Article Text

Abstract
Purpose The introduction of intra-arterial chemotherapy (IAC) as salvage treatment has improved the prognosis for eye conservation in group D retinoblastoma. The aim of this study was to compare the outcomes of consecutive patients with advanced unilateral disease treated with either first-line intravenous chemotherapy (IVC) or first-line IAC.
Design This is a retrospective mono-centric comparative review of consecutive patients.
Patients Sporadic unilateral retinoblastoma group D cases treated conservatively at Jules-Gonin Eye Hospital and CHUV between 1997 and 2014. From January 1997 to August 2008, IVC, combined with focal treatments, was the primary treatment approach. From September 2008 to October 2014, IAC replaced IVC as first-line therapy.
Methods 48 patients met the inclusion criteria, receiving only either IAC or IVC as primary treatment modality.
Results Outcomes of 23 patients treated by IVC were compared with those of 25 treated by IAC; mean follow-up was 105.3 months (range 29.2–218.6) and 41.7 months (range 19.6–89.5), respectively. Treatment duration was significantly shorter in the IAC group (p<0.001). Ten eyes in the IVC group underwent enucleation. Recordable visual acuity of the salvaged eyes was significantly better in the IAC group (0.9 vs 1.4 logarithm of the minimum angle of resolution, p<0.01). No extraocular disease, metastases or long-term systemic complications were observed in either group.
Conclusions The difference in the time frame between treatment groups had an impact on the availability of intravitreal chemotherapy treatment. Despite this, the results reported here imply that eyes treated with first-line IAC will have shorter treatment period, better ocular survival and visual acuity than first-line IVC.
- Retina
- Treatment Medical
- Child health (paediatrics)
- Neoplasia
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Over the past two decades, first-line conservative management of advanced bilateral retinoblastoma (IIRB1 group D) has moved from external beam radiotherapy (EBR) to intravenous chemotherapy (IVC), consolidated by focal treatments (FTs). Globe salvage in bilateral group D retinoblastoma (Rb) at 5 years was 47% with six cycles of IVC alone; this can be increased to 68% when combined with low-dose (36 Gy) intensity-modulated radiation therapy in cases of relapse.2 ,3 Reported functional outcome is poor, especially when the macula is involved.4–10 Due to the low salvage rate and poor visual outcome after IVC, enucleation historically remained the treatment of choice in many cases of unilateral group D Rb.2 ,11–14
Intra-arterial chemotherapy (IAC) has emerged as an alternative to enucleation or EBR in eyes with tumour recurrence or drug resistance following IVC.11 ,15–22 Schaiquevich et al23 showed significantly higher salvage rates with IAC than sequential periocular topotecan and a second course of IVC in eyes with failed first-line IVC. Despite discrepancies in classification, several studies on first-line and salvage IAC for group D Rb have reported high globe retention rates.15 ,18 ,24–26 In a survey by Grigorovski et al27 comprising 31 treatment centres, IAC was reported as first-line treatment by the majority (74%) for unilateral advanced disease. To date, visual outcomes with first-line IVC are poor, especially when there is macular involvement.5
To the best of our knowledge, there has been no prospective study completed comparing IAC with IVC as first-line treatment for group D Rb.28 This study is a retrospective systematic review of consecutive patients with sporadic unilateral group D Rb treated at the Jules-Gonin Eye Hospital by either first-line IAC or IVC to estimate eye retention rates, visual prognosis and systemic or ocular adverse occurrence rates.
Methods
Patients
This retrospective study was approved by the ethical committee of Vaud, Switzerland (authorisation # 2016-00149), and compliant with the Declaration of Helsinki. All consecutive patients with sporadic unilateral retinoblastoma treated conservatively between 1997 and 2014 at Jules-Gonin Eye Hospital and the CHUV were included. Exclusion criteria were other primary treatments undertaken (including IAC/IVC started at a different treatment centre), patients receiving both IVC and IAC during the course of treatment, consultation for second opinion only and cases with bilateral disease. Diagnosis was based on ophthalmological examination under general anaesthesia, with RetCam images and ultrasound recorded by the same ocular oncologist (FLM). Eyes were grouped according to the International Intraocular Retinoblastoma Classification (IIRC) classification1 (patients prior to 2005 reclassified from Reese-Ellsworth).29 During the study period, 231 consecutive patients were referred for unilateral Rb, of which 148 met the inclusion criteria, including 120 with advanced disease, that is, 75 group D and 45 group E. All but one of group E eyes underwent primary enucleation (97.8%) and in group D 22 were enucleated (29.3%) (20 of 36 cases prior to 2008 (56%) and 2 of 39 cases since 2008 (5%)).
Fifty-three patients with group D and one group E were treated conservatively with IVC and/or IAC. Five patients were treated with combination IAC/IVC (including the group E eye) and one did not comply with the treatment protocol, resulting in 48 records for analysis. Informed consent was obtained (MB-P). A cerebral MRI was performed to exclude trilateral Rb or extraocular extension. If the optic nerve head was not fully visible or was in contact with the tumour, a spinal tap was obtained to exclude central nervous system extension. Prior to IVC, a complete blood cell count, renal (plasma creatinine and urea) and hepatic (aspartate-aminotransferase, alanine-aminotransferase and bilirubin) assessment, and auditive evoked potentials were systematically recorded. From January 1997 to August 2008, IVC, combined with FTs, was the primary treatment approach. From September 2008 to October 2014, IAC replaced IVC as first-line therapy except in children weighing <6 kg or after IAC unsuccessful procedure attempt.
Intravenous chemotherapy
IVC was given over 3 days, every three weeks or at an absolute neutrophil count of ≥1000×106/L and thrombocyte count of ≥100 000×106/L after the nadir, as follows: etoposide 150 mg/m2/day diluted in 125–250 mL NaCl 0.9% intravenously over 1 hour and with carboplatin 200 mg/m2/day diluted in 125–250 mL glucose 5% intravenously over 1 hour, both on days 1–3. In children under 1 year of age or weighing <10 kg, the dosage was adapted to weight (5 mg/kg/day for etoposide and 6.7 mg/kg/day for carboplatin). Chemotherapy was initiated within 24–48 hours after the ophthalmological examination.30 Chemotherapy was stopped as soon as it was possible to treat the tumour(s) with FT alone (cryotherapy, photocoagulation, thermotherapy, chemothermotherapy and brachytherapy) or continued up to a maximum of five.
Intra-arterial chemotherapy
IAC was performed on an outpatient basis (1 day) under general anaesthesia with systemic intravenous heparinisation (25–70 IU/kg). A 3 or 4 French introducer sheath was placed in the common femoral artery using the Seldinger technique. The internal carotid artery was then accessed with a guiding catheter over a 0.018-inch guide wire under fluoroscopic guidance. A heparinised saline flush was connected to the guiding catheter during the entire procedure. After a baseline cerebral angiogram, a 1.2 or 1.5 French microcatheter (Baltacci or Magic, Balt Extrusion, Montmorency, France) mounted on a 0.007-inch microguide wire (Hybrid, Balt Extrusion, Montmorency, France) was navigated to the ostium of the ophthalmic artery. After fluoroscopic confirmation of the correct positioning of the microcatheter tip, and the absence of contrast reflux in the internal carotid artery, a melphalan dose prepared according to weight (range 2.8–7.5 mg adjusted to 30 mL) was infused over 30 min (1 mL/min) according to the pulsatile injection technique.16 A final cerebral angiogram was obtained to exclude any thromboembolic events before removing the endovascular material. Chemotherapy was stopped as soon as it was possible to treat the tumour(s) with FT alone or continued up to a maximum of three.
Consolidation/salvage
Prior to each chemotherapy cycle, the necessity to continue IVC or IAC was determined based on the amenability to consolidation treatments or FT. For lesions not flat or calcified, sequential intensive FT was performed.31 In 2008, intravitreal melphalan was added to the FT armamentarium for persistent or recurrent vitreous disease.32 Tumour control was achieved and classified according to complete regression of retinal tumour type 0–433 and vitreous type 0–3.34 After first-line and consolidation therapies, an observation period was initiated. In cases of relapse that were possible to treat with salvage therapy, then all treatment modalities were considered except IVC and EBR.
Patient follow-up
After completion of IVC or IAC, amblyopia therapy was initiated, with the patching regimen adapted to age, collaboration and success. At last control visual acuity was recorded: indication of the presence/absence of light perception or best corrected visual acuity (BCVA) recorded as follows depending on age: Teller cards (<30 months); Lea symbols (Good-light Inc, Elgin, Il, USA) (30 months to 4 years); Snellen ‘E’ chart (4–5 years) and Snellen chart (>6 years). Visual acuities were converted to logarithm of the minimum angle of resolution (logMAR) values.35 Hand-held spectral-domain optical coherence tomography recordings using the Bioptigen imaging system (Durham, North Carolina, USA) were made in all salvaged eyes to classify foveal structure into three categories: fovea, intact damaged or absent.
Statistical analysis
Time to treatment completion and eye retention probability were analysed using the Kaplan-Meier method and compared between the IAC and IVC groups using the log-rank test statistic at a 5% level of significance using the ‘survival’ R package.36 Time to treatment completion was defined by treatment start date until tumour treatment was complete; data were censored at the last visit or at the date of enucleation. Statistical analysis was performed with the R software package V.2.15.1.37
Results
In total, 23 patients treated with first-line IVC, including two cases where IAC was first attempted but failed due to anatomical factors, were compared with 25 cases with first-line IAC. Two cases of IAC required micro-catheterisation and chemotherapy injection via the external carotid artery due to anatomical variants of the ophthalmic artery. Mean follow-up for the IVC group was 105.3 months (range 29.2–218.6) and for the IAC group 41.7 months (range 19.6–89.5).
Duration of treatment to resolution or enucleation
All patients completed first-line treatment, and the mean number of cycles (IVC) or injections (IAC) was comparable between groups (table 1). Tumour control was significantly faster in the IAC group (table 1 and figure 1). The number of consolidation treatments was comparable for both groups, with the IVC group receiving primarily chemothermotherapy as second-line treatment and the IAC group benefitting from intravitreal chemotherapy (IViC). All but one IVC eye (95.6%) required consolidation therapy compared with 80% (n=20) in the IAC group. In addition, relapse was observed at least once in 52% (n=12) of IVC vs 24% (n=6) of IAC eyes; IVC eyes had significantly more relapse (3.3 vs 1.3) and first relapse happened later than in IAC eyes (mean 6.3 vs 8.5 months) (table 1). The number of anaesthetics required to achieve tumour control in retained eyes was significantly higher in the IVC group with a mean number of 18 (range 5–38) compared with 9 (range 3–23) for IAC (p<0.001). The event-free interval in retained eyes of the IVC group up to last follow-up shows a mean 78.5 months (range 4.7–203.4) and that of the IAC group a mean 28.2 months (range 3.5–67.9).
Baseline characteristics and consolidation/salvage treatment after first-line intra-arterial or intravenous chemotherapy

Kaplan-Meier curves showing the time to treatment success for the intra-arterial chemotherapy (IAC) and intravenous chemotherapy (IVC). The log-rank statistic indicates that there is a significant difference between the curves p<0.001.
In order to examine data that were independent of IViC treatments, a subgroup analysis was performed. In the IVC subgroup, those eyes with diffuse vitreous seeding were excluded (ie, those that would have been potentially treated with IViC, n=16), and only eyes without IViC consolidation treatment treatment were included in the IAC subgroup (n=13; this included five eyes with diffuse vitreous seeding). Due to the inclusion criteria of both groups, the IAC is expected to do worse; however, in this subgroup analysis, we observed a higher rate of relapse (63%), 10/16 vs (29%) 3/13, p=0.06, in the IVC subgroup; also the mean number of anaesthetics was higher (19.2 vs 7.5, p<0.001) in the IVC subgroup.
Globe survival and final foveal structure
We observed that there was change in the primary enucleation rate in unilateral retinoblastoma between 1997 and 2008 from 56% (n/N=20/36) to 5% since the introduction of IAC in 2008 (2/39). Prior to 2008, eyes were often enucleated due to massive seeding (16 of the 20 cases) since 2008 no case of unilateral retinoblastoma group D has been enucleated due to seeding. The two enucleations were due to suspicion of optic nerve involvement. Histological risk factors were not observed in any of the cases of primary enucleation. This can be observed partially in the number of eyes with diffuse vitreous seeding observed at presentation, 72% in IAC vs 30% in IVC. None of the IAC group required enucleation (figure 2). In the IVC group, 10 eyes were enucleated after an average 16.5 months of treatment (range 0.8–48.4 months), 9 due to uncontrollable seeding and/or total retinal detachment (RD) and 1 due to phthisis bulbi. Excluding those eyes without diffuse vitreous seeding in the IVC group (n=16), five eyes underwent subsequent enucleation.
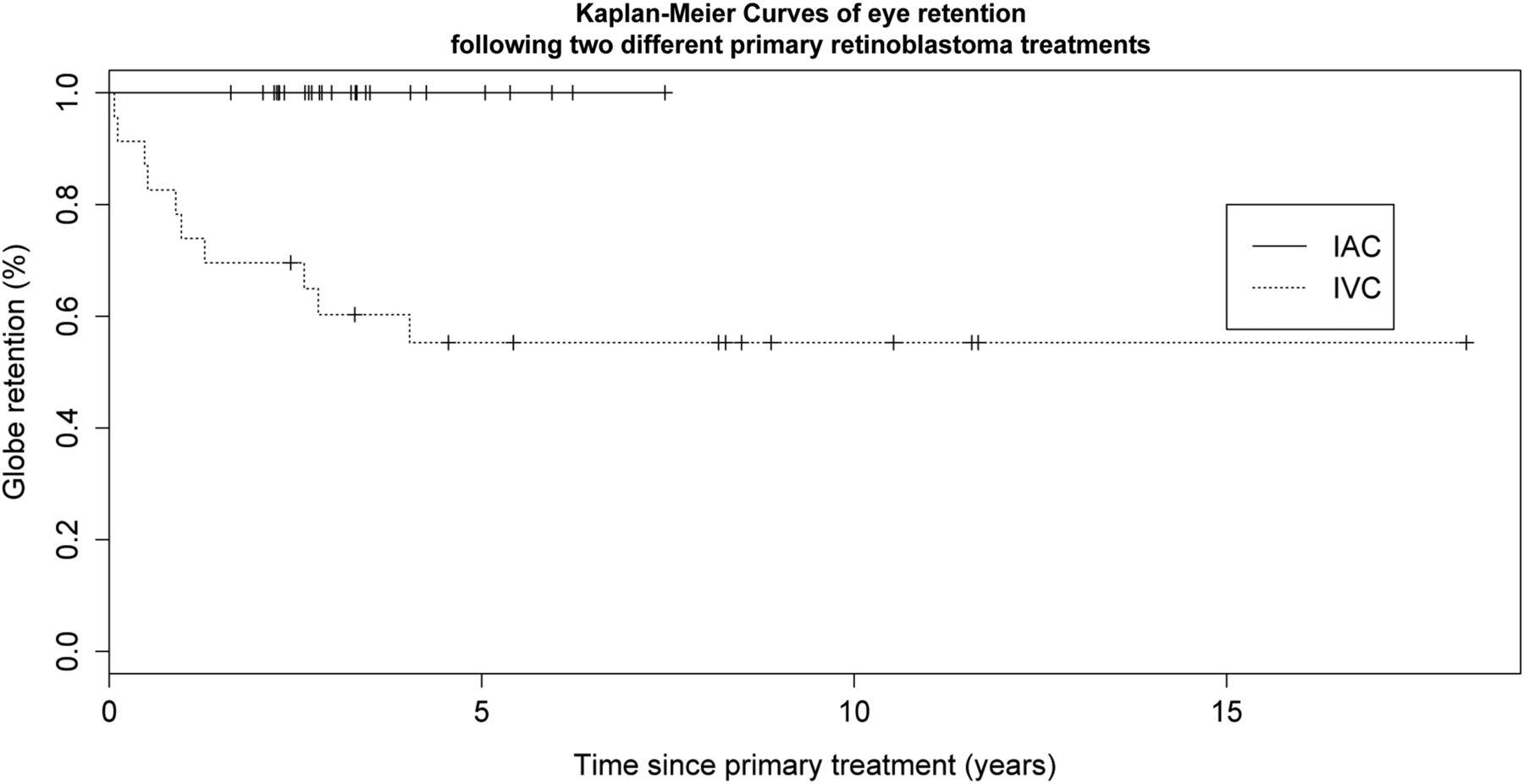
Kaplan-Meier curves showing the eye retention rates with respect to time for the intra-arterial chemotherapy (IAC) and intravenous chemotherapy (IVC). The log-rank statistic indicates that there is a significant difference between the curves p<0.001.
Review of the 10 cases enucleated showed that at presentation the macula was damaged/absent in 3 cases (30%) and intact in 7 cases (70%). OCT recordings taken at treatment completion for the IVC 13 salvaged eyes showed the fovea to be damaged in 6 cases (46%), absent in 7 (54%); none was intact. In the IAC group, OCT findings at treatment completion revealed the fovea to be damaged in 14 (56%), absent in 4 (16%) and intact in 7 eyes (28%).
Functional outcomes
Amblyopia therapy was carried out in the majority of retained eyes in both groups: IVC 11/13 (85%) and IAC 21/25 (84%). Irrespective of macula status, daily patching of the healthy eye (hours per day dependent on age and collaboration) was initiated in all cases except one where no treatment was necessary (ie, normal visual acuity).
In two cases in the IVC group and four of the IAC group patching was discontinued due to poor visual prognosis and/or lack of collaboration. Final visual acuity was significantly better in the IAC-treated eye (figure 3). In the IVC group, 1 of the 13 retained eyes had no detectable light perception. In the other 12 eyes, median visual acuity at last visit was 1.4 logMAR (IQR 1.2–3). Median visual acuity in contralateral eyes was 0.0 logMAR (IQR 0.0–0.0). In the IAC group, 22/25 eyes had light perception or better, and median visual acuity at last visit was 0.9 logMAR (IQR 0.3–1.2). Median visual acuity in contralateral eyes was 0.0 logMAR (IQR 0.0–0.0). The number of lines lost in comparison to the contralateral eye is given in figure 3, with a median of 6 lines (IQR 3–12) lost in the IAC group and 14 lines (IQR 12–31) lost in the IVC group (p=0.01).

{kind=link}
{kind=link}
{kind=link}
A bar chart summarising the number of lines lost in treated eye in comparison to contralateral healthy eye for intra-arterial chemotherapy (IAC) (black) and intravenous chemotherapy (IVC) (grey) treated eyes.
Complications
Details of systemic and/or ocular complications are given in table 2. There was no stroke, seizure, neurological impairment, hearing loss, limb ischaemia, second non-ocular primaries, metastasis or death in either cohort. There were significantly fewer, and less severe, systemic complications observed in the IAC group. Eight patients in the IVC group required transfusions versus none in the IAC group. Transient cardiorespiratory disturbances were observed intraoperatively in four patients in the IAC group but with no consequences. Following one successful injection of IAC, spasticity of the internal carotid artery in one patient resulted in the procedure being stopped during the second injection. Two patients in the IVC group were initially prescribed IAC, but the procedure was abandoned in favour of IVC due to anatomical restrictions inhibiting treatment.
Complications
In the ocular complications, secondary RD was observed in a similar number of patients in both groups. A greater number of IVC eyes receiving brachytherapy led to radiation-induced retinopathy (four eyes). In the IAC group, occlusive choroidopathy was observed in three eyes but with macula sparing and good visual acuity in one case. Melphalan-related retinopathy was noted in three cases with grades 1–3 related to IViC therapy.34
Discussion
To the best of our knowledge, this study is the second direct comparison between IAC and IVC in unilateral group D retinoblastoma as first-line treatment. Although between the two groups there are differences in the consolidation treatments used, the globe retention was 100% when IAC was the first-line therapy compared with 57% in the IVC group. No metastases or deaths occurred in either group. IAC was associated with fewer side effects, faster and more extensive response rates, fewer relapses and better visual acuity than the IVC-retained eyes. During the study period for unilateral group D retinoblastoma, primary enucleation dropped from 56% to 5% after the introduction of IAC and IViC in 2008. Moreover, in eyes that were independent of IViC treatment (cf subgroup analysis), relapses occurred more often in the IVC group.
Historically, IVC has been associated with poor eye retention rates, with 25–47% of eyes preserved in Rb group D eyes.2 In the present study, the eye retention rate was 57% at 5 years, notably with three courses of IVC compared with the 6–9 monthly cycles for group D eyes administered by the majority of treatment centres.1 In the recent publication by Shields et al comparing directly IVC and IAC in retinoblastoma, in the advanced treated eye (ie group D using the Philadelphia classification), similar numbers of eyes were examined. Although survival analysis was not performed and thus the rates cannot be directly compared, lower globe survival rates of 48% in IVC and 91% in IAC-treated eyes were reported. In our IAC cohort, we report a 100% eye retention rate with mean follow-up of 41 months, comparing favourably with the retention rates (82–100%) reported in the literature with a notably shorter mean follow-up (12–24 months).25 ,26 The higher retention rate reported here may be related to the more intensive FT protocol implemented at our centre and the early introduction of IViC treatments.
Tumour control was achieved sooner with IAC and with fewer relapses. Diffuse vitreous seeding was more frequent at presentation in the IAC group, but while these patients benefitted from consolidation and/or salvage IViC, this was a factor for enucleation in the IVC group. However, of the six cases in the IVC that relapsed and were subsequently enucleated, only three had vitreous seeding. The principal secondary complication in both cohorts was RD (table 2). In the IAC group, RD surgery without drainage was carried out in eight cases with successful reapplication; for the IVC group, this would also have been considered a contributing factor for enucleation. On closer review of the IVC cases that resulted in enucleation, if available at the time then a combination of intra-arterial (n=4) and/or intravitreal (n=3) chemotherapy and/or concomitant RD surgery (n=5) would have been proposed in 9 of the 10 cases. The remaining case, with evolution to phthisis bulbi despite complete tumour control, would still be enucleated.
To date, while electroretinogram alterations have been reported,38 the visual outcomes following globe salvage in unilateral retinoblastoma have rarely been reported in the literature.4–10 ,39 In the majority of cases, successfully treated eyes with preserved vision are amblyopic, but the results of the present study indicate that this can be successfully overcome and useful vision retained in a large proportion of eyes. In the IAC group, significantly better visual acuity was obtained; this may be due to the quicker time to resolution that allowed amblyopia therapy to begin sooner. While 7 of the 10 enucleated eyes in the IVC group were free of macular involvement at presentation, total RD was recorded in 6/7 of these eyes during follow-up, indicative of lower visual potential. Irrespective of whether these eyes could have been retained and reasonable VA achieved, figure 3 indicates that this would be insufficient to reverse the trend of better visual acuity afforded by IAC.
Theoretically, there is only a prophylactic benefit against metastases with IVC, but this cohort is inadequately powered to indicate superiority in terms of the systemic control between the two treatment types. On the other hand, a recent study pooling the data from four centres (n=634) demonstrated that there was no increase in mortality with IAC.40 On histopathological examination, none of the enucleated eyes showed risk factors, negating the need for adjuvant IVC. Despite these encouraging results, there is a perceived increased metastatic risk associated with IAC in advanced retinoblastoma.20 This fear originates from the increased histopathological risk factors observed in group D (17%) eyes following primary enucleation.41–43 In the case of neoadjuvant chemotherapy, these risks would either pass unnoticed if the eye is retained or be masked if secondary enucleation was finally performed.44 If left untreated, the presence of higher histopathological risk factors is expected to cause a 3% incidence of metastatic relapse, which can be reduced to 0.8% with adjuvant treatment in group D eyes.42 ,43 Preventive systemic chemotherapy in the presence of histopathological risk factors remains controversial as it exposes a large proportion of patients unnecessarily to additional risks.40 In the future, high-resolution MRI may play a role in determining which eyes require adjuvant therapy by documenting the presence or absence of radiological risk factors for minimally disseminated disease, such as invasion of the choroid or the retrolaminar portion of the optic nerve.45 Along the same lines, Torbidoni et al46 recently described the infraclinical detection of micro-metastasis using a cone-rod homeobox containing gene-dependent assay, which could be combined with the molecular detection of GD2 synthase mRNA in the cerebrospinal fluid.47
Some intraoperative haemodynamic respiratory disturbances were observed with IAC but all were transient. Episodes of neutropenia observed with IVC were more severe than with IAC, but none was life-threatening. With IAC, fewer general anaesthetics and shorter hospital stays were required, which indicates large improvements in cost efficiency for health providers. While IVC is available and widely decentralised, chemotherapy delivery via the ophthalmic artery route requires skills that only the most experienced interventional neuropediatric radiologists will possess. Therefore, IAC is only achievable with a sufficient number of patients within a centralised secondary or tertiary referral centre. However, we believe that the gains would more than justify investment required to remodel the shared care networks in order to allow the widespread implementation of this treatment modality.
The retrospective nature and the differences in adjunct treatment modalities available at the time of treatment undermine this comparison between groups. The introduction of IAC in 2008 as salvage treatment for group D disease had not been an option for the majority of the IVC group. We therefore excluded any subsequent cases combining IVC and IAC in order to compare the performance as primary options. There was a significant difference between cohorts at baseline in terms of age; however, this is likely an artefact of the minimum age limit for IAC treatment. Furthermore, the advent of IViC has provided an efficient FT for vitreous seeding that was not available as second-line or salvage treatment for most of the IVC group and is an unavoidable source of bias. To examine this possible source of bias, we performed subgroup analysis of eyes with vitreous seeding in the IVC group and without IViC treatment in the IAC group, and we observed that the primary outcomes were similar.
At present, IVC remains a valuable treatment option in bilateral disease, children too young for IAC or in the rare cases of failure of IAC due to anatomical factors. While more evidence is required, the significant advantages of IAC in terms of local disease control, eye retention, visual function prognosis, time to resolution, reduction in number of relapses and fewer retreatments required indicate that, when available and provided additional risk factors can be reliably identified, IAC is the treatment of choice in group D unilateral disease.
Acknowledgments
The authors thank Nicolas Milliet, Jules-Gonin Eye Hospital, and Pierre Flubacher, Department of Anesthesiology, Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland, for their contribution to this work.
References
Footnotes
Contributors FLM made substantial contributions to the conception and design of the work, the acquisition and interpretation of data. He contributed to revising the article critically for important intellectual content and gave final approval of the version published. He agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. CB made substantial contributions to the analysis and interpretation of data. She drafted and revised the article critically for important intellectual content and gave final approval of the version published. She agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. SH and MB-P made substantial contributions to the acquisition of data. Both drafted and revised the article critically for important intellectual content and gave final approval of the version published. Both agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. M-CG, CS, FP and PM made substantial contributions to the acquisition of data. They revised the article critically for important intellectual content and gave final approval of the version published. They agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Competing interests None declared.
Ethics approval Ethical committee of Vaud.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance