Article Text

Statistics from Altmetric.com
Birdshot retinochoroiditis: the origins of the disease name
Birdshot retinochoroiditis (BRC) is a uveitis predominantly affecting the posterior segment of the eye with dual, independent retinal and choroidal inflammation and almost only seen in Caucasians.1 ,2 Ryan and Maumenee first described the bilateral retinochoroidal inflammatory disease in early 1980, reporting on 13 patients.2 These authors called it ‘birdshot retinochoroidopathy’ because they found that lesions had a pattern comparable to that seen in wounds produced by birdshot shotguns. Later in 1980, Kaplan and Aaberg published a series of four similar cases ‘involving a choroidal and retinal pigment epithelium disease not previously described’, which they also called birdshot retinochoroidopathy.3 In 1981, Gass described 11 similar cases and called the disease vitiliginous chorioretinitis.4
In these first articles on the disease, clinicians had no choice but to rely on fundus examination and fluorescein angiography (FA). Therefore, the striking choroidal involvement seen on fundus examination was at the origin of the eponym the authors chose to give to the disease, because both ‘birdshot’ and ‘vitiliginous’ refer to the typical rice-shaped, depigmented choroidal birdshot fundus lesions (BFLs) that strongly and specifically characterised the condition. Of the two designations, ‘birdshot’ became the universally used and accepted term. It is understandable that such remarkable choroidal signs determined the naming of the disease because the retinal and FA signs were so much less specific and pathognomonic. Nevertheless, an important FA sign was noted by Gass, who observed retinal vasculitis of small and large vessels and the profuse leakage of fluorescein into the retina in the early disease, as well as a reduced presence of fluorescein in the large veins.4 He interpreted this feature as a substantial delay in retinal arteriovenous circulation, an explanation that was later shown to be inexact, thanks to the use of dual FA/indocyanine green angiography (ICGA) (see below).5 Retinal involvement was accounted for by calling the disease a retinochoroiditis or a chorioretinitis. Often the disease was also called a retinochoroidopathy or a chorioretinopathy, which was inadequate because it is clearly inflammatory, so that the suffix ‘-itis’ should have been used.
The importance of HLA-A29 histocompatibility antigen as a disease-defining criterion
Association of BRC with the HLA-A29 major tissue histocompatibility (MHC) antigen was first reported in 1982, 2 years after the entity was originally described.6 The association rate was estimated to be approximately 95% in subsequent reports.7 ,8 LeHoang et al9 found that BRC was associated with the HLA-A29-2 subtype, with a subsequent study confirming this link as well as an association with the HLA-A29-1 subtype.10 The HLA-A29 MHC antigen is present in around 7% of Caucasian populations.11 It is increasingly likely that the association is closer to 100% rather than >95% because false negatives were not so rare when the antibody testing method was used.12 The rate of false-negative results could be reduced with PCR-based testing.12 The disease has no known extraocular inflammation sites and yet features the strongest known HLA association with an MHC antigen with a greatly increased OR of 157.5 for the disease when the HLA-A29.02 allele is present.13 Truly HLA-A29-negative birdshot patients are a rarity if they exist at all, and restricting the diagnosis to PCR-positive HLA-A29 patients would exclude a very tiny proportion of cases, if any. Therefore, the presence of HLA-A29 antigen should be considered an essential criterion for diagnosing BRC.
ICGA is essential in detecting occult choroiditis and perform early diagnosis
Together with HLA testing, the second most important element that has drastically changed the appraisal of BRC was the fact that ICGA became available to image the choroid. ICGA first came into clinical use in the early 1990s and enabled insight into choroidal inflammation.14 One substantial advantage of this method was that it made possible the detection of occult choroidal lesions that were inaccessible using other investigational methods.15 ,16 ICGA allowed clinicians to subdivide choroidal inflammation into choriocapillaritis entities (eg, acute posterior multifocal placoid pigment epitheliopathy or idiopathic multifocal choroiditis) and stromal choroiditis (eg, Vogt-Koyanagi-Harada (VKH) disease and BRC).17 ,18
ICGA findings in BRC were standardised in 1999.19 Relevant ICGA signs for diagnosis and disease monitoring are the presence of hypofluorescent dark dots (HDDs) and fuzziness of large choroidal vessels. HDDs were suspected to arise from space-occupying stromal inflammatory foci, a hypothesis that Gaudio et al20 confirmed histopathologically. Many HDDs in BRC become isofluorescent on late angiographic frames, which indicates that (unlike in VKH) lesions do not occupy the full thickness of the choroidal stroma and do not involve the inner choroid.21 Fuzziness of choroidal vessels indicates vasculitis of large choroidal vessels.14
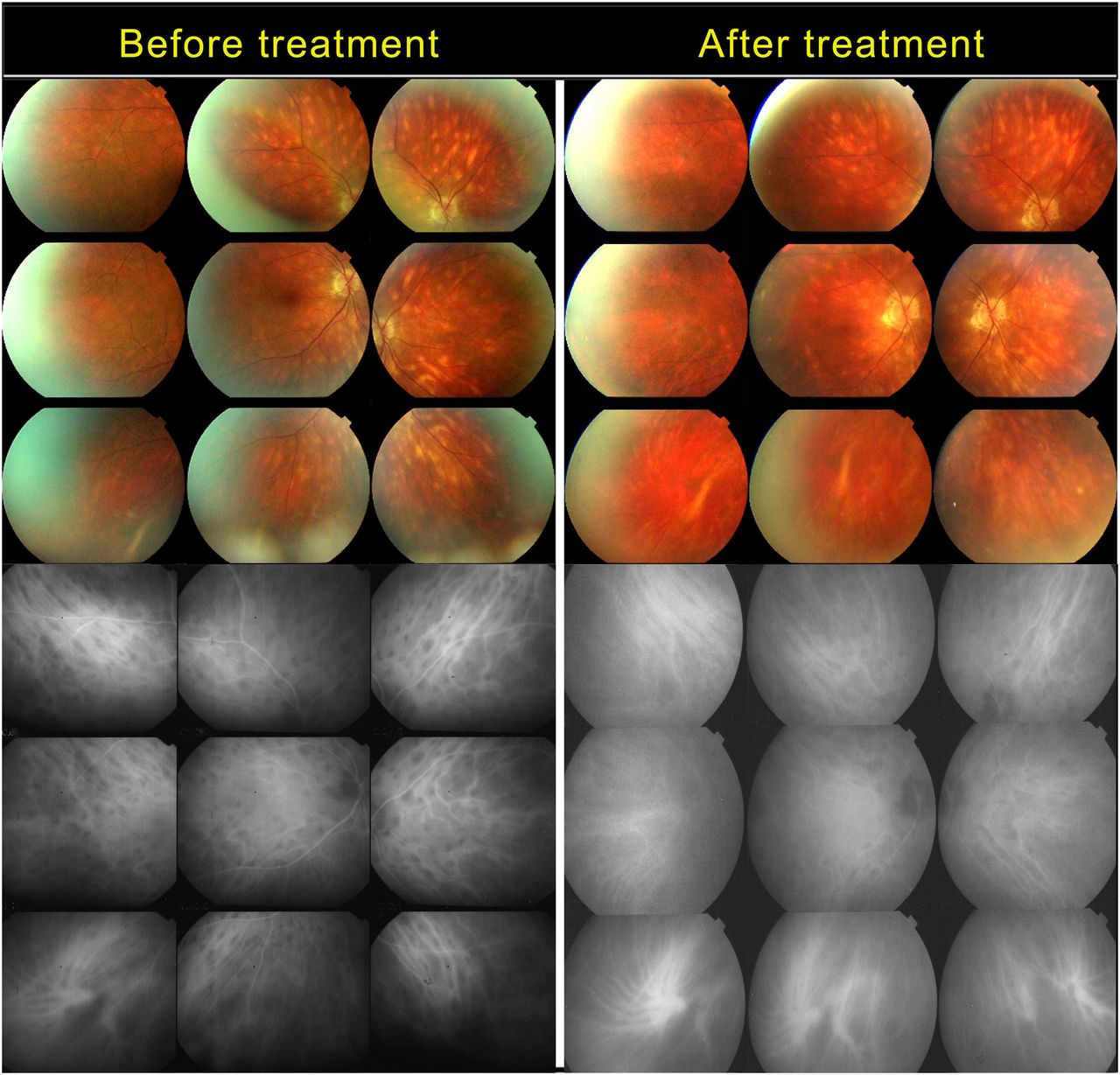
In several reports, HDDs were thought and reported to be the angiographic expression of BFLs.22 They are not, however, because we now know that BFLs are silent on ICGA and correspond to inactive depigmented cicatricial areas where pigment has been destroyed by the inflammatory mechanism. BFLs can coexist with HDDs, meaning that the disease has been present for some time and is still active (figure 1). On the other hand, HDDs may be absent in the presence of BFLs, meaning that the disease is no longer active and that what we see are simply areas devoid of melanocytes, marking regions of previously active stromal choroiditis (figure 1).
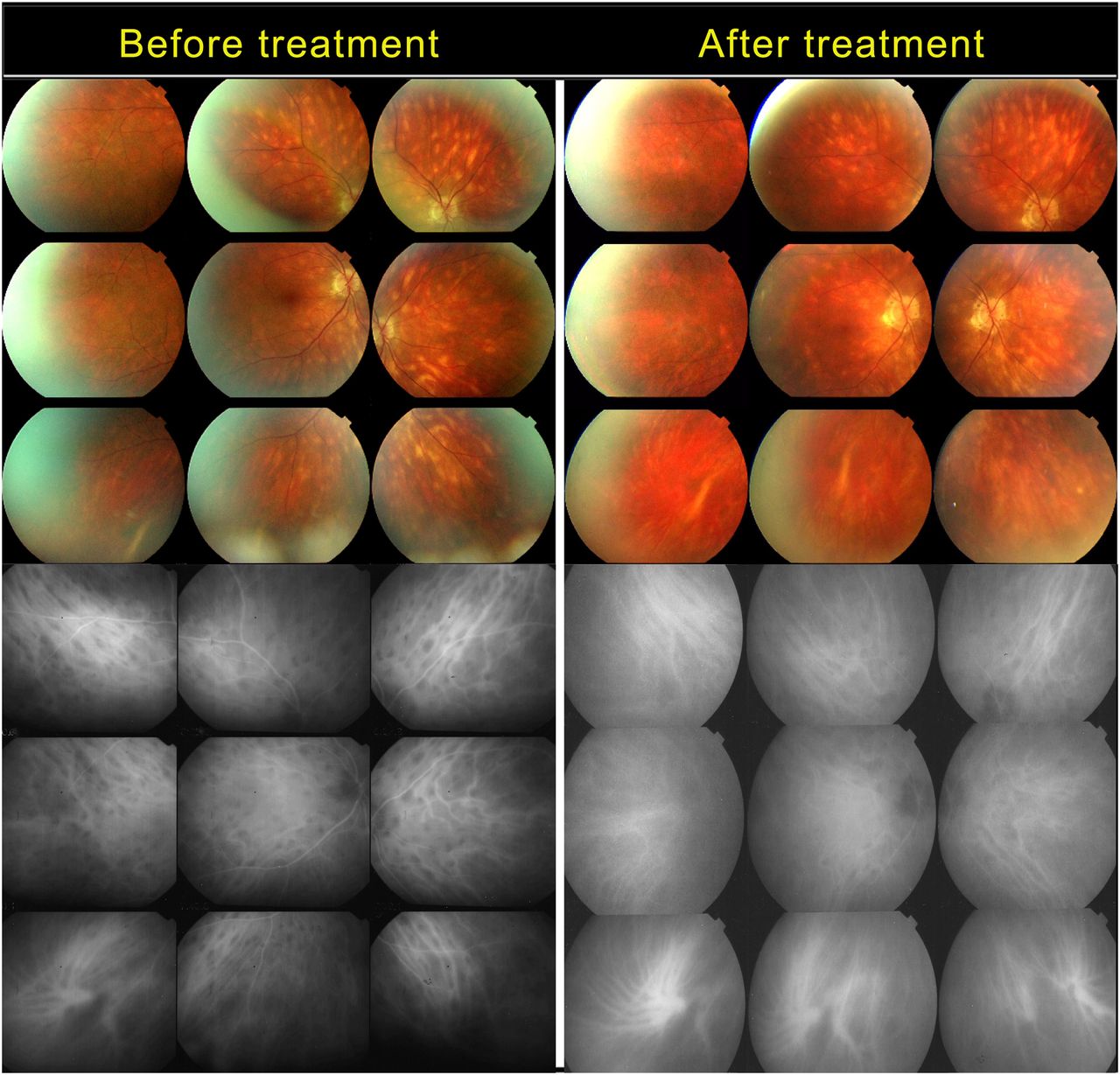
Birdshot fundus lesions (BFLs) do not correspond to hypofluorescent dark dots (HDDs). Case of birdshot retinochoroiditis that lasted for >5 years before the patient agreed to treatment. Top left: untreated patient; many BFLs are present in the fundus. Bottom left, indocyanine green angiography (ICGA) frame, the presence of numerous HDDs indicating active disease; however, there are more angiographically silent BFLs than HDDs. Top right: the fundus after 7 years of treatment with persisting BFLs. Bottom right: ICGA frame showing that neither resolved HDDs nor BFLs appear on ICGA (angiographically silent).
HDDs resolved in treatment-naïve patients with BRC having BFLs without affecting substantially their size or number,23 precisely because BFLs correspond to areas of depigmentation that no longer have any active inflammation once the stromal pigment islets have been ‘digested’. This explains why BRC fundus lesions are angiographically silent. The third scenario that can arise consists of HDDs without BFLs, indicating early disease before cicatricial depigmentation has occurred (see below) (figure 2).

(A) Case of birdshot retinochoroiditis diagnosed before birdshot fundus lesions (BFLs) were visible. Top: fundus pictures of the right and left eye. No BFLs seen. Middle: indocyanine green angiography (ICGA) showing numerous HDDs on both sides. Bottom: diffuse retinal vasculitis involving veins of all sizes with diffuse leakage. (B) Same case as (A) after 10 years of immunosuppressive therapy. Top: fundus pictures of right and left eye showing absence of typical BFLs. Middle: ICGA shows a totally normal choroid indicating that the choroid is responding easily to immunosuppressive therapy with resolution of all lesions. Bottom: fluorescein angiography (FA) shows that retinal vasculitis is substantially improved; however, discreet leakage is still present, and there is bilateral disc hyperfluorescence.
ICGA also demonstrated that choroidal and retinal inflammation develop independently, showing that areas of retinal capillary leakage seen on FA do not correspond to HDDs.24 Dual FA/ICGA makes it clear that choroidal inflammation promptly responds to therapy, whereas retinal inflammation is more resistant and is responsible for most of the symptoms and morbidity caused by the disease.25
ICGA also made it possible to explain the apparent perfusion delay of retinal veins reported by Gass, which in fact is a ‘pseudo-delay’ caused by massive extrusion of fluorescein into the retina, while ICGA retinal arteriovenous circulation time is normal.5
ICGA, crucial for early diagnosis/early treatment, modified the phenotype of BRC
By far the most important impact of ICGA in BRC was that choroidal involvement can be detected before the typical choroidal birdshot lesions are seen on funduscopy (figure 2).26 Moreover, among patients treated before the development of BFLs, the appearance of such lesions could be prevented altogether in five of six cases treated within a mean of 6.5 months of the onset of symptoms. In addition, such lesions were not observed during a mean follow-up period of 10 years under treatment, implying a change in the phenotype of BRC (figure 2).23 In this regard, BRC behaved like VKH, another stromal choroiditis in which early, aggressive and prolonged treatment can prevent the development of sunset glow fundus.27 The preponderant role of ICGA in BRC has been reported by several groups in Europe and recently also in the USA.19 ,28–30 Indeed, prevention of BRC fundus lesions requires early diagnosis, which is not possible with the present diagnostic criteria.
The need for appropriate diagnostic criteria of BRC
In 2006, a group of experts published research criteria for the diagnosis of BRC.31 However, these criteria fail to truly characterise BRC, especially early stage disease. The major shortcomings are the omission of ICGA signs, which are present in 100% of cases19 ,23; the lack of any reference to the visual field changes that are present in almost 100% of cases at presentation, depending on the onset of symptoms32 ,33; the characterisation of HLA-A29 antigen as a merely supporting factor, even though it is present in almost 100% of cases when PCR testing is used and the lack of acknowledgement that keratic precipitates cannot be an exclusion criterion because they are present in 15.8%–23% of treatment-naïve patients.2 ,4 ,34 In our series, the 3/19 (15.8%) patients with keratic precipitates had been evolving for more than 3 years without treatment.34
There is an urgent need for new and proper diagnostic criteria for the appropriate appraisal and management of BRC, especially for early disease. In our studies, we used the following criteria for the diagnosis of BRC: (1) presence of vitritis and retinal vasculitis in one or both eyes, (2) visual field anomalies in one or both eyes, (3) stromal choroiditis as evidenced by ICGA in both eyes (required), HLA-A29 antigen positivity (required) and absence of extraocular inflammation sites. An additional (but not any more requested) strongly suggestive criterion is the presence of BFLs. Such criteria are to be recommended for use in clinical practice as they correspond to the reality of the disease presentation (box 1).
Global diagnostic criteria for birdshot retinochoroiditis (BRC)/HLA-A29 uveitis
Presence of vitritis in one or both eyes (required)
Presence of retinal vasculitis in one or both eyes (required)
Stromal choroiditis, as evidenced by ICGA, in both eyes (required)
HLA-A29 antigen positivity (required)
Visual field anomalies in one or both eyes (supportive)
Absence of extraocular inflammatory site (supportive)
Presence of rice-shaped depigmented ‘birdshot lesions’ (BRC fundus lesions) (strongly supportive but not required)
BRC, birdshot retinochoroiditis; ICGA, indocyanine green angiography.
HLA-A29 uveitis, a more appropriate name for BRC?
In case of fulfilment of the above-listed clinical and investigational (especially angiographic) characteristics, birdshot cases can be expected to be associated with HLA-A29 positivity almost 100% of the time as long as PCR methodology is used; this rate is by far the highest known HLA association with a disease. Furthermore, if the diagnostic criteria cited here are used together with HLA-A29 determination, early diagnosis before the pathognomonic BFLs are seen, becomes possible. It would therefore be justified and even advisable to rename the disease after the most frequent characteristic element associated with it, the HLA-A29 antigen, which must be elevated to a disease-defining criterion. Indeed, in the early stage of disease, birdshot lesions are not disease defining, and classically relying on their presence leads to diagnostic delay when early diagnosis and treatment are so important.35
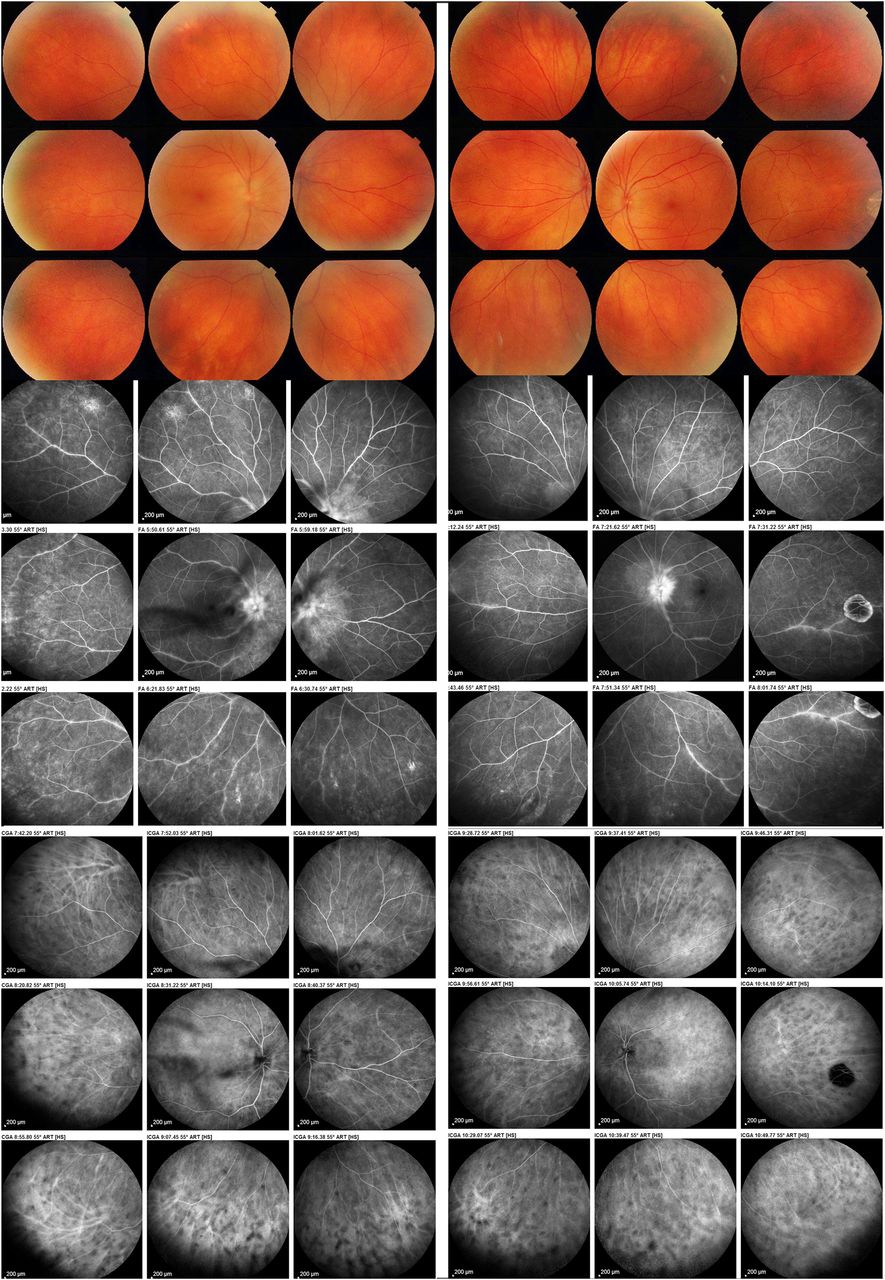
In practice, cases devoid of fundus lesions that were referred to us with vitritis and FA signs compatible with BRC usually were sent with the a diagnosis of retinal vasculitis (figure 3). When performing ICGA, which is absolutely necessary with such a constellation, the presence of bilateral ICGA angiographic signs including HDDs and fuzziness of vessels invariably led to HLA testing. HLA-A29 positivity confirmed the diagnosis in the absence of any BFLs, making HLA-A29 antigen rather than BFLs the hallmark of the disease.

{kind=link}
{kind=link}
{kind=link}
Case of birdshot retinochoroiditis without birdshot fundus lesions at presentation. The patient was referred for retinal vasculitis and also complained of floaters bilaterally. Posterior segment showed numerous vitreous opacities but no fundus lesions (top). Middle: diffuse retinal vasculitis in both eyes. Bottom: typical indocyanine green angiography signs of stromal choroiditis with numerous HDDs and non-recognizable pattern of choroidal vessels. The patient was immediately tested for the presence of HLA-A29 antigen, which was indeed positive.
Perspective and concluding remarks
BRC has been characterised by a strong clinical phenotype since its initial description. Subsequently, additional and even stronger investigational disease-defining criteria have become available. HLA-A29 histocompatibility antigen was first estimated to be present in up to 95% of BRC cases, but was finally found to be present in almost 100% of cases when PCR methodology was used.12 Long-neglected ICGA showed a stromal choroiditis in 100% of cases. Together, these two strong disease-defining criteria have opened the way to early diagnosis of the disease, no longer requiring the presence of BFLs, representing a diagnostic delay until BFLs appear. Recent data have even shown that in case of early and sustained treatment, birdshot lesions are prevented altogether, changing the phenotype of BRC.23 In this context of a disease without BFL, the traditional name no longer corresponds to the new reality of this clinical entity. To retain it could even have a deleterious effect on disease management by delaying therapeutic intervention during the wait for birdshot lesions to arise. ‘HLA-A29 uveitis’ more adequately reflects the current, updated clinical context. This name change would have the same implications as HLA-B27 uveitis because both terms reference diseases for which the etiopathogenicity is unknown but the exact course of the disease is well-established.
References
Footnotes
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.