Article Text

Abstract
Aim To assess the safety and efficacy of microinterventional endocapsular nuclear fragmentation in moderate to severe cataracts.
Methods This was a prospective single-masked multisurgeon interventional randomised controlled trial (ClinicalTrials.gov NCT02843594) where 101 eyes of 101 subjects with grade 3‒4+ nuclear cataracts were randomised to torsional phacoemulsification alone (controls) or torsional phacoemulsification with adjunctive endocapsular nuclear fragmentation using a manual microinterventional nitinol filament loop device (miLOOP group). Outcome measures were phacoemulsification efficiency as measured by ultrasound energy (cumulative dispersed energy (CDE) units) and fluidics requirements (total irrigation fluid used) as well as incidence of intraoperative and postoperative complications.
Results Only high-grade advanced cataracts were enrolled with more than 85% of eyes with baseline best corrected visual acuity (BCVA) of 20/200 or worse in either group. Mean CDE was 53% higher in controls (32.8±24.9 vs 21.4±13.1 with miLOOP assistance) (p=0.004). Endothelial cell loss after surgery was low and similar between groups (7‒8%, p=0.561) One-month BCVA averaged 20/27 Snellen in miLOOP eyes and 20/24 in controls. No direct complications were caused by the miLOOP. In two cases, capsular tears occurred during IOL implantation and in all remaining cases during phacoemulsification, with none occurring during the miLOOP nucleus disassembly part of the procedure.
Conclusions Microinterventional endocapsular fragmentation with the manual, disposable miLOOP device achieved consistent, ultrasound-free, full-thickness nucleus disassembly and significantly improved overall phaco efficiency in advanced cataracts.
Trial registration number NCT02843594
- Treatment Surgery
- Optics and Refraction
- Lens and zonules
- Pathology
- Clinical Trial
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
Introduction
Endocapsular nuclear disassembly is an integral component of modern phacoemulsification. Fragmenting the nucleus permits extraction through a smaller corneal incision and a well-circumscribed curvilinear capsulorhexis. Nuclear fragmentation also reduces the likelihood of intraoperative posterior capsule rupture (PCR) because most nuclear emulsification occurs in the pupillary or supracapsular plane, a safe distance from the posterior capsule. To segment the nucleus, phacoemulsification (phaco) chop substitutes manual instrument forces for the sculpting that is required for the stop-and-chop or divide-and-conquer methods.1 Studies have confirmed that chopping reduces the amount of ultrasound energy and power required, and minimises endothelial cell loss.1–5 As a bimanual technique, however, phaco-chop is more difficult to learn and also requires some concurrent ultrasound to either impale the phaco tip or to sculpt a central pit in the case of denser nuclei. Methods to fragment the nucleus prior to introducing the phaco tip include the prechop technique and femtosecond laser nuclear fragmentation.6–9 An over-riding challenge with all of these methods is difficulty in transecting the posterior nuclear plate, especially with advanced brunescent cataracts in which the nucleus is much thicker and in close approximation to the posterior capsule.10
We describe a novel technique for full-thickness nuclear fragmentation using a disposable microinterventional device (miLOOP; IanTech, Reno, NV) without requiring concurrent ultrasound. The manually operated device uses a superelastic, memory-shaped nitinol (nickel titanium) filament to encircle and then divide the nucleus within the capsular bag. This report details our findings in a first-in-human randomised prospective clinical trial (RCT) that compared phacoemulsification with and without miLOOP prefragmentation in a series of dense cataracts.
Materials and methods
The miLOOP device
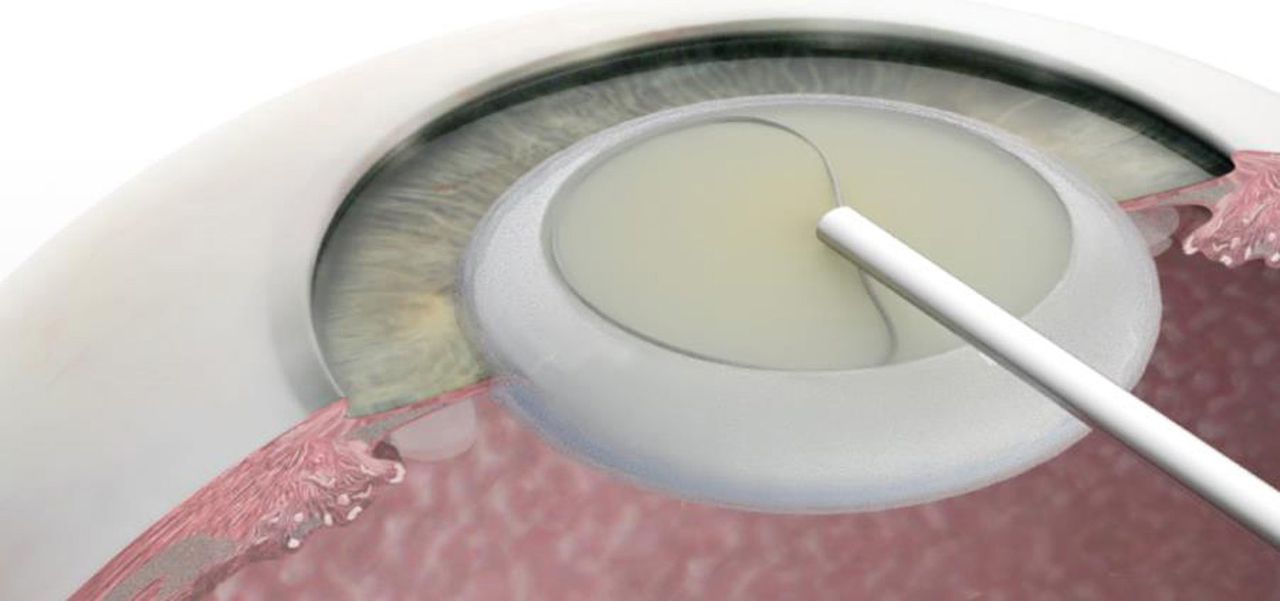
The device has a microthin filament loop made of nitinol alloy whose memory shape and superelastic properties allow alternate contraction to a 1.5 mm radius and expansion to a 10.5 mm radius (figure 1). After completing capsulotomy the instrument tip is introduced through a clear cornea incision into the anterior chamber filled with ophthalmic viscosurgical device (OVD). Advancing a sliding actuation button on the handle opens the nitinol filament loop within the capsular bag. The initial loop expansion is performed in the coronal plane just beneath the anterior capsule (figure 2). The surgeon next sweeps the fully expanded loop back along the hydrodissection plane against the internal capsular contour until it encircles the nucleus in the sagittal plane. Sliding the handpiece button backward contracts the loop until the metal filament completely transects the nucleus. For denser nuclei, a second instrument may be used to steady the nucleus as it is being cut. After rotating the nucleus, the same manoeuvres are repeated to divide the nucleus into quadrants. An additional optional cut will divide the nucleus into six pieces, if desired.
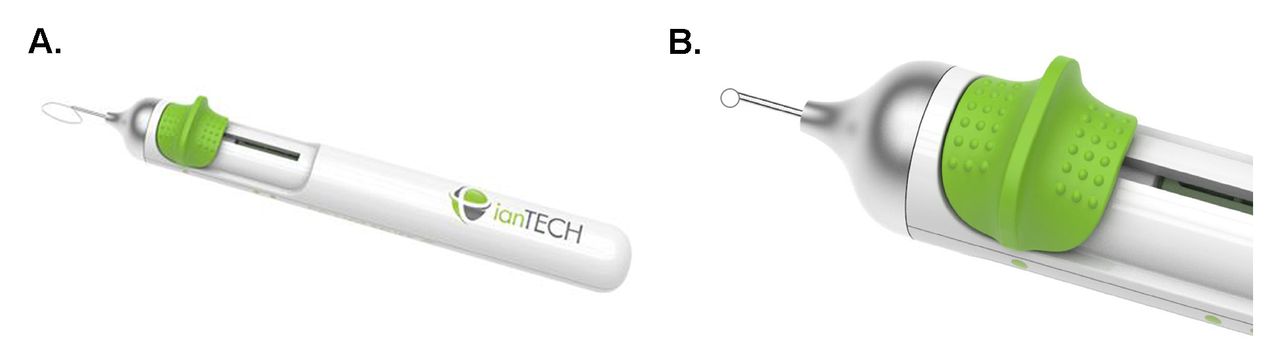
The miLOOP device (A) is a handheld single-use unit with a sliding actuator button that controls expansion and constriction (B) of a cutting loop constructed of a single 300 µm diameter nitinol microfilament.

miLOOP expansion in the coronal hydrodissection plane prior to nuclear encirclement, endocapsular rotation and first nuclear bisection.
The nitinol filament is 300 μm in diameter and was structurally designed to optimise elasticity, memory and cutting force. Microfilaments thinner than 100 μm in diameter are too compliant for satisfactory endocapsular unfolding, resulting in poor nucleus-encircling ability. The mechanical dynamics of how the loop unfolds and its memory shape are engineered to accommodate all sizes and grades of nucleus. The flexible loop’s smooth outer surface precisely and dynamically matches the curved inner contour of the capsule. These characteristics minimise deformation of the surrounding capsular bag during loop expansion and cataract encirclement. Upon retraction of the device actuating button, the constricting loop cuts through the nucleus using centripetal constricting forces directed inwardly away from the capsular bag.
Preclinical modelling and experimentation was conducted during development and design of the miLOOP device to optimise proper architecture, physical properties and mechanical behaviour of the microthin nitinol filament. The dynamic behaviour of the microfilament during expansion was carefully engineered so that it unfolds slowly, smoothly and segmentally in the coronal plane without excessive capsular pressure or distortion. In human cadaver eye testing, Miyake-Apple posterior video analysis confirmed atraumatic, tension-free movement of the microfilament along the posterior capsule (figure 3). The unit is fully operable using only one hand.

{kind=link}
{kind=link}
{kind=link}
Miyake-Apple view of the microinterventional loop in a sagittal endocapsular position prior to initiating a full-thickness nuclear cut (A) and midway through the bisection (B). Panel (C) shows the dissection plane of the cleanly bisected nucleus (human cadaver study).
Clinical study
This prospective, multisurgeon RCT (ClinicalTrials.gov NCT02843594) was performed at the Clínica de Ojos Orillac-Calvo, Panama City, Panama. One eye from each of 101 subjects was randomised to conventional phaco or to phaco preceded by adjunct microinterventional nuclear fragmentation with the miLOOP. All patients provided written informed consent. The study protocol was approved by the study site Institutional Review Board, and conformed to the Declaration of Helsinki.
Inclusion criteria included an advanced visually significant nuclear cataract of ≥grade 3nuclear sclerosis with best corrected visual acuity (BCVA) limited to 0.33 decimal (20/60 Snellen) or worse. Eyes with significant anterior segment comorbidity besides an advanced cataract that could complicate the procedure were excluded, including corneal opacity, zonulopathy or trauma history.
After a variable-block, digitally generated 1:1 randomisation to miLOOP-assisted phaco or standard phaco, all subjects underwent cataract surgery under topical anaesthesia by one of six experienced phaco surgeons. Patients were masked to treatment assignment. Observers but not surgeons were masked to treatment assignment. No surgeon performed <8 cases. Provisc OVD (Alcon, Fort Worth, TX), 2.7 mm clear cornea incisions and the Centurion Vision phaco platform (Alcon) with customised torsional power settings were used for all cases. All surgeons used their preferred phaco-chop technique, and only resorted to a divide-and-conquer technique when deemed necessary by the operator. When using the miLOOP device, microinterventional sectioning was done after the hydrodissection step beneath the OVD and prior to inserting the phaco handpiece.
Subjects received a standard preoperative regimen of topical antibiotics for 3 days prior to surgery, and postoperative 1 week of topical antibiotics and 4 weeks of topical steroid and non-steroidal anti-inflammatory drops. Follow-up examinations were performed 1 day and 1 month postoperatively. The primary outcome in this study was phaco energy required for nuclear emulsification, measured by the cumulative dispersed energy (CDE) recorded by the phaco machine. All eyes had preoperative and 1-month postoperative endothelial cell counts using Konan CellChek Specular Microscopy (Konan Medical, Irvine, CA). Intraoperative complications and those occurring ≤1 month postoperatively were tabulated. Central corneal endothelial cell density, corneal thickness and BCVA were evaluated at baseline and postoperative 1 month.
Results
Subjects (n=101) were enrolled and their study eye randomised to either the miLOOP or control phaco group. Four subjects originally randomised to control phaco surgery underwent miLOOP instead; because of severity and density of their highly brunescent cataracts the surgeon thought miLOOP-assisted phaco was safer than converting to extracapsular cataract extraction. For safety and efficacy analyses, those cases were included in the miLOOP group. One subject randomised to the miLOOP group had significant capsular adhesions and instability from prior ocular inflammation, and the surgeon opted to use the standard phaco technique. For safety and efficacy analyses, the miLOOP group contained 53 subjects and the control group contained 48 subjects.
Baseline characteristics are compared in table 1. The cohort averaged 68.7 years old and was 50% female. All study cataracts were advanced, that is, Lens Opacities Classification System III grades 3‒4. Mean preoperative endothelial cell density, axial length and BCVA (20/360 Snellen or worse) were comparable in the operated eye of both groups. Most eyes in control and miLOOP groups had 20/400 or worse vision—with 87.5% and 84.6% 20/200 BCVA or worse and 58.3% and 59.6% BCVA of count fingers or worse, respectively. There were nine (18%) cases of pseudoexfoliation in the control group and 10 (19%) in the MiLOOP group.
Baseline characteristics
Operative data are shown in table 2. Full-thickness lens segmentation was achieved in 100% of miLOOP cases, and prefragmentation significantly lowered both necessary energy delivery during emulsification and surgical irrigation fluid volume used. Control phaco eyes required 53.3% greater mean CDE for cataract disintegration than miLOOP eyes, and exhibited larger interindividual variability as evidenced by the larger SD and range. The effective time required for phaco did not differ in the miLOOP and control groups (1.7±1.0 min vs 1.5±1.0 min, respectively (p=0.315)). Prefragmentation with the miLOOP device was performed in less than 3 min in all subjects, and required no or minimal additional OVD.
Intraoperative procedures and parameters
Intraoperative and postoperative complication rates were comparable between both groups (table 3). There was a trend towards a lower rate of capsular tear during the phaco portion of the procedure with miLOOP-assisted phaco (7.5%) compared with standard phaco (10.4%). In the miLOOP-assisted phaco group, there was one case of capsular tear related to the intraocular lens (IOL) inserter when implanting the IOL. Endothelial cell loss averaged <10% at 1 month in both groups, demonstrating a high level of phaco surgical proficiency for the surgeons; control eyes displayed a trend of a 20% greater cell loss versus miLOOP-assisted eyes, though this difference was not significant. Corneal thickness measurements were similar between treatment groups, and were essentially identical to baseline values, in both groups. Corrected acuity at 1 month was similar between both groups, with the miLOOP-assisted phaco eyes achieving a mean BCVA of 0.74 decimal units (20/27 Snellen) and the unassisted control phaco group averaging 0.83 decimal units (20/24 Snellen). No cases of early posterior capsular opacification were observed through the 30-day follow-up period.
Intraoperative and postoperative complications
Discussion
As a method of nuclear disassembly, chopping techniques consistently reduce overall ultrasound time and energy compared with methods that rely on sculpting to divide the nucleus.1–5 This reduction in ultrasound power would be most apparent with denser lenses, which increases expected endothelial cell loss.11 12 This may explain the reduction in endothelial cell loss with phaco-chop compared with sculpting techniques reported in some studies.4 5 Other reports have similarly shown a reduction in ultrasound time and endothelial cell loss with femtosecond laser-assisted cataract surgery by presumably reducing or eliminating the need for sculpting of the nucleus.7–9 However, one large prospective, case-controlled trial found a statistically higher rate of postoperative cornea oedema with the femtosecond laser compared with manual phaco.13
This is the first clinical comparison of microinterventional miLOOP-assisted phaco to standard phaco. We tested miLOOP efficacy and safety in a population comprising exclusively advanced cataracts. As an adjunctive method of presegmenting the nucleus, the miLOOP technique was 100% effective in fragmenting every dense nucleus within the capsular bag. There were no instances of zonular dialysis or anterior or posterior capsule tears occurring during miLOOP nuclear segmentation. Unlike conventional prefragmentation techniques such as chopping, the microfilament follows the already created hydrodissection plane and the cutting force is centripetally directed inward as the loop closes. This is likely the reason for the atraumatic relationship between the loop and the capsule, and the lack of untoward capsular changes during prefragmentation in this study. However, there was a higher rate of PCR during nuclear emulsification in both groups, attributable to the high surgical complexity and severity of cataracts in this population where most subjects had 20/400 BCVA or worse at baseline. Nevertheless, the PCR rate was no higher in the miLOOP group than in the conventional phaco control group. Five of the six study surgeons were visiting and therefore operating in an unfamiliar facility. One instance of PCR occurred as a complication of IOL injection.
In this population having very dense cataracts, the miLOOP-assisted phaco technique achieved a statistical reduction in CDE and in irrigation fluid volume used per case. It is noteworthy that phaco-chop employing a latest generation phaco machine with torsional ultrasound was used for all cases. As with phaco-chop, non-longitudinal ultrasound reduces CDE when compared with longitudinal ultrasound.14 That the miLOOP-assisted phaco method was able to significantly reduce CDE even further suggests that there may be other potential advantages to manually sectioning the nucleus in advance without ultrasound. A detailed video review of the cases suggested that segment removal and emulsification occurred more easily and efficiently in the miLOOP-assisted group. We speculate that the peripheral endocapsular sweep of the miLOOP filament mechanically separates the epinucleus from the lens capsule along the hydrodissection plane. This may further facilitate aspiration and removal of presectioned lens fragments compared with performing hydrodissection alone. Cortex removal also appears to be expedited by this mechanical endocapsular wiping effect.
Dividing the posterior nuclear plate is the most difficult step with all nuclear disassembly methods, and is particularly challenging with dense nuclei. Compared with other methods, an important mechanical difference with miLOOP nuclear fragmentation is that the capsular bag is never subjected to any centrifugally directed instrument forces. With divide-and-conquer a deep trench is sculpted to score and thin the nucleus centrally until outward separating instrument forces can crack the residual posterior plate. With phaco-chop, the chopper initially moves centripetally towards the phaco tip to generate a partial-thickness nuclear split. Outward separating movements of the instrument tips then propagate the fracture through the remaining nucleus. With the Akahoshi prechopper, the paired blades are first driven into the centre of the nucleus after which a forceful separation of the blades fractures the nucleus. Finally, many surgeons sculpt a central pit prior to initiating phaco-chop with a very dense and thick nucleus. This permits the phaco tip to more deeply impale the nucleus to stabilise it against the force of the chopper. In contrast, the miLOOP filament completely transects the nucleus without any centrifugally directed instrument forces that would stress or stretch the capsular bag, and without any concurrent ultrasound at all.
In our series there were four (7.5%) cases of posterior capsule tears in the miLOOP group and five (10.4%) in the control phaco group. Of those, one in each group occurred during IOL implantation after completion of uneventful cataract extraction. This rate is higher than what we often see generically reported in the phaco literature for standard cataract cases. In this study, we used only highly experienced phaco and anterior-segment surgeons and the latest generation phaco equipment. The cataract population, on the other hand, was anything but average—almost all cases were hard mature and brunescent cataracts so advanced that almost 90% of cases had baseline BCVA of 20/200 or worse. Also, 18%–19% of cases had pseudoexfoliation. So, we examined closer the peer-review literature for the rate of cataract surgical complications in such highly advanced cases of hard nuclei, often buried in the subgroup analyses of larger data sets. One of the largest outcome peer-reviewed studies of phaco cataract surgery in 55 567 patients from the UK National Database reported a PCR rate of 1.92% across all cases.15 Furthermore, the OR in dense cataracts was 2.99 with observed rate of ≥6%. Many similar studies are consistent in reporting an increased rate of complications and unique challenges in such distinct populations of advanced cataracts.16–20
Automating nuclear fragmentation prior to phaco is one purported advantage of femtosecond laser-assisted cataract surgery. Despite the higher procedural costs, this might be particularly appealing for the many surgeons who are not adept or comfortable with chopping techniques. However, the need to leave a 150‒250 μm safety buffer between the posterior capsule and the deepest laser shots means that full-thickness nuclear fragmentation is frequently not achieved. In contrast, the miLOOP is a relatively inexpensive disposable instrument that can be used in the normal surgical sequence without disrupting operating room efficiency, and without requiring additional patient payment.
The study was limited only to advanced cataracts as a means to test the functional limits of the miLOOP technology. Potential advantages for soft to medium density cataracts or for other complicated eyes were not tested in this study. Although there was a trend towards lower endothelial cell loss in the miLOOP eyes, this study was too small to identify statistical significance and an independent specular microscopy reading centre was not used. However, we confirmed the effectiveness and safety of mechanically transecting and prechopping extremely dense nuclei prior to phaco. Further clinical studies will better establish the merits and any potential shortcomings of this new technology.
Acknowledgments
The authors thank Matthew Silverman PhD (Biomedical Publishing Solutions; Delray Beach, FL) for exemplary scientific, analytical, and writing assistance.
References
Footnotes
Contributors Conception and design of the study (TI, EC); data collection (TI, EC); analysis and interpretation (TI, DFC, EK, SM, EC, FTT, AV, IIKA); writing of the article (TI, DFC, EK, SM, EC, FTT, AV, IIKA); critical revision of the article (TI, DFC, EK, SM, EC, FTT, AV, IIKA); final approval of the article (TI, DFC, EK, SM, EC, FTT, AV, IIKA); obtained funding (TI); literature search (TI, EC); administrative, technical or logistic support (AV).
Funding This study was funded by IanTech, the device manufacturer.
Competing interests TI is the CEO of IanTech. DFC is a consultant for IanTech and has an ownership interest in the company. EK, EC and FTT have financial interests in IanTech. SM is a consultant for IanTech and Perfect Lens. AV received study funding from IanTech. IIKA has a consultancy (C), or received speaker fees (S) or research funding (R) from: Abbott Medical Optics (AMO), C,S,R; Acucela, C; Aerie Pharmaceuticals, C,R; Alcon, C,S,R; Allergan, C,S,R; ArcScan, C; Bausch and Lomb, C; Carl Zeiss Meditec, C,S,R; Centervue, C; Clarity Medical Systems, C; ElutiMed, C; Envisia Therapeutics, C; Equinox, C; Eyelight, C; ForSight Labs, C; Glaukos, C,R; Gore, C; IanTech, C; InjectSense, C; InnFocus, C; Iridex, C; iStar, C; Ivantis, C,R; KeLoTec, C; LayerBio, C; Leica Microsystems, C; New World Medical, C,R; Omega Ophthalmics, C; Ono Pharma, C; PolyActiva, C; Sanoculis, C; Santen, C; Science Based Health, C; SOLX, C; Stroma, C; TrueVision, C.
Patient consent Obtained.
Ethics Approval The study protocol was approved by the Institutional Review Board of the Clínica de Ojos Orillac-Calvo, Panama City, Panama.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance