Article Text

Abstract
Aim To compare the clinical outcomes of posterior chamber phakic intraocular lens implantation with a central hole (Hole Implantable Collamer Lens (ICL), STAAR Surgical) for low-to-moderate myopia and for high myopia.
Methods This multicentre retrospective case series comprised 351 eyes of 351 consecutive patients undergoing ICL implantation. Eyes were divided into groups based on preoperative degree of myopia: group 1; 57 eyes, manifest spherical equivalent less than −6 dioptres (D), and group 2; 294 eyes, −6 D or more. Safety, efficacy, predictability, stability and adverse events were compared preoperatively; and at 1 day, 1 week and 1, 3, 6 and 12 months postoperatively,
Results Uncorrected and corrected visual acuities were −0.17±0.14 and −0.21±0.10 logMAR in group 1, and −0.16±0.09 and −0.21±0.08 logMAR in group 2, 1 year postoperatively. In groups 1 and 2, 98% and 99% of eyes were within 1.0 D of the targeted correction. Manifest refraction changes of −0.12±0.34 D (group 1) and −0.18±0.43 D (group 2) occurred from 1 day to 1 year. ICL exchanges were necessary in two eyes (0.7%) in group 2. No vision-threatening complications occurred at any time.
Conclusions The ICL performed well for the correction of both low-to-moderate myopia and high myopia throughout the 1-year observation period. The clinical outcomes of ICL implantation for low-to-moderate myopia are essentially equivalent to those for high myopia.
- hole ICL
- phakic IOL
- safety
- efficacy
- predictability
- stability
- intraocular pressure
- endothelial cell density
- low-to-moderate myopia
- high myopia.
Statistics from Altmetric.com
- hole ICL
- phakic IOL
- safety
- efficacy
- predictability
- stability
- intraocular pressure
- endothelial cell density
- low-to-moderate myopia
- high myopia.
Introduction
The EVO Visian Implantable Collamer Lens (Hole ICL; STAAR Surgical, Monrovia, California, USA), a posterior chamber phakic intraocular lens with a central hole, has become widely accepted as a long-term effective approach for the correction of moderate-to-high myopia.1–5 The ICL provides several advantages in visual performance compared with laser in situ keratomileusis (LASIK), including less induction of higher order aberrations (HOAs), higher contrast sensitivity and higher retinal image magnification, not only in eyes with high myopia, but also in eyes with low-to-moderate myopia.6 7 To date, the surgical indication for ICL implantation is generally limited to high myopic eyes, and has not been indicated for low-to-moderate myopic eyes. Yet, the literature has shown promising results for ICL implantation in eyes with low-to-moderate myopia.7–9 To the best of our knowledge, no study has undertaken the direct comparison of the visual and refractive outcomes of ICL implantation for low-to-moderate myopia to high myopia. The purpose of the current study was to retrospectively evaluate the visual and refractive outcomes of ICL implantation in eyes with low-to-moderate myopia compared with eyes with high myopia in a large cohort of patients presenting at major clinical centres in Japan.
Patients and methods
Study population
The protocol was registered with the University Hospital Medical Information Network Clinical Trial Registry (000022043). Three hundred fifty-one (351) eyes of 351 consecutive patients (150 men and 201 women, mean age±SD, 33.8±7.3 years) who underwent implantation of the posterior chamber phakic ICL with a 0.36 mm central hole at six major Japanese medical institutions (Kitasato University Hospital, Sanno Hospital, Kobe Kanagawa Eye Clinic, Nagoya Eye Clinic, Oka Eye Clinic and Ray Eye Clinic) from January 2013 to March 2015, who regularly returned for postoperative examination and who completed a 1-year follow-up were retrospectively evaluated. Only one eye per subject was selected randomly for statistical analysis. This study was conducted as a collaborative work of the ICL Study Working Group in Japan. Eligible patients were divided into two groups, based on the preoperative degree of myopia (group1; low-to-moderate myopia, manifest spherical equivalent less than −6 D and group 2: high myopia, manifest spherical equivalent −6 D or more). If manifest cylinder was 1.25 D or less, 35 eyes in group 1 (61%) and 151 eyes in group 2 (51%) were implanted with a non-toric ICL. If manifest cylinder was 1.5 D or more, 22 eyes in group 1 (39%) and 143 eyes in group 2 (49%) were implanted with the toric ICL version. Before surgery, 1 day, 1 week and at 1, 3, 6 and 12 months after surgery, we compared the following parameters between the two groups: logarithm of the minimal angle of resolution (logMAR) of uncorrected distance visual acuity (UDVA), logMAR of corrected distance visual acuity (CDVA), manifest refraction (spherical equivalent), intraocular pressure (IOP). Endothelial cell density (ECD) was evaluated preoperatively, and 3 and 12 months postoperatively. We measured high-contrast visual acuity using a Snellen chart with Japanese letters at a distance of 5 m with best correction (but not with habitual correction) under photopic conditions (250 lux). All eyes underwent slit-lamp biomicroscopic and funduscopic examinations. Preoperatively, the horizontal white-to-white distance and anterior chamber depth were measured with scanning-slit topography, and the mean keratometric readings and the central corneal thickness were measured using an autorefractometre and an ultrasound pachymeter, respectively. The IOP was assessed using a non-contact tonometer, and the ECD was determined using a non-contact specular microscope. Eyes with keratoconus as determined by Placido disk topography were excluded from this study. Written informed consent for the ICL surgery was obtained from all patients. This retrospective review of the clinical charts was approved by the Institutional Review Board at Kitasato University and followed the tenets of the Declaration of Helsinki. Our Institutional Review Board waived the requirement for informed consent for this retrospective study.
Lens power calculation
The ICL power was calculated by using a modified vertex formula per the manufacturer’s instruction. In all eyes, emmetropia was selected as the target refraction to minimise preoperative refractive errors. The ICL size was selected based on the horizontal corneal diameter and the anterior chamber depth.
Surgical procedure
Dilating agents and topical anaesthesia were topically instilled on the day of surgery. After a viscosurgical device (OVD; Opegan; Santen, Osaka, Japan) was placed into the anterior chamber, model V4c ICL was inserted through a 3 mm clear corneal incision with the use of an injector cartridge. The ICL was placed in the posterior chamber using the manipulator. The OVD was washed out by a balanced salt solution, and a miotic agent was administrated. For toric ICL implantation, to control for potential cyclotorsion in the supine position, the zero horizontal axis was marked preoperatively by using a slit lamp. After the ICL was placed in the posterior chamber, it was rotated by 22.5° or less by using a manipulator. All surgeries were performed by experienced surgeons. Postoperatively, steroid (Rinderon; 0.1% betamethasone; Shionogi, Osaka, Japan) and antibiotic (Cravit; 0.5% levofloxacin; Santen, Osaka, Japan) medications were administered topically four times daily for 2 weeks, and then tapered.
Statistical analysis
Statistical analysis was conducted using a commercially available statistical software (Ekuseru-Toukei 2015, Social Survey Research Information, Tokyo, Japan). The normality of all data samples was first checked using the Kolmogorov-Smirnov test. Since the use of parametric statistics was not possible, the Friedman repeated measures analysis of variance (ANOVA) was used for the analysis of the time course of changes, and the Mann-Whitney U test was used to compare the data between the two groups. The Fisher’s exact test was used to compare the efficacy and predictability at 1-year postoperatively. Unless otherwise indicated, the results are expressed as mean±SD, and a value of p<0.05 was considered statistically significant.
Results
Study population
Preoperative demographics of the study population are summarised in table 1. No significant intraoperative complications occurred in any case. We found no significant differences in age (Mann-Whitney U test, p=0.32), gender (p=0.20), manifest cylinder (p=0.33), white-to-white distance (p=0.22), anterior chamber depth (p=0.13) and mean keratometric readings (p=0.10), but significant differences in preoperative manifest spherical equivalent (p<0.001), logMAR UDVA (p<0.001) and logMAR CDVA (p=0.001) between the two groups.
Preoperative demographics in eyes undergoing ICL implantation for low-to-moderate myopia and for high myopia
Safety outcomes
LogMAR CDVA was −0.21±0.10 (range, −0.30 to 0.30) in group 1 and −0.21±0.08 (range, −0.30 to 0.10) in group 2 at 1-year postoperatively (p=0.56). At 1-year postoperatively, in group 1, 36 eyes (63%) showed no change in CDVA, 13 eyes (23%) gained one line and 8 eyes (14%) lost one line, while in group 2, 142 eyes (48%) exhibited no change in CDVA, 112 eyes (38%) gained one line, 13 eyes (4%) gained two lines, 26 eyes (9%) lost one line and 1 eye (0.3%) lost two lines (figure 1).
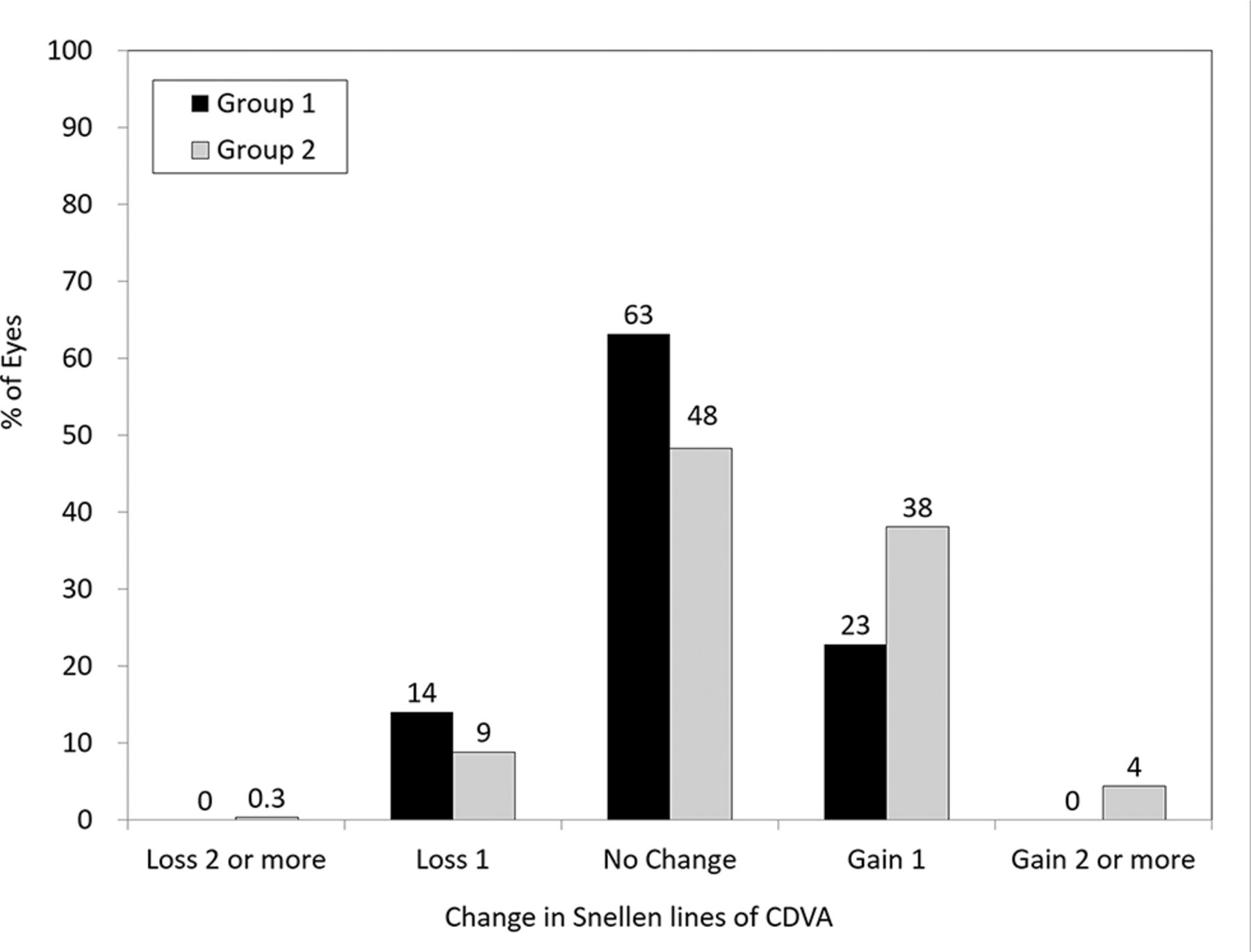
Changes in corrected distance visual acuity (CDVA) 1 year after implantable collamer lens implantation in eyes with low-to-moderate myopia and those with high myopia.
Effectiveness outcomes
At 1 year postoperatively, LogMAR UDVA was −0.17±0.14 (range, −0.30 to 0.30) in group 1 and −0.16±0.09 (range, −0.30 to 0.15) in group 2 (p=0.17). One day, 1 week and at 1, 3, 6 and 12 months postoperatively, 88%, 95%, 95%, 96%, 98% and 91% of eyes, respectively, in group 1% and 92%, 97%, 98%, 98%, 97% and 97% of eyes, respectively, in group two had UDVA of 20/20 or better (figure 2).

Cumulative percentages of eyes attaining specified cumulative levels of uncorrected distance visual acuity 1 year after implantable collamer lens implantation in eyes with low-to-moderate myopia and those with high myopia. D, day; M, month(s); W, week; Y, year.
Predictability
Figure 3 shows scatter plots of the attempted versus the achieved spherical equivalent correction. One day, 1 week and at 1, 3, 6 and 12 months postoperatively, 91%, 91%, 93%, 93%, 98% and 93% of eyes, respectively in group 1, 1% and 80%, 91%, 89%, 91%, 90% and 94% of eyes, respectively, in group 2 were within ±0.5 D of the attempted correction. One day, 1 week and at 1, 3, 6, and 12 months postoperatively, 100%, 100%, 100%, 98%, 100%, and 98% of eyes, respectively, in group 1, 1% and 95%, 98%, 98%, 99%, 99% and 99% of eyes, respectively, in group two were within ±1.0 D of the attempted correction.
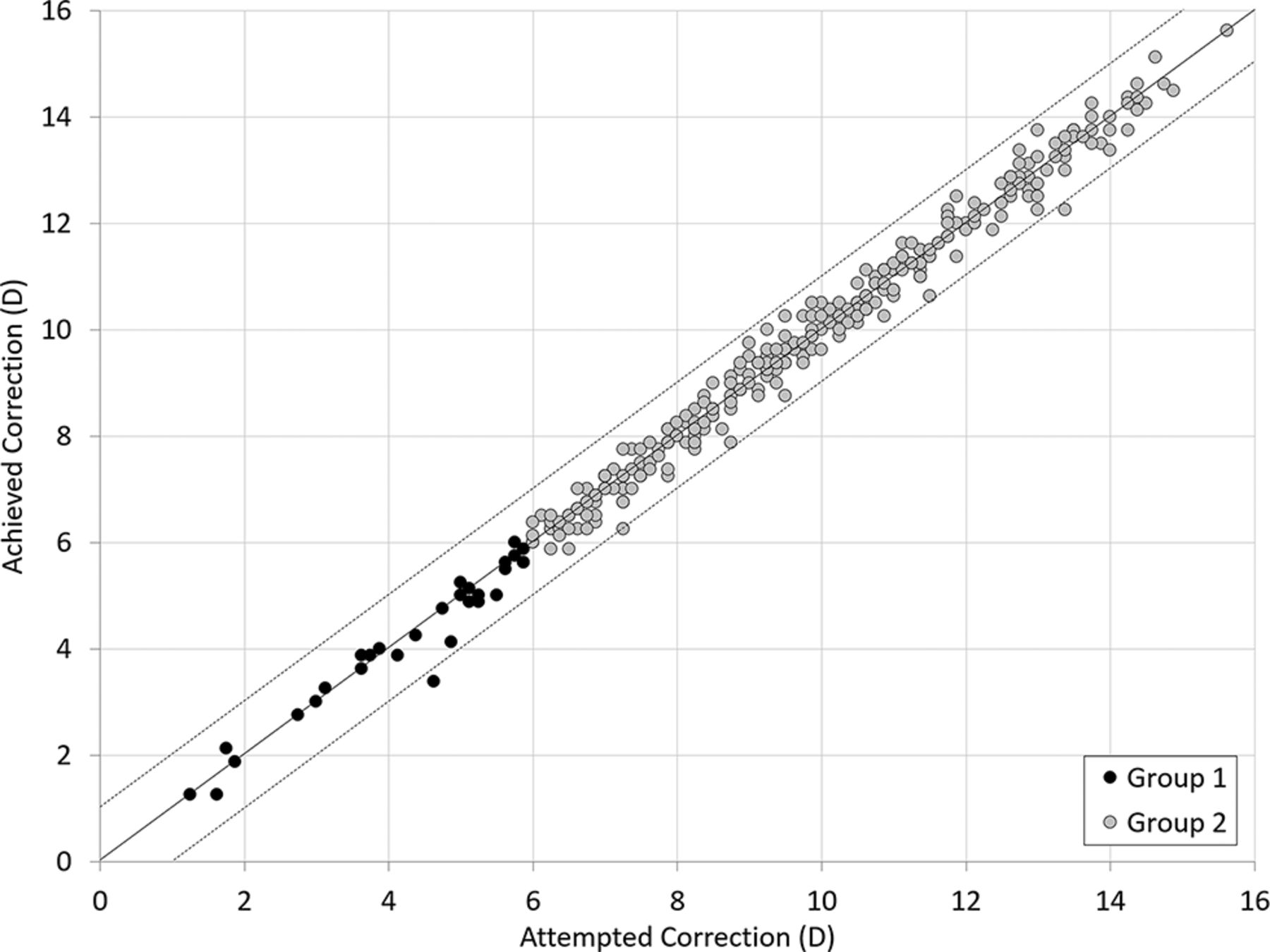
A scatter plot of the attempted versus the achieved manifest spherical equivalent correction 1 year after implantable collamer lens implantation in eyes with low-to-moderate myopia and those with high myopia.
Stability
Figure 4 shows the time-course changes in the manifest refraction. Changes in the manifest refraction from 1 day to 1 year were −0.12±0.34 D (range, −0.88 to 0.75 D) in group 1, and −0.18±0.43 D (range, −1.38 to 1.88 D) in group 2 (p=0.34).

Time course of manifest spherical equivalent after implantable collamer lens implantation in eyes with low-to-moderate myopia and those with high myopia. D, day; M, month(s); W, week; Y, year.
Intraocular pressure
Figure 5 shows the time-course changes in the IOP. We found significant changes in the IOP in group 1 (ANOVA, p<0.001) and in group 2 (p<0.001). Multiple comparisons using the Dunnett test demonstrated significant differences between measurements made preoperatively and at 1 day postoperatively (p<0.001), and preoperatively and 1 week postoperatively (p=0.03) in group 1. Multiple comparisons using the Dunnett test also demonstrated significant differences between measurements made preoperatively and 1 day postoperatively (p<0.001), and preoperatively and 1 week postoperatively (p<0.001) in group 2.

Time course of changes in intraocular pressure after implantable collamer lens implantation in eyes with low-to-moderate myopia and those with high myopia. D, day; M, month(s); W, week; Y, year.
Endothelial cell density
Figure 6 shows the time-course changes in the ECD. There was no statistically significant change in the ECD in group 1 (ANOVA, p=0.90) or in group 2 (p=0.24). The mean percentage of endothelial cell loss was 0.1%±9.7% and 0.1%±10.0% in groups 1 and 2, respectively, 1 year postoperatively (p=0.92).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Time course of changes in endothelial cell density after implantable collamer lens implantation in eyes with low-to-moderate myopia and those with high myopia. M, months, Y, year.
Secondary surgeries/adverse events
Of the 351 eyes, glare and/or halo were reported in five eyes (8.7%) and seven eyes (2.4%) in groups 1 and 2, respectively, but symptoms were mild and no secondary intervention was required. An ICL exchange occurred in two eyes (0.7%) in group 2, due to incorrect initial sizing or power. One eye (0.3%) developed significant axis rotation of the toric ICL (≥30°) in group 2. One eye (0. 3%) developed iritis due to unknown origin in group 2. One eye (0.3%) required LASIK due to undercorrection in group 2. No other vision-threatening complications were reported at any time throughout the 1-year observation period.
Discussion
The present study showed the ICL implantation is an effective treatment for both low-to-moderate and high myopia, with excellent safety, predictability and stability throughout a 1-year observation period. To expand the surgical indication of the ICL to include low-to-moderate myopia, it is essential to directly compare the visual and refractive outcomes and the adverse events in eyes with low-to-moderate myopia to eyes with high myopia.
Until now, there have been only a few published studies on ICL implantation for low-to-moderate myopia, and all studies have concentrated on comparing the visual performance post-ICL implantation to visual performance post-LASIK. Sanders et al first reported that ICL implantation had advantages over LASIK even in eyes with low myopia.8 Sanders et al later showed that ICL implantation was superior to LASIK in terms of safety, efficacy, predictability and stability for myopia of −3.00 to −7.88 D with matching preoperative data.9 We previously demonstrated that ICL implantation induced significantly fewer ocular HOAs than did wavefront-guided LASIK even in low-to-moderate myopic eyes7; we further demonstrated that ICL implantation significantly increases contrast sensitivity, whereas wavefront-guided LASIK does not.7 This is presumably because the laser ablation associated with LASIK creates a more oblate cornea, which results more surgically induced HOAs,10 11 and because retinal magnification after ICL implantation is reduced to a lesser extent than after LASIK.12–14
Both the postoperative UDVA and the refractive stability in group 1 were significantly better than in group 2, possibly because group 1 had better preoperative UDVA and lower rates of myopia than group 2. Otherwise, our remaining results in group 1 were comparable with those in group 2, indicating that the clinical outcomes of ICL implantation for low-to-moderate myopia was almost equivalent to those for high myopia.
Our study represents the first multicentre comparative study on visual and refractive outcomes and adverse events of ICL implantation between eyes with low-to-moderate myopia and eyes with high myopia. Moreover, no vision-threatening complications occurred in any case during the 1-year follow-up period. Based on these 1-year comparative findings, we believe that the surgical indication for ICL implantation can be expanded to include the correction of low-to-moderate myopia.
There are some concerns about postoperative complications after ICL implantation, including IOP rise (including pupillary block), corneal endothelial cell loss and cataract formation. In this study, we did not find any significant differences in either IOP rise or ECD loss in any case during the follow-up period. Our findings support those of earlier studies on Hole ICL implantation, even when preoperative laser iridotomy or intraoperative peripheral iridectomy was not performed.15–17 We found no cataract formation in any case throughout the 1-year follow-up. Kawamorita et al used computational fluid dynamics to show that Hole ICLs may improve the circulation of aqueous humour to the anterior surface of the crystalline lens.18 Packer et al reported that previous studies on Hole ICL implantation including data on 1291 eyes followed for up to 5 years describe a zero incidence of asymptomatic anterior subcapsular cataract formation.19 More prolonged careful follow-up is still required to determine the exact rate of cataract formation in Hole ICL-implanted eyes.
This study has several limitations. First, the study was performed in a retrospective fashion. Although this is a multicentre study in a large cohort of patients undergoing ICL implantation, a prospective randomised study would be ideal for confirming our results. Second, ICL surgery was performed by multiple experienced surgeons, and thus there were some variations in the use of surgical devices and drugs. Third, only consecutive patients who completed a 1-year follow-up were included in this study. Since the patients who were satisfied with their visual performance after refractive surgery tended to be lost to the follow-up, our longitudinal data may have a possible source of selection bias. In conclusion, this multicentre comparative study supports the view that the ICL performed equally well in the correction of low-to-moderate myopia as it did in high myopia during the 1-year observation period. ICL implantation for low-to-moderate myopia is clinically, if not statistically, equivalent to results in high myopia in terms of the safety, efficacy, predictability and stability. ICL implantation is a viable surgical option for the treatment of low-to-moderate myopia.
References
Footnotes
Contributors The authors were involved in the conception or design of the work, the acquisition, analysis or interpretation of data for the work (KK, KS, AI, YK, TK, TN, YO, RM); drafting the work or revising it critically for important intellectual content (KK, AI); final approval of the version to be published (KK, KS, AI, YK, TK, TN, YO, RM); agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved (KK, KS, AI, YK, TK, TN, YO, RM).
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests KS was a consultant to STAAR Surgical. YK is a paid consultant for STAAR Surgical. The other authors have no commercial or proprietary interest in the product or company described in the current article.
Patient consent Obtained.
Ethics approval IRB of Kitasato University.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance