Article Text

Statistics from Altmetric.com
Case report
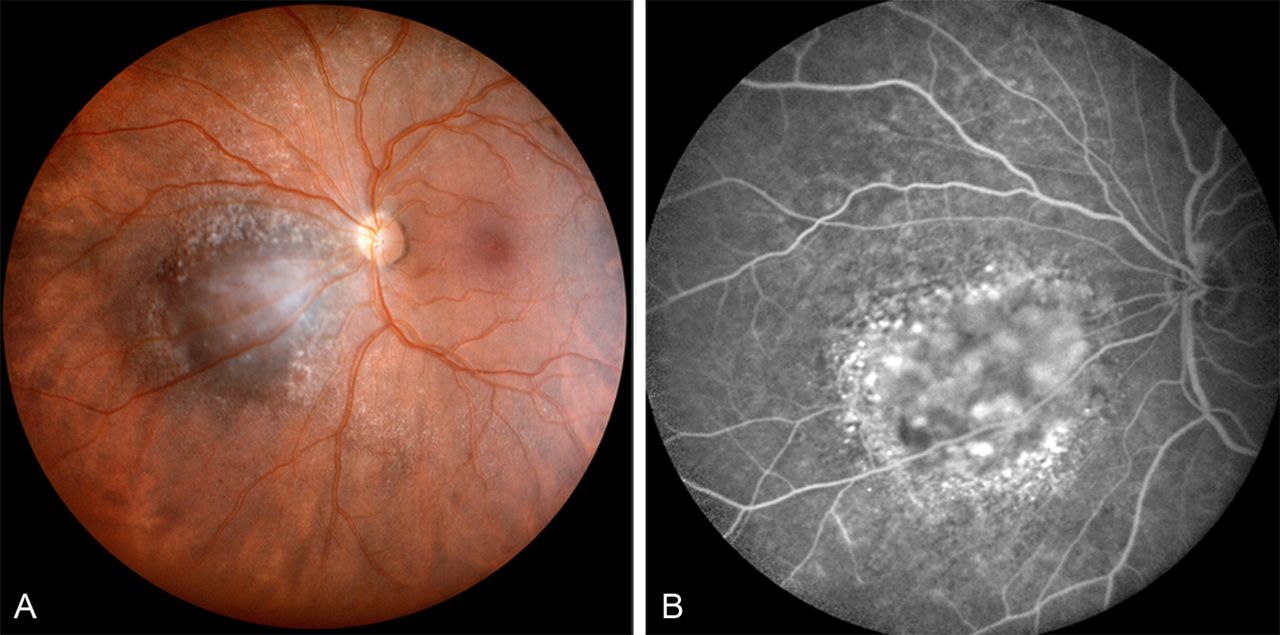
A 68-year-old lady was referred to the Jules-Gonin Eye Hospital (Lausanne, Switzerland), 6 months after her ophthalmologist had observed, during routine eye examination, an asymptomatic, parapapillary, choroidal pigmented tumour in the left eye, covered with drusen and without any orange pigment or associated serous retinal detachment (figure 1A).

(A) Panoramic fundus picture (PANORET camera) of a small pigmented parapapillary choroidal tumour covered with drusen and without orange pigment at its surface. (B) On fluorescein angiography, the absence of an associated serous retinal detachment or leaking ‘pin points’ is confirmed, as well as the presence of pigment epithelial alterations at the lesion's periphery.
Best corrected Snellen visual acuity was 0.7 in the right eye, related to a relative hypermetropic amblyopia known since childhood, and 1.0 in the left eye. On fluorescein angiography, pigment epithelial alterations were present, with limited diffusion of the dye (figure 1B).
Questions
-
What is your diagnosis?
-
How would you manage?
-
What is the prognosis?
For answers see 1539.
Answers
For questions see 1530
-
In order for the work-up of a pigmented choroidal tumour to be complete, a B-scan ultrasonography must be performed. All the while confirming the ophthalmoscopic impression that this was an intraocular tumour with a limited thickness (height (H)=2.5 mm), echography revealed the surprising presence of a large extrascleral extension (H=6.0 mm) (figure 2A). The diagnosis of a presumed small choroidal melanoma hiding a large extrascleral extension was made.
-
The usual general check-up for uveal melanoma including a liver scan did not show distant metastases. In addition, a high definition orbital MRI (3 Tesla) with gadolinium injection was organised, on which the extrascleral extension appeared to be circumscribed without invasion of the optic nerve sheath (figure 2B). Extraocular extensions have been demonstrated to occur through emissary scleral channels, in this case a posterior ciliary artery, rather than an erosion of the sclera.1 As both the ultrasound and MRI images did not suggest the contrary, a conservative therapeutic approach including excision of the extraocular extension followed by proton therapy was proposed, to which the patient agreed. During tantalum clip surgery, the extrascleral tumour nodule could be easily isolated from both the intact sclera and the surrounding orbital tissues, and was subsequently removed (figure 2C). Two weeks later, the intraocular tumour was irradiated with external proton beam irradiation, delivering 60 Gray in four fractions over four consecutive days,2 with posterior safety margins increased with 3 mm to include the orbital tissues surrounding the site of the previously excised extraocular extension in the target volume.
Six months later, the tumour was reduced to a flat scar, with a thickness of 1.2 mm and no signs of an orbital recurrence on B-scan ultrasonography.
-
On histopathological examination, the extrascleral extension consisted of mixed type (fusiform and epithelioid) uveal melanoma cells (figure 2D), with the epithelioid cells displaying prominent nucleoli and a back-to-back loop vascular pattern. The immunohistochemic proliferation index (Ki67) was about 5%. These elements have been classically correlated with a poor vital prognosis.
Cytogenetic analysis (array-comparative genomic hybridisation or array-CGH) was also performed, revealing a complete gain of the entire chromosome 20 and a partial amplification and gain of chromosome 6p, but without monosomy 3 or 8q gains. According to the recent literature, and assuming that this analysis is also representative of the intraocular tumour part, such a result is correlated with a low metastatic risk.3

{kind=link}
{kind=link}
(A) B-scan ultrasonography reveals the presence of an extrascleral extension, close to the optic nerve and surprisingly large (height (H)=6.0 mm), compared with the intraocular tumour part (H=2.5 mm). (B) A high definition (3 Tesla) MRI of the orbit gives the image of a circumscribed extraocular tumour, without evidence of optic nerve sheath invasion (T1, with gadolinium). (C) Macroscopic image of the excised encapsulated extraocular extension. (D) Histopathological analysis demonstrates an infiltration of the scleral and peri-scleral connective tissue by a proliferation of epithelioid and fusiform melanoma cells, isolated or organised in large, sometimes confluent nests or sheets (H&E stain; original magnification ×126).
Discussion
This case report illustrates the challenges with regard to the diagnosis, management and prognosis of a small choroidal melanoma hiding a large extrascleral extension.
The ophthalmoscopic and angiographic characteristics of this pseudo small pigmented parapapillary tumour were closer to those of a large nevus (absence of symptoms, orange pigment, or serous retinal detachment and presence of drusen and pigment epithelial alterations) than those of a melanocytic tumour at risk of growth.4 ,5 Even the thickness of the intraocular tumour did not exceed 3 mm. However, the presence of an extrascleral extension on B-scan ultrasonography changed the diagnosis and subsequent management and prognosis completely. Choroidal nevi are quite frequent in Caucasians, with an estimated prevalence between 5% and 8%6 against an annual incidence of about 5–7/million for choroidal melanoma.6 ,7 Consequently, it might be tempting for the general ophthalmologist in a busy practice not to refer a patient with a slightly elevated nevus for B-scan ultrasonography or to defer it, with the ulterior risk of conservative treatment becoming difficult or even impossible. Our patient experienced for this very reason a delay in referral of 6 months.
An extrascleral extension, present in 2%–15% of all uveal melanomas,1 ,2 ,8 ,9 ,10 invariably raises the question whether—in analogy to the dermatologists’ approach of cutaneous melanoma—orbital exenteration, or at least adjuvant orbital irradiation, is indicated. With regard to local tumour control, the presence of an extraocular extension has not been shown to be a significant risk factor for local recurrence after conservative proton therapy.2 ,8 ,10 With regard to survival, the Collaborative Ocular Melanoma Study (COMS report nr 24) found no survival advantage attributable to pre-enucleation radiation of the orbit,11 albeit with only 20 Gray, despite the presence of an extrascleral extension in 8.2% of all eyes with uveal melanoma primarily enucleated in the frame of this study.9 A similar study using an effective 60 Gray irradiating the whole orbit has not been undertaken yet, researchers probably being discouraged by the major radiation side effects described for other orbital tumours without a therapeutic alternative.12
With the introduction of cytogenetic and molecular tests, uveal melanoma prognostication has become a hot topic in recent literature and different techniques are being evaluated, such as FISH, array-CGH, multiplex ligation-dependent probe amplification (MLPA) and gene expression profiling. All researchers agree that the presence of monosomy 3 is the most important metastatic risk factor. Damato et al even found that some ‘traditional’, clinical risk factors, such as extraocular extension, lost significance when cytogenetic and histological data were included in their statistical prognostication model.3 Though these prognostic tests have changed profoundly the research on uveal melanoma, effective ‘tailored’ adjuvant therapies preventing metastatic disease have yet to be developed.
In conclusion, B-scan ultrasonography belongs to the basic work-up of small melanocytic tumours. The presence of a large encapsulated extrascleral extension is not necessarily a contraindication for conservative treatment, all the while requiring enlarged radiation safety margins. Following surgical resection, the extrascleral tumour part can be used for cytogenetic analysis, prognostication and defining the terms of oncological follow-up. However, no effective adjuvant treatment based on specific cytogenetic tumour characteristics has been developed yet.
References
Footnotes
-
Contributors The four authors are justifiably credited with authorship according to the authorship criteria. In detail, DP, AS, LZ: conception, design, analysis and interpretation of data, drafting of the manuscript, final approval given. APM: critical revision of manuscript analysis and interpretation of data, final approval given.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.