform keratitis due to varicella-zoster virus (VZV). These branching elevated lesions without terminal bulbs are often PCR-positive for VZV and respond to topical gangciclovir, evidence that they are signs of chronic and/or recurrent VZV infection. (B) The dendriform lesions stain with fluorescein.
The zoster vaccine
The zoster vaccine (ZV) (Zostavax (Zoster Vaccine Live), Merck & Co., Whitehorse Station, New Jersey, USA) is recommended by Centers for Disease Control and Prevention (CDC) for immunocompetent patients age 60 and older since 2006 in the USA, and was approved by the Food and Drug Administration (FDA) for immunocompetent patients age 50 and older in 2011.30 ,31 This vaccine is a live vaccine using the attenuated Oka strain of VZV at 14× the concentration used in the varicella vaccine. In the USA, it costs between US$185 and US$230. This vaccine decreases the incidence of HZ by approximately 50%,30 but it has failed yet to affect the epidemiology of zoster.10 As of 2013, according to CDC, it had been received by only approximately 24% of eligible individuals in the USA age 60 and older. Given that the mean age of onset in the USA is approximately 50, and the vaccine reduces the incidence by only 50%, over 95% of all people in the USA are at continued risk for HZ.5 ,32
Vaccine efficacy and safety
In a randomised controlled trial (RCT) of over 38 000 people age 60 years and above, the ZV reduced the burden of disease (a combination of incidence, severity and duration) by 61.1%, PHN by 66.5% and the incidence of HZ by 53.1%.30 The incidence of HZ was reduced by 63.9% in people age 60–69 and only 37.6% in people age 70 years and older. Because the effect on severity of disease was greater among older patients, the reduction in burden of disease was similar in both age groups.30 After a subsequent study reported a 68% reduction in incidence of HZ following the ZV in people age 50–59, the FDA approved the vaccine for this age group.33 Immunocompromise, due to diseases or treatment, reducing T-cell-mediated immunity, is the main contraindication for this live vaccine (http://www.cdc.gov/vaccines).
The vaccine is safe, with only local injection site reactions and headaches (6%) occurring more often in vaccine recipients than in controls.31 Local reactions are significantly more common in younger than in older people.30 ,34 ,35 These reactions may reflect the greater immune response of younger vaccine recipients.
There are case reports of two patients with HZO who developed recurrences 3 and 5 weeks after ZV, respectively, likely due to an immune response.36 ,37 Patients with HZO should be informed of this, and monitored 3–6 weeks after ZV.
Two cases of acute retinal necrosis 6 days and 2 months after the ZV, respectively, raise safety issues.38 The ZV was contraindicated in one renal transplant patient. The other patient had end-stage renal disease, which was associated with lymphoid immune dysfunction, but not a current CDC contraindication.39 The contraindication for ZV in people with impaired cellular immunity should be strictly followed.
Overcoming barriers to vaccination
Barriers to use of the ZV in the USA include high cost, complex and partial reimbursement, frozen storage requirement and lack of a strong recommendation by primary-care doctors.40 ,41 Despite interventions to overcome these barriers, including education, availability at pharmacies and electronic medical record reminders, primary-care doctors do not consider this vaccine as important as influenza and pneumonia vaccines.42 ,43 Ophthalmologists can also recommend this vaccine to their patients.41 Implementation of evidence-based medical practices requires changes first in knowledge, then attitudes and finally practice.44 According to the bioethicist, Arthur Caplan, changes in behaviour also involve a sense of moral obligation to do the right thing (personal communication).
Timing of vaccination
Despite 68% efficacy in preventing HZ in people vaccinated age 50–59, FDA approval of ZV for this age group in 2011 and an absence of supply issues since 2012, as of 2014, the CDC continues to recommend this vaccine only for people age 60 years and older.45 They base this decision in part on the analysis of a recent decision (cost-effectiveness) model that demonstrates lesser health impacts and a higher incremental cost-effectiveness ratio (ie, dollars per unit of health gained) of vaccination at age 50 as compared with vaccination at older ages.46 In contrast, a previous modelling study based on UK data estimated that vaccination for HZ for those between 50 and 59 would be cost-effective.47 The results of the CDC analysis were likely strongly influenced by uncertainty of data regarding vaccine durability, complication rates and impact of HZ and PHN and costs.48 New insights into these uncertainties may alter the attractiveness of ZV among younger cohorts.
Data on people vaccinated age 60 years and older in the short-term persistence study and the long-term persistence study indicate that efficacy of the vaccine wanes after 8 years for incidence of disease and 10 years for burden of illness and PHN.49 ,50 No long-term efficacy studies have been done on people vaccinated at age 50–59, who may have a differential durability of response (ie, a patient vaccinated at younger age may maintain a greater degree of protection over a given time period than the same patient vaccinated at an older age).51 Furthermore, recent evidence supports that there are similar immunological responses in those undergoing revaccination as compared with first-time vaccinees, suggesting that revaccination after initial vaccine efficacy wanes is scientifically plausible.52
The incidence of complications in the CDC study is based on a single publication regarding one county in Minnesota,4 which may not be representative of the US population, and non-PHN complications of HZ may have been underestimated.46 Recent epidemiological and biological evidence links incident HZ (and especially HZO) with ischaemic stroke,26–29 a highly morbid disease with large healthcare costs. There is evidence to suggest that the risk of stroke following HZ (or HZO) is greatest among younger people (<60 years),29 potentially increasing the value of prevention among this population. Furthermore, recurrence of HZ may be more prevalent than initially suspected,53 which was not accounted for in the CDC analysis. Substantial recurrence rates among patients under 60 years of age could further increase the indirect and productivity costs incurred by this population, which is not accounted for in the CDC cost-effectiveness calculations.
Methods of accounting for both direct (eg, vaccine-related costs, healthcare usage) and indirect costs (eg, lost time at work) may have increased the inefficiency of earlier vaccination strategies. Inclusion of costs related to minor local reactions (greater incidence in 50–59 vaccine recipients) and non-inclusion of productivity losses (also greater in patients with HZ age 50–59)20 could act in concert to make earlier vaccination appear less valuable in this analysis.
Clearly, more research is needed to address key questions related to the durability of response to ZV, and the potential for revaccination, in order to clarify the most optimal prevention strategies, since ZV is more effective in preventing HZ in younger recipients.
Rationale for investigation of suppressive antiviral treatment in HZO
Although there is considerable consensus on oral antiviral treatment of acute HZO, there is no standard approach to treatment of HZO sequelae, including ocular disease and PHN. Standard recommended care, consisting of acute oral antiviral treatment beginning within 72 h of rash onset with valacyclovir 1000 mg three times daily, famciclovir 500 mg three times daily or acyclovir 800 mg five times daily for 1 week reduces chronic ocular complications from 50% to 30%, but does not prevent them54 ,55 or reduce PHN.56 ,57 Long-term topical corticosteroids are needed to control stromal keratitis, endothelialitis and/or uveitis in most patients with chronic HZO disease (figures 2, 3A, B, 4 and 5). Effective treatment for dendriform keratitis is topical gangciclovir five times a day for 2 weeks and then twice daily for 2–4 weeks.58 Use of long-term suppressive oral antivirals is highly variable.59

Stromal keratitis without ulceration. (A). Broad slit-lamp image with corneal neovascularisation and stromal opacity with lipid deposition. (B). Narrow slit image showing stromal keratitis.

Endothelial keratitis with localised full-thickness corneal oedema.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Case of zoster sine herpete (radicular pain without rash) associated with neurotrophic keratitis, uveitis with hypopyon and necrotising scleritis. After epithelial defect heals, uveitis is treated with topical steroids. Scleritis requires systemic treatment.
Several factors call for evaluating long-term suppressive antivirals to prevent HZO complications in an RCT: recent discoveries about the infectious pathogenesis of complications of HZ and HZO, the significant benefit of suppressive antivirals in reducing recurrent herpes simplex virus (HSV) stromal keratitis and evidence of comparable benefit of suppressive antiviral treatment of chronic HZO and HSV in a retrospective study.60–63 A 2012 editorial in Archives of Ophthalmology suggested that ‘… although stromal keratitis or uveitis may not represent active viral infection, clinicians may question whether subclinical or intermittent viral shedding may help to perpetuate destructive, inflammatory, anterior segment disease in HZO’.64 In one survey, over 85% of specialists reported treating cases of chronic or recurrent HZO in the preceding year. They reported prescribing oral antivirals most often for 7–14 days (37%), while some used them for a year or longer (15%) and others as long as patients were on topical corticosteroids (15%).59 Confirming that long-term antiviral treatment reduces morbidity associated with chronic HZO could significantly reduce the disease burden for patients and costs to society.
Evidence of chronic active VZV infection after HZ and HZO
The rationale for a randomised placebo-controlled trial of prolonged suppressive valacyclovir treatment of HZO includes the increasing body of evidence that chronic active VZV infection occurs after HZ and contributes to complications, including dendriform keratitis, uveitis, PHN and strokes.61 ,62 ,65–69 In 1995, a study showed that late epithelial dendriform keratitis lesions were often PCR-positive for VZV, and this was confirmed in 2010 by a larger series.61 ,62 Dendriform keratitis’ response to antiviral treatment is further evidence that it is caused by active VZV infection.58 ,62 VZV DNA has been found to persist in the saliva of 67% (21/32) of people with a past history of HZ up to 12 years after disease onset,70 but not in the saliva of healthy people.71
The finding of VZV DNA in blood mononuclear cells of patients who have HZ with PHN, in the arteries of patients with zoster-related strokes and, most recently, in temporal arteries of patients with possible and proven giant cell arteritis is helping to raise awareness of the devastating consequences of chronic active VZV infection and the potential for improved antiviral treatment of these conditions.72–74
In 2014, HZ was reported as a risk factor for myocardial infarction in addition to cerebrovascular disease.11–13 An editorial concludes, ‘The growing awareness of the role of VZV in vascular disease promises to lead to clinical trials to assess the benefit of antiviral therapy’.75
Herpetic eye disease study: oral antivirals to reduce recurrent ocular HSV disease
The herpetic eye disease study (HEDS) acyclovir prevention trial (APT) examined long-term use of oral acyclovir to prevent recurrent HSV disease, and found a 45% reduction (95% CI 0.41 to 0.75, p<0.001) in recurrent ocular disease over 1 year.63 On the basis of this landmark study, recommended care for HSV eye disease changed to include prolonged suppressive antiviral treatment. In HEDS APT, suppressive antiviral treatment for 1 year was most beneficial in preventing recurrence of stromal keratitis, reducing it from 28% to 14% (95% CI 0.29 to 0.80, p=0.005).63 A retrospective community-based cohort study also concluded that patients were significantly less likely to have recurrent HSV epithelial keratitis and stromal keratitis on prolonged suppressive treatment.76 There is an absence of direct evidence that viral replication contributes to either HZO or HSV stromal keratitis.
A retrospective study reported efficacy of suppressive antiviral treatment in both HSV and HZO disease. Immune status of patients was not reported. This study found that in patients with HZO, this treatment reduced the overall number of recurrences to 2.1 per year, compared with 3.4 episodes without antiviral treatment, a 35% reduction (p<0.05).60 The same treatment of patients with HSV keratitis reduced recurrences to 2.3 from 3.8, a 39% reduction (p<0.05). In both HZO and HSV, stromal keratitis and/or uveitis were the most common forms of recurrent disease.
Zoster eye disease study
The proposed zoster eye disease study (ZEDS) is analogous to the HEDS APT design. If funded by the National Eye Institute in the USA, study participants in the USA will be randomised in a double-masked, placebo-controlled trial to 1 year of oral valacyclovir 1000 mg daily or placebo, with follow-up every 3 months for a total of 18 months, to compare the rates of new or worsening anterior segment ocular disease during and after treatment. Valacyclovir, a prodrug of acyclovir, achieves a higher serum level of acyclovir, which is necessary due to the higher inhibitory concentration of VZV compared with HSV.77 Efficacy regarding incidence, severity and duration of PHN during and following treatment will also be assessed. Concluding as a result of this trial that valacyclovir is effective as suppressive treatment in patients with HZO in reducing ocular disease and/or PHN would be a major advance in management of HZO and possibly HZ in other locations.
References
Footnotes
Contributors The authors have contributed to and take responsibility for the content of the review article.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.