Article Text

Abstract
Background Age-related macular degeneration (AMD) is a degenerative process that leads to severe vision loss. Wet AMD is defined by choroidal neovascularisation, leading to the accumulation of subretinal fluid (SRF), macular oedema (ME), and pigment epithelium detachments (PED). Purpose To evaluate the initial clinical experience of conversion from bevacizumab or ranibizumab to aflibercept in wet AMD patients.
Methods Records of 250 consecutive wet AMD patients were retrospectively reviewed. Of 250 patients, 29 were naive (with no previous treatment), and 221 were previously treated with bevacizumab (1/3) or ranibizumab (2/3). On average, converted patients received 14 injections every 6 weeks on a treat-and-extend regimen with Avastin or Lucentis before being converted to aflibercept every 7 weeks on average (no loading dose) for three doses. For the purposes of this study, we concentrated on the patients converted to aflibercept since the number of naive patients was too small to draw any conclusion from. Snellen (as logMar) visual acuities, and optical coherence tomography (OCT) were compared predrug and postdrug conversion.
Results Converted patients did not show a significant difference in visual acuity or average OCT thickness from preconversion values; however, small improvements in ME (p=0.0001), SRF (p=0.0001), and PED (p=0.008) grading were noted on average after conversion to aflibercept.
Conclusions No significant difference in visual outcome or average OCT thickness was observed when switched from bevacizumab or ranibizumab q6 week to aflibercept 7-week dosing, on average. Mild anatomic improvements did occur in converted patients with regard to ME, SRF and PED improvement, on average, after conversion to aflibercept, and aflibercept was injected less frequently. No serious adverse reactions, including ocular infections or inflammation, as well as ocular and systemic effects were noted.
- Macula
- Pharmacology
- Retina
- Treatment Medical
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Age-related macular degeneration (AMD) is a chronic degenerative process that is the leading cause of severe vision loss in people over the age of 60 years in developed countries. Wet AMD is defined by the abnormal growth of blood vessels, choroidal neovascularisation (CNV), leading to accumulation of subretinal fluid (SRF), macular oedema (ME), and pigment epithelium detachments (PED). Ischaemia and the secondary upregulation of angiogenic factors are the main driving factors of CNV, eventually leading to severe vision loss. Vascular endothelial growth factor (VEGF) is a homodimeric glycoprotein that induces endothelial cell proliferation and migration. It is a main activator of angiogenesis and causes increased permeability and lymphangiogenesis.1–4
The mainstay of treatment for wet AMD has become intravitreal injections of anti-VEGF agents. The two most common anti-VEGF agents used today include ranibizumab (Lucentis, Genentech, South San Francisco, California), a recombinant antibody fragment that binds all active forms of VEGF A, and bevacizumab (Avastin, Genentech), a recombinant humanised full-length antibody that also binds all active isoforms of VEGF. Level 1 data has clearly illustrated that these two agents are beneficial in the treatment of wet AMD.5 ,6 Though considered to be ‘off-label,’ the use of bevacizumab for wet AMD has also been well established with a favourable adverse event profile. The Comparison of Age-Related Macular Degeneration Treatments Trial (CATT) reported that monthly injections of ranibizumab had slightly better visual acuity gain compared to bevacizumab injections, with a better serious adverse event profile.7
Newer agents have been investigated with hope for better efficacy, duration of effect and safety. Aflibercept (Eylea Regeneron, Tarrytown, New York, USA), VEGF Trap, is a fusion protein that aggregates VEGF-receptor 1, VEGF receptor 2 and IgG, and binds VEGF A, VEGF B and placental growth factor. It binds with a higher affinity and has a longer intravitreal half-life than ranibizumab and bevacizumab.8 ,9 With its longer half-life and higher affinity, studies have examined the possibility of patients needing fewer injections to achieve similar efficacy.8
Methods
Institutional review board approval was obtained from the North Shore-Long Island Jewish Health System, Manhasset, New York for this study. The medical records of 250 consecutive patients with wet age-related ME were reviewed. This was a retrospective, consecutive series of our initial clinical experience with patients’ initial three doses of aflibercept. Patients chosen for this study were an average of 83 years old; one-third of whom were male and two-thirds female. Patients’ records were analysed for age, gender, Snellen visual acuity, previous anti-VEGF treatment, if any, interval of treatment, and pretreatment and post-treatment visual acuities and optical coherence tomography (OCT) (tables 1⇓–3, respectively). Clinical findings were followed using Snellen visual acuity and OCT. ME, SRF and PED were graded on scales as follows: ME and SRF 0=none, 1=mild, 2=moderate, 3=marked, 4=severe; and, PED 0=none, 1=low, 2=moderate, 3=severe. Four authors in a blinded, masked fashion read the optical coherence topographies. An independent biostatistician analysed the data collected; Snellen visual acuity was converted to logMar for statistical purposes.
Demographics
Intravitreal agents used prior to conversion to aflibercept
Snellen visual acuity
Results
Of the 250 patients analysed, 29 patients (12%) had not been previously treated with anti-VEGF therapy, and 221 patients (88%) were previously treated with either intravitreal bevacizumab or ranibizumab injections. Since the number of naive patients is small and our experience with these patients was similar to the View 1 and 2 study results, we will not focus on the 29 patients in this naive group. Previously treated patients received an average total of 14 injections every 6 weeks, on a treat-and-extend regimen before being converted to aflibercept. The range for these injections was from every 4–8 weeks. Of the 221 previously treated patients, approximately one-third (76 patients) had been treated with bevacizumab and two-thirds (145 patients) with ranibizumab before conversion to aflibercept. The 221 patients previously treated with either bevacizumab or ranibizumab, received three doses of aflibercept after conversion at 7-week intervals, on average, based on results of no fluid or maximal anatomical response, without a loading dose for three doses. The range for these injections was every 4–9 weeks. The initial Snellen acuity of 199 of the 221 previously treated patients was equal to or better than 20/200. Twenty-two of the 221 previously treated patients had vision worse than 20/200 preconversion.
When comparing average visual acuities of all previously treated patients across visits as seen in figure 1, the average visual acuity of converted patients (red line) did not show significant improvement (p=0.06; n=221), a Snellen equivalent of approximately 20/63 (logMar 0.50). Converted patients with an initial visual acuity equal to or better than 20/200, (figure 1), also did not show a significant improvement, a Snellen equivalent of 20/48 (logMar 0.38) preconversion to 20/53 (logMar 0.42) postconversion (blue line) (p=0.08; n=199).
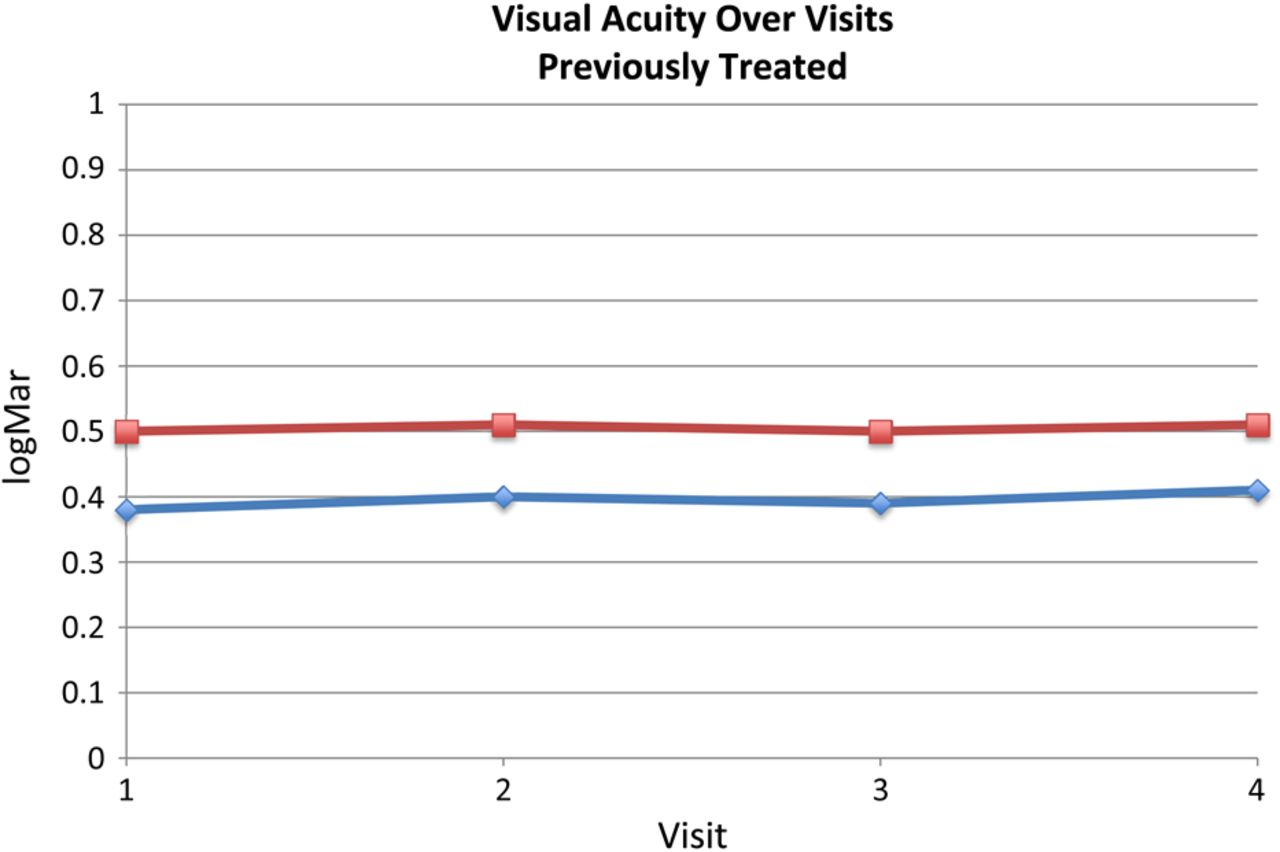
Visual acuity over visits. Overall change in logMAR visual acuities over visits in previously treated patients. The average overall visual acuity of converted patients (shown in red) did not show significant improvement after conversion to aflibercept (p=0.06; n=221). The converted patients with an initial visual acuity equal to or better than 20/200 (shown in blue) also did not show a significant improvement over time, on average, after drug conversion (p=0.08; n=199).
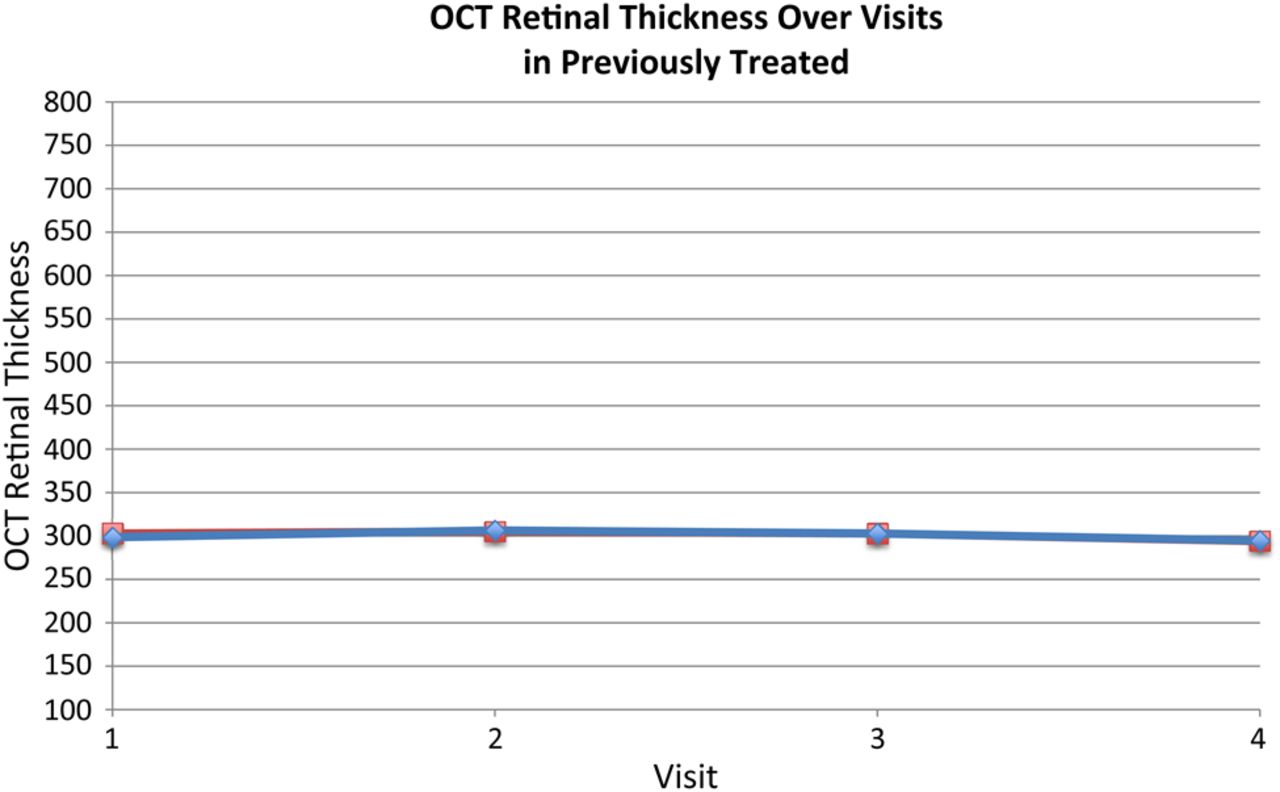
When comparing OCTs of all patients over time in figure 2, retinal thickness did not improve significantly for converted patients (red line), approximately 300 microns preconversion and postconversion (p=0.3). In the subgroup analysis of patients with an initial acuity of equal to or better than 20/200, similar results were seen (blue line) with an average of 295 microns predrug and postdrug conversion (p=0.07).

Optical coherence tomography (OCT) retinal thickness over visits. Change in overall retinal thickness measured by macular OCT over visits in previously treated patients. Retinal thickness did not improve significantly for those converted patients (shown in red), approximately 300 μ (p=0.3; n=221) preconversion and postconversion. Patients with an initial acuity equal to or better than 20/200 (shown in blue) also did not show a significant difference after conversion, an average of 295 microns preconversion and postdrug conversion (p=0.07; n=199).
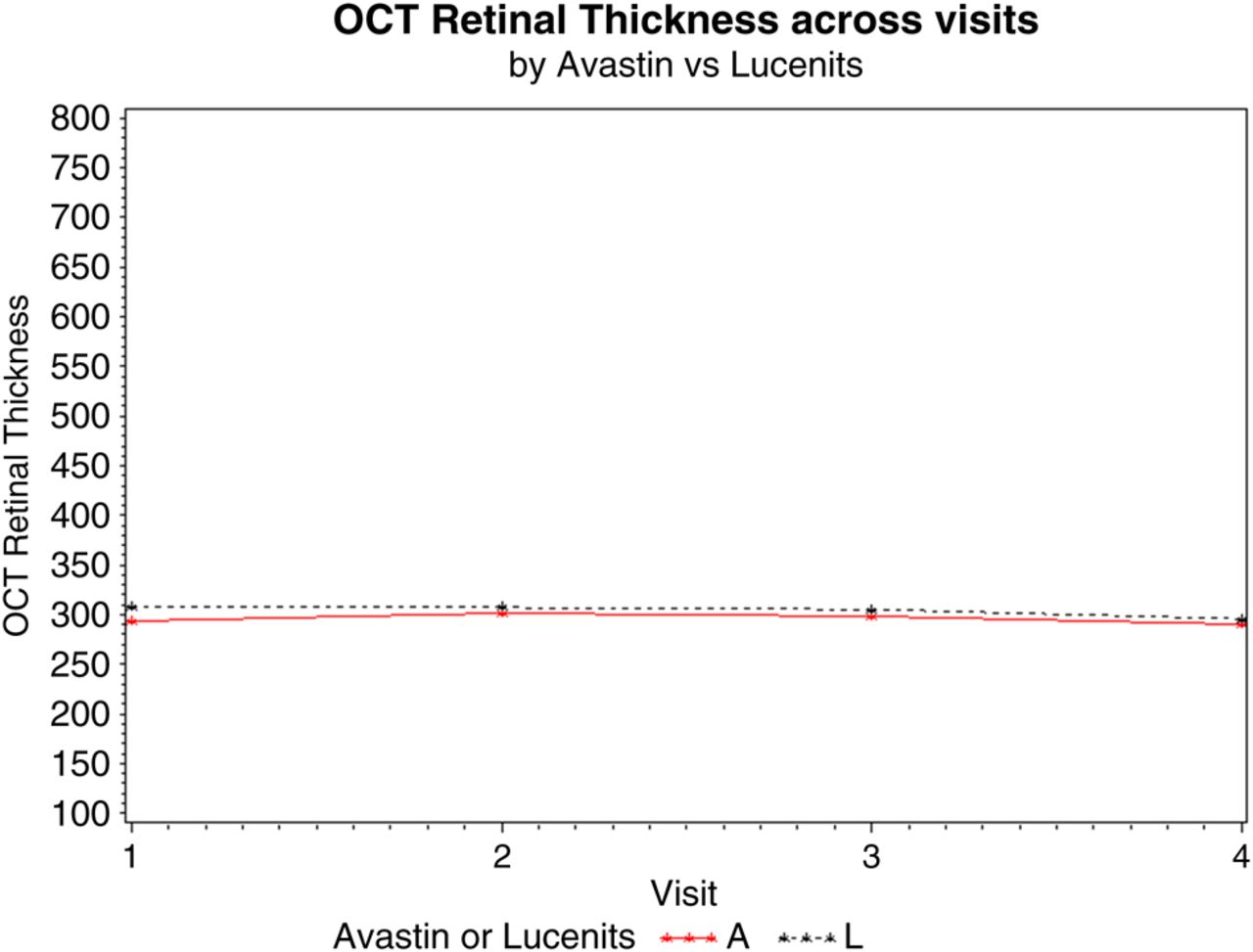
Visual acuity in patients treated with bevacizumab and ranibizumab were also analysed separately preconversion and postconversion. There was no significant change in patients converted from bevacizumab or Ranbizumab to aflibercept with regard to vision, as well as no significant changes in central foveal thickness in either group of patients after conversion (figures 3 and 4). Recal, that on average, ranibizumab and bevacizumab were injected every 6 weeks, whereas aflibercept was injected every 7 weeks.

Avastin/lucentis visual acuity of previously treated patients. Red line indicates change in previously treated Avastin patients (n=76), and black line indicates change in previously treated Lucentis patients (n=145) after being switched to aflibercept. Neither group has a significant p value for change in vision (p=NS).

Avastin/lucentis optical coherence tomography (OCT) central foveal thickness for previously treated patiets. OCT central foveal thickness for the Avastin group (n=76; red line), and Lucentis group (n=145; black line) after switch to aflibercept. The p value for both groups is not significant (p=NS).
ME and SRF accumulation were compared using a standard grading scale: 0 equivalent to none, 1 equivalent to mild, 2 equivalent to moderate, 3 equivalent to marked, and 4 equivalent to severe. ME decreased in the converted patients (figure 5) (grading of 0.42–0.18; p=0.0001). SRF, as seen in figure 6, significantly decreased in converted patients (grading of 0.73–0.36; p=0.0001). The dashed yellow line indicates the mean grading of subretinal fluid, where the solid lines indicate individual grades. The darker the individual grade lines, the more patients that had that particular change occur, and this is reflected in the average. PEDs were compared using a standard grading scale: 0 being none, 1 equivalent to low, 2 equivalent to medium and 3 equivalent to severe. In figure 7, converted patients displayed a significant decrease in PED size (0.73–0.62; p=0.008). As in the other subgroups, the dashed yellow line indicates the mean grading of PED size, where the solid lines indicate individual patient changes after drug conversion with the darker black lines indicating more patients represented in that change for better or worse over time after conversion.
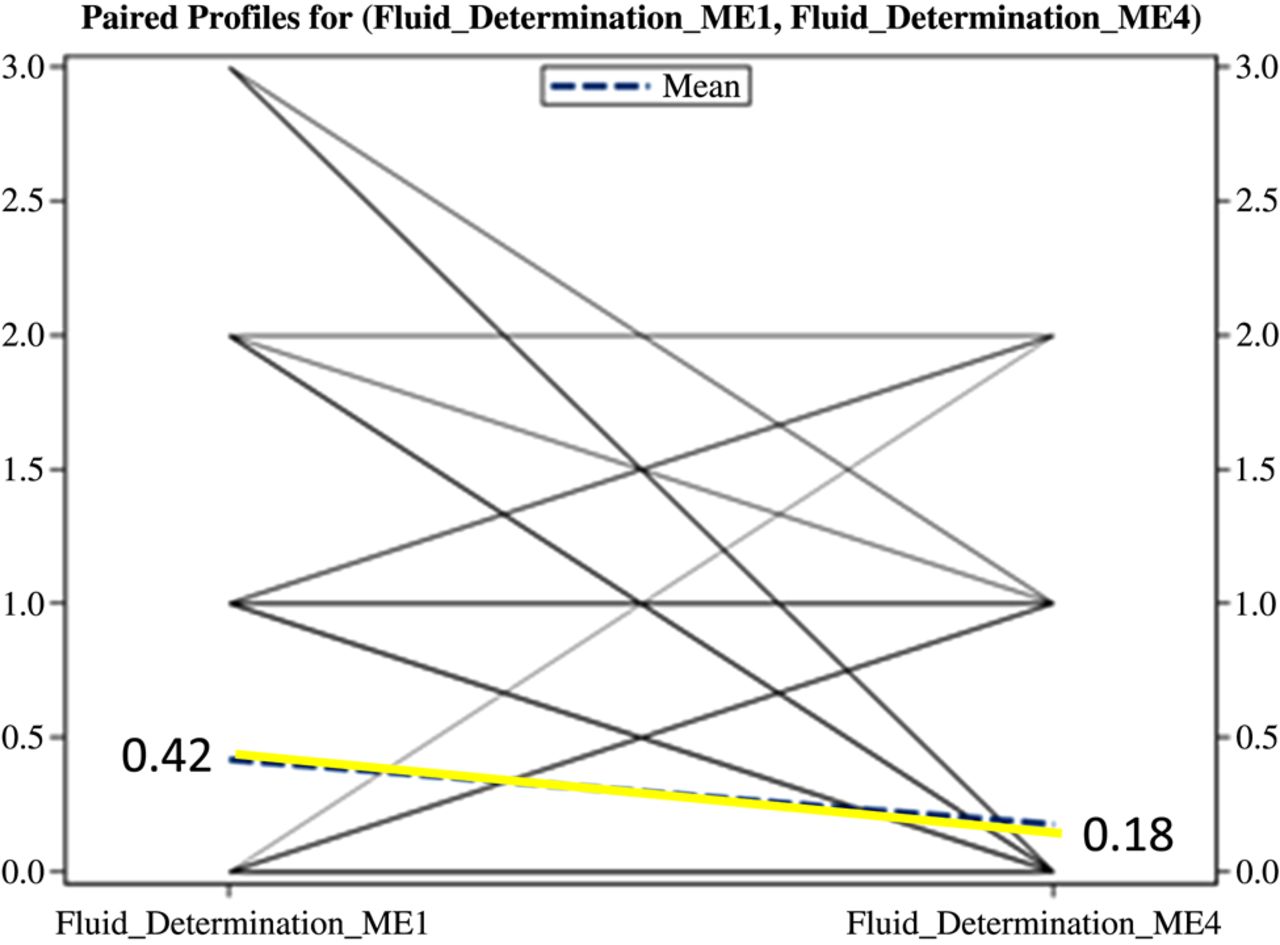
Grading of macular oedema (ME) in converted patients. The dashed yellow line indicates the mean grading of oedema, where the solid lines indicate individual grades. The darker the line, the more patients that are represented making that same change preconversion to postdrug conversion. ME accumulation compared using a standard grading scale: 0 equivalent to none, 1 equivalent to mild, 2 equivalent to moderate, 3 equivalent to marked, and 4 equivalent to severe. ME decreased significantly in the converted group (grading of 0.42–0.18) (p=0.0001).
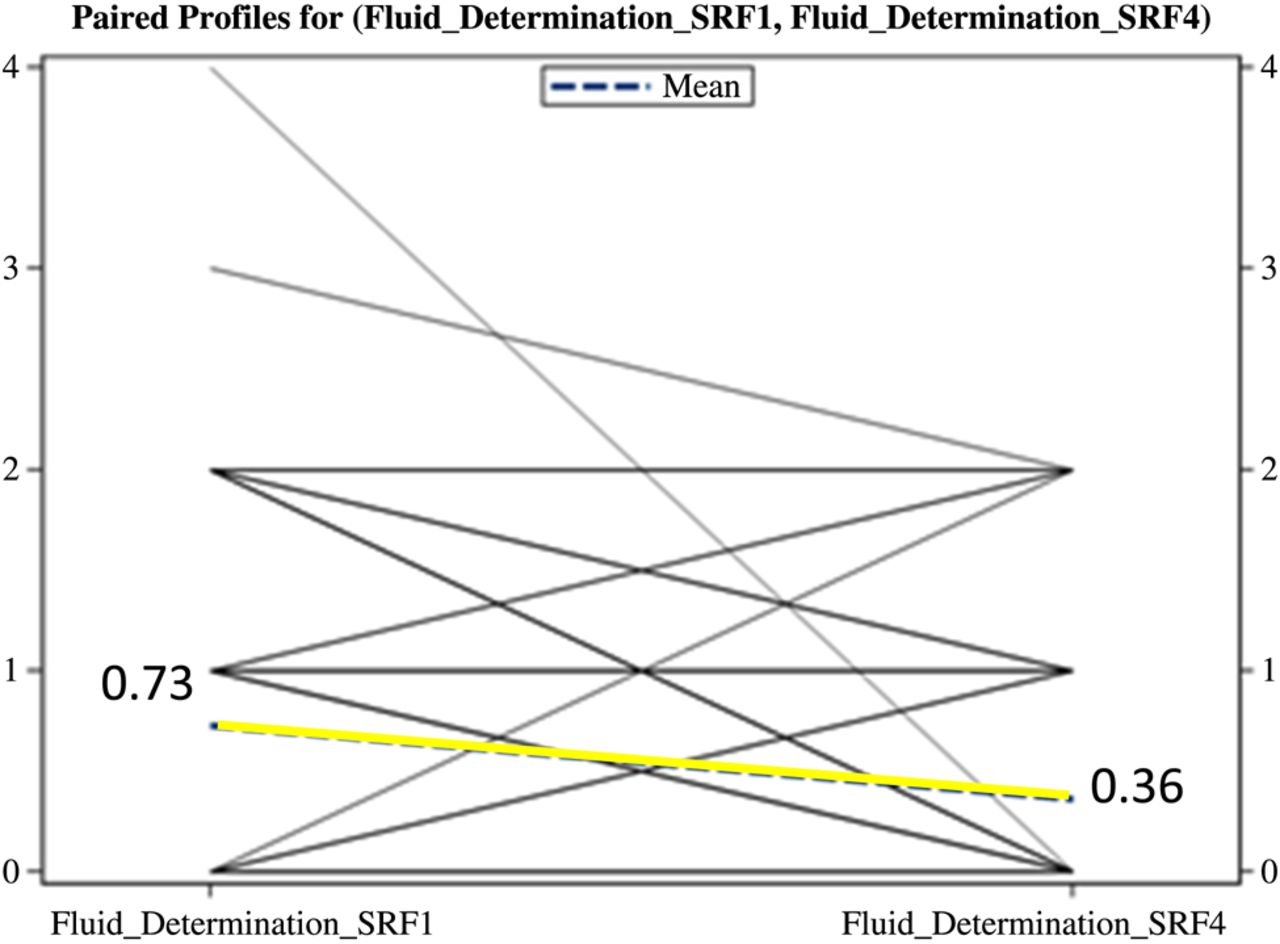
Grading of subretinal fluid (SRF) in converted patients. The dashed yellow line indicates the mean grading of oedema, where the solid lines indicate individual grades. The darker the line, the more patients that are represented making that same change preconversion to postdrug conversion. SRF accumulation was compared using a standard grading scale: 0 equivalent to none, 1 equivalent to mild, 2 equivalent to moderate, 3 equivalent to marked, and 4 equivalent to severe. SRF decreased in the converted group improved significantly, on average (0.73–0.36) (p=0.0001).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Grading of pigment epithelial detachments (PED) in converted patients. The dashed yellow line indicates the mean grading of PEDs, where the solid lines indicate individual grades. The darker the line the more patients that are represented making that same change preconversion to postdrug conversion. PEDs were compared using a standard grading scale: 0 being none, 1 equivalent to low, 2 equivalent to medium, and 3 equivalent to severe. Converted patients displayed an average decrease in the size of the PED (0.73–0.62) (p=0.008).
Overall in the converted group, 96 patients started with a vision of 20/40 or better, and 91 patients ended with a visual acuity of 20/40 or better (logMar 0.30), while 76 patients started and ended with a visual acuity of 20/40 or better out of the 221 converted patients. During the study, no drug or injection-related serious adverse events, such as endophthalmitis, inflammatory reactions, or systemic complications occurred.
Discussion
This was a retrospective, consecutive, case series of 250 consecutive patients with wet AMD, in which 29 patients were naive to treatment, and 221 were converted from ranibizumab or bevacizumab to treatment with intravitreal aflibercept. Our initial experience with aflibercept shows favourable outcomes overall. Visual acuity and OCT central foveal thickness in those patients converted to aflibercept did not show improvement. Grading of ME, SRF, and pigment epithelial detachment showed some improvement, on average, in converted patients, and this was statistically significant when reviewed by masked, independent graders. In the patients converted from ranibizumab and bevacizumab to aflibercept, 96 patients started with a vision of 20/40 or better, and 91 patients ended with a visual acuity of 20/40 or better (logMar 0.30), while 76 patients started and ended with a visual acuity of 20/40 or better out of the 221 converted patients. In summary, while no significant difference in visual outcome was observed in patients switched from bevacizumab or ranibizumab to aflibercept, mild anatomic improvements did occur, on average, after the switch to aflibercept, and the treatment interval increased from every 6 weeks, on average, before drug conversion, to every 7 weeks after conversion to aflibercept.
The CATT trial demonstrated that monthly injections of ranibizumab and bevacizumab had more favourable outcomes, compared to as-needed dosing, though this difference was small, on average.7 The VEGF Trap-Eye: Investigation of Efficacy and Safety in Wet AMD (Views 1 and 2) was a randomised, double-masked, multicentred, active-controlled trial that compared monthly and every other month intravitreal injections (after 3 monthly loading doses) of various doses of aflibercept to monthly injections of 0.5 mg of ranibizumab. Specifically, the doses of aflibercept and ranibizumab were: 0.5 mg aflibercept monthly, 2 mg aflibercept monthly, 2 mg aflibercept every other month after 3 monthly loading doses, and 0.5 mg ranibizumab monthly. Monthly, and every other month, intravitreal injections of 2 mg aflibercept were shown to have non-inferior results compared to monthly injections of ranibizumab in the first year. Additionally, monthly injections of 2 mg of aflibercept compared to monthly injections of 0.5 mg of ranibizumab showed a significant improvement in visual acuity (p<0.01) at 52 weeks. There was a favourable safety profile for aflibercept and ranibizumab. Views 1 and 2 illustrated that one of the benefits of aflibercept may include fewer injections compared to monthly ranibizumab.8 The effect of ranbizumab and aflibercept on ME has been shown to be equal, with favourable outcomes for both.10
Prior studies have examined the switch from other anti-VEGF drugs (ranbizumab or bevacizumab) to aflibercept. Cho et al studied 353 eyes with persistent SRF after ranbizumab and bevacizumab injections. Six months after switching to aflibercept, 89% of patients showed a significant decrease in central subfoveal thickness (295–274 microns) and 18% were completely dry on OCT. However, no visual improvement was seen at last follow-up 6 months after switching to aflibercept.11 There have been other studies on switching from ranbizumab or bevacizumab to aflibercept. In a study by Yonekawa et al,12 102 eyes were studied with 18 weeks follow-up where the authors found stabilised vision and anatomical improvement with a lengthened injection interval of 1–2 weeks, on average, after converting to aflibercept from Avastin or Lucentis. In another study by Bakall et al,13 36 eyes were converted, and after 3 monthly injections of aflibercept, 50% of eyes had an improvement in subretinal or intraretinal fluid (from three previous monthly injections of Avastin or Lucentis before conversion) while 42% remained stable, and 8% worsened after drug conversion to aflibercept. Vincent Ho and colleagues reported 96 eyes treated with 3 monthly injections of aflibercept followed by a fourth injection within 2 months. Eighty-five percent of patients remained visually stable, 7% gained two or more lines, and 7% lost two or more lines of visual acuity after drug conversion to aflibercept. Similar mixed results were seen on OCT after drug conversion in his study.14
In our study, ranibizumab and bevacizumab injected every 6 weeks compared to aflibercept injected every 7 weeks, did not show a significant change with regard to visual acuity or OCT central foveal thickness. On analysis of the individual OCTs, we saw mild anatomic improvements, on average, in patients after being converted to aflibercept. On average, in converted patients, as seen in figures 5⇑–7, there was a modest improvement in ME, SRF and PED. These anatomical improvements with respect to ME, SRF and PED were not seen in all patients, and as noted in some previous studies, some patients improved, some had no change, and some worsened, as seen in figures 5⇑–7 represented by the individual black lines in those graphs (which averaged out to the yellow line). Aflibercept proves to be an effective treatment for wet age-related macular degeneration with slightly fewer injections, on average, and anatomical benefits in some cases. The exact response that one will see to one anti-vegf drug versus another is not predictable, and this highlights the need to be able to use all the anti-vegf drugs as needed and judged to be potentially helpful by the treating physician to optimise the patient's visual and anatomical result, and ideally decrease the treatment burden for the patient.
This study included 250 subjects of which we focused on the 221 converted patients. Limitations of this study include its retrospective nature, limited sample size, visual acuity recorded in Snellen format, no predetermined protocol, and limited follow-up period, as well as the fact that these patients were treated with a treat-and-extend protocol that may have induced some bias. Additionally, most of these patients were converted due to a physician perception that there was a limited degree of effect, or duration of effect, from their previous therapy (Avastin or Lucentis). Although adverse events were carefully noted, there is always a possibility that some systemic effect may not have been captured in this retrospective study.
Footnotes
-
Contributors PJF, DF, KG, and VD designed data collection tools, monitored data collection, and analysed the data. PJF is the principle guarantor. PJF aided in the statistical analysis plan as well. PJF and FA analysed the data, drafted, and revised the paper. JN and KC aided in revising the paper.
-
Funding This work was supported by Regeneron and Genentech.
-
Competing interests None.
-
Ethics approval North Shore Long Island Jewish IRB.
-
Provenance and peer review Commissioned; externally peer reviewed.