Article Text

Abstract
Aim To determine the effects of pupil size on uncorrected visual acuity (UCVA) in astigmatic eyes.
Methods The authors examined 20 normal eyes of 20 healthy volunteers (age 26.7±4.9 years (mean±SD); 8 men, 12 women). After fully correcting cycloplegic refraction, the authors created with-the-rule and against-the-rule astigmatism of 1, 2, and 3 dioptres (D) in each eye, and then assessed UCVA using artificial pupils (1 to 5 mm) in these astigmatic eyes. Measurements were performed three times, and the mean value was used for statistical analysis.
Results In eyes with with-the-rule astigmatism of 1, 2 and 3 D, logMAR UCVA was 0.04±0.08, 0.09±0.09 and 0.16±0.16 for 1 mm pupils, −0.01±0.09, 0.12±0.15 and 0.33±0.24 for 2 mm pupils, 0.02±0.09, 0.20±0.19 and 0.46±0.30 for 3 mm pupils, 0.02±0.08, 0.24±0.20 and 0.48±0.21 for 4 mm pupils, and 0.08±0.10, 0.33±0.18 and 0.53±0.22 for 5 mm pupils, respectively. The variance of the data was statistically significant (p=0.03 for 1 D, p<0.001 for 2 D, p<0.001 for 3 D, analysis of variance). Similar results were obtained in eyes with against-the-rule astigmatism.
Conclusions Both the amount of astigmatism and the pupil size can affect UCVA in astigmatic eyes. It is suggested that not only the amount of astigmatism but also the pupil size should be taken into consideration for acquiring better visual performance in astigmatic eyes.
- Astigmatism
- pupil size
- visual acuity
- optics and refraction
- treatment surgery
Statistics from Altmetric.com
Introduction
Since astigmatic errors can lead to both a decrease in uncorrected visual acuity (UCVA) and deterioration of quality of vision, reducing this pre-existing astigmatism and acquiring good visual outcomes are two essentials for minimising spectacle dependence and maximising subsequent patient satisfaction. Several surgical options for the correction of astigmatism have been advocated, such as laser in situ keratomileusis, photorefractive keratectomy, astigmatic keratotomy using limbal or corneal relaxing incisions, the use of a toric phakic or pseudophakic intraocular lens, and other excimer laser refractive procedures. At present, we merely consider the amount of astigmatism as well as the axis of astigmatism for these surgical approaches. However, it is known that pupil size plays an important role in the refractive outcomes of the surgical procedure.1–5 To our knowledge, the effects of pupil diameter on visual performance in astigmatic eyes have not been investigated so far and still remain unclear. The purpose of this study is to prospectively evaluate the effects of pupil size on visual acuity in eyes with astigmatism.
Materials and methods
Twenty eyes of 20 healthy volunteers (eight men and 12 women; ages 26.7±4.9 years (mean age±SD; range, from 22 to 37 years old)) who had no ophthalmic diseases other than refractive errors were enrolled in this prospective study. The manifest refraction (spherical equivalent) was −1.69±2.20 dioptres (D) (range −6.25 to 0.75 D). The manifest refractive cylinder was −0.11±0.25 D (range −0.75 to 0.00 D). Corneal and ocular higher-order aberrations (HOAs) determined using Hartmann–Shack aberrometry (KR-9000, Topcon, Tokyo, Japan) were 0.06±0.02 μm (range 0.04 to 0.10 μm), and 0.10±0.02 μm (range 0.05 to 0.16 μm) for a 4 mm pupil, respectively. Eyes with keratoconus were excluded from the study by using the keratoconus screening test of Placido disk videokeratography (TMS-2, Tomey, Nagoya, Japan). Informed consent was obtained from all volunteers in accordance with institutional guidelines, according to the tenets of the Declaration of Helsinki.
After corneal anaesthesia was obtained using one drop of oxybuprocaine (Benoxil; Santen, Osaka, Japan), cycloplegia was achieved with three drops of 1% cyclopentolate hydrochloride (Cyplegin; Santen), spaced 5 min apart.6 7 Autorefraction (ARK-700A; Nidek, Gamagori, Japan) was undertaken at least 30 min after the third administration of cyclopentolate hydrochloride and only if the pupillary light reflex was absent. After fully correcting cycloplegic refraction, we produced with-the-rule (WTR) (axis 90°) and against-the-rule (ATR) (axis 0°) astigmatism of 1, 2 and 3 D in each eye. We assessed UCVA using artificial pupils (1 to 5 mm) in these eyes. Only right eyes were tested. We carried out this measurement three times, and the average value was used for the analysis.
All statistical analyses were performed using SPSS. Repeated-measures analysis of variance (ANOVA), followed by the Dunnett post hoc test for multiple comparisons, was used to compare the differences between groups with different pupil sizes. The results are expressed as mean±SD, and a p value of <0.05 was considered statistically significant.
Results
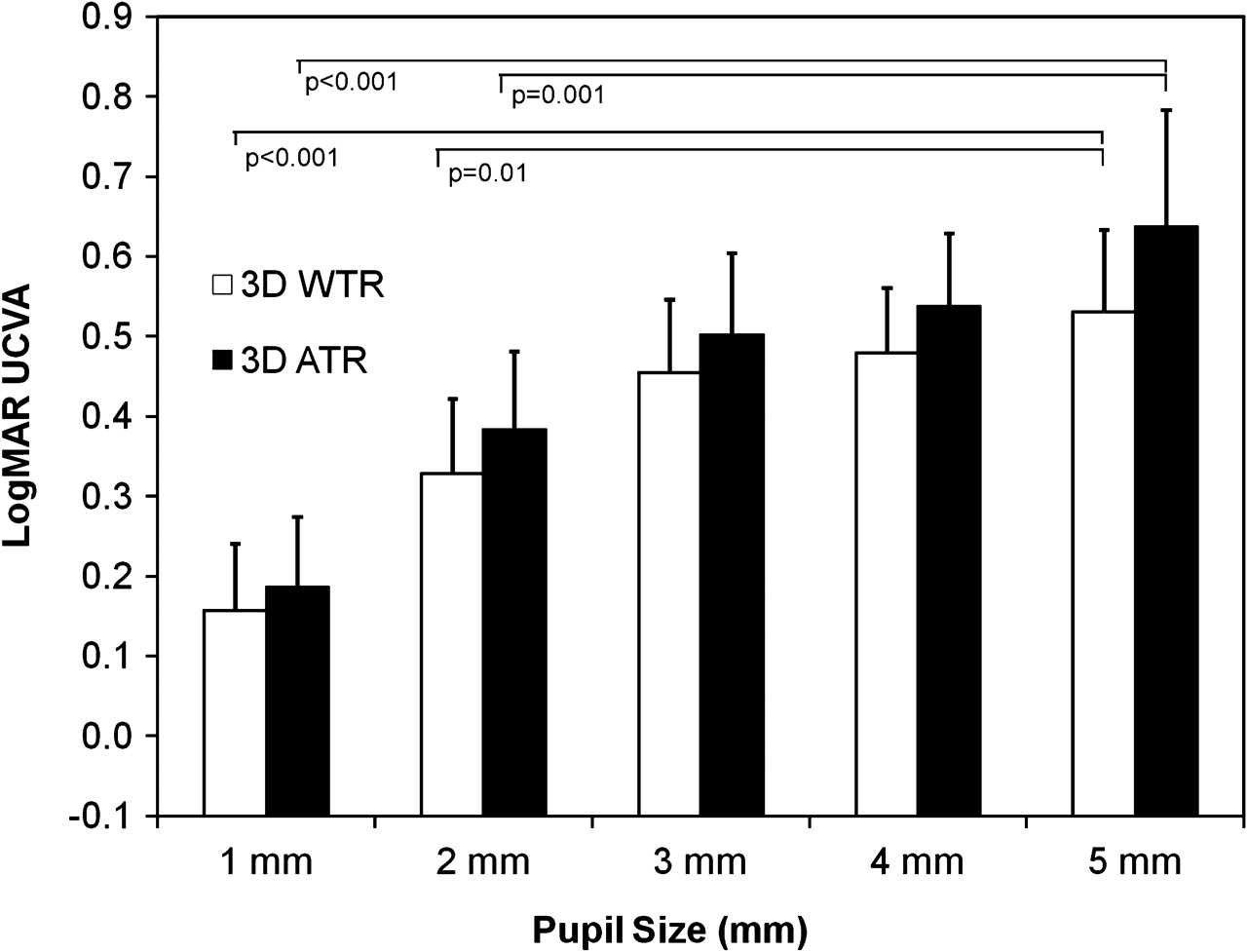
In eyes with a WTR astigmatism of 1 D, logMAR UCVA was 0.04±0.08, −0.01±0.09, 0.02±0.09, 0.02±0.08 and 0.08±0.10, for 1, 2, 3, 4 and 5 mm pupils, respectively (figure 1). The variance of the data was statistically significant (p=0.03, ANOVA). Multiple comparisons demonstrated a significant difference between measurements made for a 2 mm pupil and for a 5 mm pupil (p=0.004, Dunnett test), for a 3 mm pupil and a 5 mm pupil (p=0.05), and for a 4 mm pupil and a 5 mm pupil (p=0.05), but no significant differences between those made for a 1 mm pupil and a 5 mm pupil (p=0.21). In eyes with a WTR astigmatism of 2 D, logMAR UCVA was 0.09±0.09, 0.12±0.15, 0.20±0.19, 0.24±0.20 and 0.33±0.18, for 1, 2, 3, 4 and 5 mm pupils, respectively (figure 2). The variance of the data was statistically significant (p<0.001, ANOVA). Multiple comparisons demonstrated a significant difference between measurements made for a 1 mm pupil and for a 5 mm pupil (p<0.001), for a 2 mm pupil and a 5 mm pupil (p<0.001), and for a 3 mm pupil and a 5 mm pupil (p=0.02), but no significant differences between those made for a 4 mm pupil and a 5 mm pupil (p=0.13). In eyes with WTR astigmatism of 3 D, logMAR UCVA was 0.16±0.16, 0.33±0.24, 0.46±0.30, 0.48±0.21 and 0.53±0.22, for 1, 2, 3, 4 and 5 mm pupils, respectively (figure 3). The variance of the data was statistically significant (p<0.001, ANOVA). Multiple comparisons demonstrated a significant difference between measurements made for a 1 mm pupil and a 5 mm pupil (p<0.001), and for a 2 mm pupil and a 5 mm pupil (p=0.01), but no significant differences between those made for a 3 mm pupil and a 5 mm pupil (p=0.36), or for a 4 mm pupil and a 5 mm pupil (p=0.51).
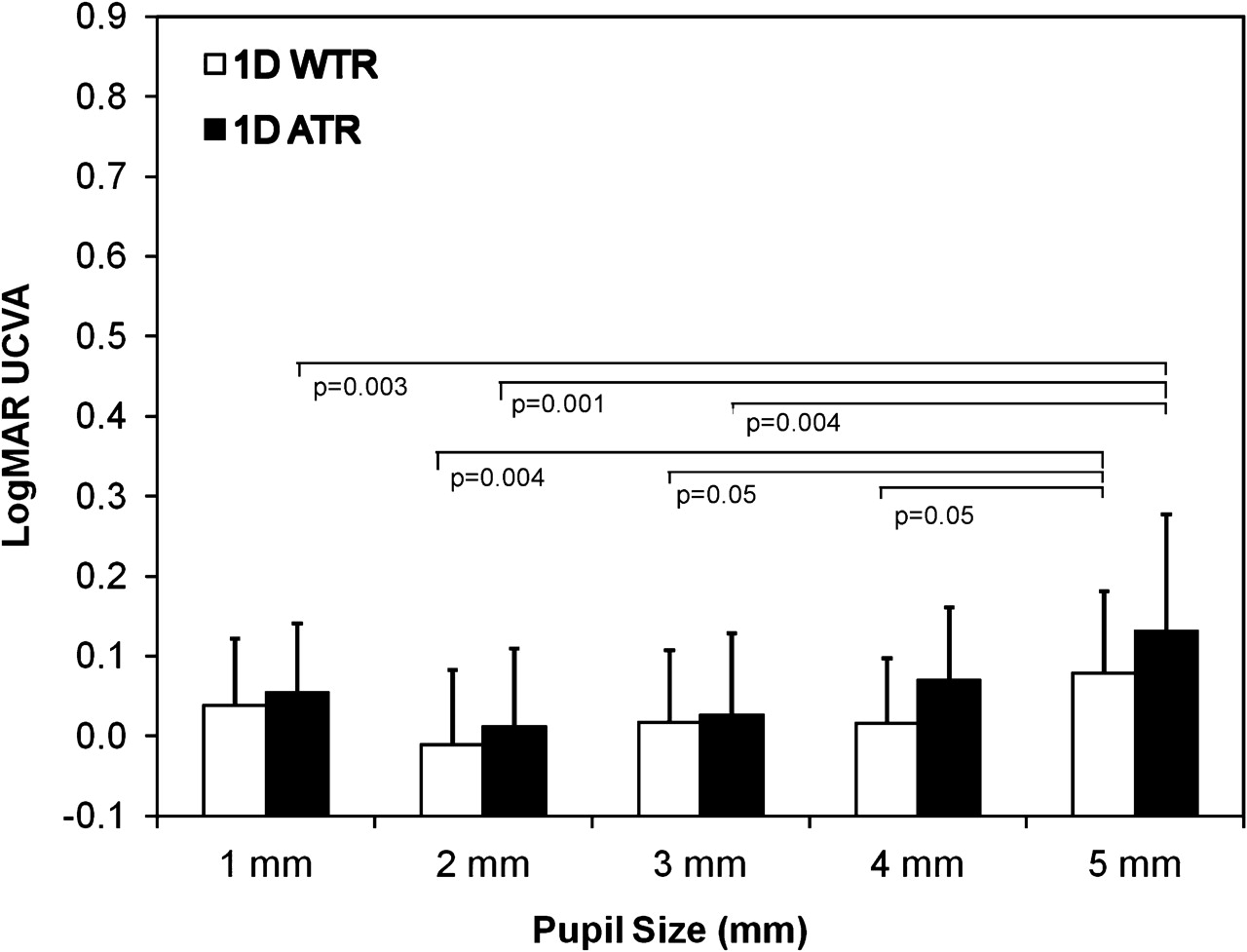
Uncorrected visual acuity (UCVA) as a function of pupil diameter in eyes with 1 dioptres of with-the-rule (WTR) and against-the-rule (ATR) astigmatism.

Uncorrected visual acuity (UCVA) as a function of pupil diameter in eyes with 2 dioptres of with-the-rule (WTR) and against-the-rule (ATR) astigmatism.
{kind=link}
{kind=link}
{kind=link}
Uncorrected visual acuity (UCVA) as a function of pupil diameter in eyes with 3 dioptres of with-the-rule (WTR) and against-the-rule (ATR) astigmatism.
Similarly, in eyes with an ATR astigmatism of 1 D, logMAR UCVA was 0.05±0.09, 0.01±0.10, 0.03±0.10, 0.07±0.09 and 0.13±0.15, for 1, 2, 3, 4 and 5 mm pupils, respectively (figure 1). The variance of the data was statistically significant (p=0.006, ANOVA). Multiple comparisons demonstrated a significant difference between measurements made for a 1 mm pupil and for a 5 mm pupil (p=0.03), for a 2 mm pupil and a 5 mm pupil (p=0.001), and for a 3 mm pupil and a 5 mm pupil (p=0.004), but no significant differences between those made for a 4 mm pupil and a 5 mm pupil (p=0.10). In eyes with ATR astigmatism of 2 D, logMAR UCVA was 0.11±0.10, 0.17±0.15, 0.27±0.20, 0.32±0.19 and 0.44±0.22, for 1, 2, 3, 4 and 5 mm pupils, respectively (figure 2). The variance of the data was statistically significant (p<0.001, ANOVA). Multiple comparisons demonstrated a significant difference between measurements made for a 1 mm pupil and for a 5 mm pupil (p<0.001), for a 2 mm pupil and a 5 mm pupil (p<0.001), and for a 3 mm pupil and a 5 mm pupil (p=0.007), but no significant differences between those made for a 4 mm pupil and a 5 mm pupil (p=0.06). In eyes with ATR astigmatism of 3 D, logMAR UCVA was 0.19±0.14, 0.38±0.23, 0.50±0.26, 0.54±0.24 and 0.64±0.23, for 1, 2, 3, 4 and 5 mm pupils, respectively (figure 3). The variance of the data was statistically significant (p<0.001, ANOVA). Multiple comparisons demonstrated a significant difference between measurements made for a 1 mm pupil and for a 5 mm pupil (p<0.001), and for a 2 mm pupil and a 5 mm pupil (p=0.001), but no significant difference between those made for a 3 mm pupil and a 5 mm pupil (p=0.09), or for a 4 mm pupil and a 5 mm pupil (p=0.22).
Discussion
The results of our study have revealed that UCVA was better in eyes with smaller pupil sizes in almost all cases in which both WTR and ATR astigmatism was present, which was in good agreement with their previous studies on non-astigmatic eyes that showed that eyes with larger pupil sizes tended to have a lower UCVA,8–10 indicating that pupil size plays an essential role in visual performance in astigmatic eyes as well as in non-astigmatic eyes. Especially in eyes with larger pupils, it may be necessary to correct the pre-existing astigmatism in order to acquire excellent visual outcomes. Our results have also revealed that UCVA was better in eyes with less astigmatism in both WTR and ATR astigmatic eyes. It is quite reasonable that it was in line with previous studies that eyes with a greater astigmatism had lower UCVA.11 12 We suggest that not only the amount of astigmatism but also pupil diameter may play an important role in determining UCVA, which is an important factor for minimising spectacle dependence and maximising subsequent patient satisfaction in astigmatic eyes. The human visual system is known to suffer from aberrations, diffraction, scatter, finite receptor size and noise in the neural pathways. The smaller pupil size may have some advantages in its superiority for image formation, such as an increasing depth of focus, a decrease in HOAs13 14 and a decrease in light scatter,15 all of which may, to some extent, offset the deleterious effects of reduced luminance16 and diffraction. Accordingly, the smaller pupil may moderate the impact of astigmatic defocus. It is not only the amount of astigmatism or the axis of astigmatism that should be taken into consideration for the surgical correction of cylindrical errors, but also the pupil diameter.
Interestingly, UCVA is highest not for 1 mm pupil but for 2 mm pupils in eyes with WTR and ATR astigmatism of 1 D, whereas UCVA is highest for 1 mm pupils in eyes with WTR and ATR astigmatism of 2 and 3 D. Atchison et al8 demonstrated that the maximum visual acuity occurred for 2–3 mm diameter pupils, but that larger pupils reduced acuity only marginally in non-astigmatic eyes. Strang et al13 reported that the contrast sensitivity function with a larger pupil was better than that with a smaller pupil at some spatial frequencies, owing to the complex interactions between pupil size and defocusing. The optical modulation transfer function of the human eye has been reported to be equivalent to that of the perfect diffraction system-limited system at a pupil diameter of 1 mm but not of 1.5 or 2 mm.14 15 17 18 Although the exact reason still remains unclear, the authors assume that the pupil-dependent effect of increasing depth of focus, and a decrease in HOAs and light scatter, on UCVA may be larger than the counteractive effect of diffraction and reduced luminance for a 1 mm pupil, not in eyes with low astigmatism, but in eyes with high astigmatism.
It has been shown that pupil size can be influenced not only by patient background, for example by age,19–25 manifest refraction26 and the accommodative state of the eye,27 28 and by various sensory and emotional conditions,29 but also by measurement conditions affecting the level of retinal illuminance.30 31 This measurement does not necessarily offer a high reproducibility. However, we used artificial pupils, which were not at all influenced by these factors, at the spectacle plane. The artificial pupils may be useful for determining the exact role of pupil size in visual performance in such eyes.32
There are several limitations to this study. First, we examined younger populations who often show WTR astigmatism in this study, and thus this study does not actually reflect the status of any population having some astigmatism. In addition, younger people frequently have a larger pupil,19–25 which contributes to larger HOAs and higher retinal luminance levels. Second, in the present study, we measured only HOAs for a 4 mm pupil, and did not investigate other factors that can affect visual performance in these astigmatic eyes. Since the level of HOAs appears to be low and almost equivalent in all eyes, as shown in the results, we assume that HOAs did not significantly influence the visual outcomes in this study. A further study is needed in order to clarify the exact role of HOAs and other factors on visual outcomes in eyes having cylindrical errors. Third, we measured only high-contrast visual acuity under photopic conditions (250 lux) with monocular vision, and so our measurements in this study do not accurately reflect natural binocular viewing conditions. However, these natural viewing conditions may include not only the photopic but also the mesopic conditions under which we assessed the pupil size. We are currently conducting a further study to assess pupil size under natural viewing conditions without occlusion.
In conclusion, our study revealed that not only the amount of astigmatism but also the pupil size can affect UCVA in WTR and ATR astigmatic eyes, suggesting that not only the amount of astigmatism but also pupil size should be taken into consideration in order to acquire better visual performance in eyes with astigmatism. Especially in eyes with larger pupils, it may be necessary to correct the pre-existing astigmatism to acquire excellent visual outcomes. We believe that these findings, although simple, are clinically important because most surgeons merely consider the amount of astigmatism and the axis of astigmatism for the surgical correction of astigmatism in a clinical setting. A further study with greater numbers of subjects is required to confirm these preliminary findings.
References
Footnotes
Competing interests None.
Patient consent Obtained.
Ethics approval Ethics approval was provided by the Local Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance