
Abstract
Purpose To report a case of peripapillary choroidal neovascularization (CNV) complicating serpiginous choroiditis that was treated by a single indocyanine green (ICG)-mediated photothrombosis session combined to intravitreous triamcinolone acetonide (TA) injection.
Methods Interventional case report. A 48-year-old patient with peripapillary CNV was submitted to a laser-dye-mediated technique that uses ICG and low-intensity 810-nm light for continuous laser application; TA was then injected into the vitreous cavity 1 hour later, and prospective evaluation with fluorescein and ICG angiography as well as optical coherence tomography (OCT) was performed.
Results At 2 weeks after treatment, best-corrected visual acuity improved from 20/200 to 20/50, with further improvement to 20/20−1 in the subsequent 10 weeks. Absence of fluorescein leakage from the CNV and OCT evidence of resolved retinal oedema was observed at that time. Clinical stabilization was maintained up to 1 year of follow-up. There was no significant complication related to the procedure.
Conclusion Combined ICG-mediated photothrombosis and intravitreous TA induced rapid and significant visual acuity recovery in this particular case of peripapillary CNV complicating serpiginous choroiditis. Accordingly, angiographic and OCT findings demonstrated neovascular lesion regression and restoration of the macular architecture.
Similar content being viewed by others


Main
Serpiginous choroidopathy is a chronic recurring disorder, usually bilateral and asymmetrical, which primarily affects the choriocapillaris and retinal pigment epithelium with disruption of the overlying neurosensory retina. The aetiology is uncertain, although an inflammatory cause has been suggested.1 Clinical course of this progressive disease varies, particularly with regard to the central vision prognosis. Although slow visual recovery is likely to occur,2 profound visual loss happens if foveal or parafoveal areas are involved or secondary choroidal neovascularization (CNV) development is noticed.3 This communication reports the treatment and follow-up of one patient with serpiginous choroidopathy, complicated with a peripapillary CNV, who was treated with combined indocyanine green (ICG)-mediated photothrombosis and intravitreous triamcinolone acetonide (TA) injection.
Case report
A 48-year-old white man with no previous systemic disease complained of decreased visual acuity in the right eye 1 week prior to presentation. His best-corrected visual acuity (BCVA) was 20/80 in the right eye and 20/20 in the left eye. Ophthalmologic examination revealed asymmetrical scarring with clumping and loss of retinal pigment epithelium (RPE), and destruction of the choroidal vasculature in the peripapillary region of both eyes. Some inflammatory cells were observed in the posterior vitreous and one foci of active choroiditis was suspected in the right eye. No other signs such as peripheral retinal lesions, optic disc involvement, polypoidal lesions, and angioid streaks were encountered. The diagnosis at that time was serpiginous choroiditis based on these findings and in the results of serologic tests and haematological evaluation. Oral corticosteroids were prescribed and by 2 weeks, the BCVA had further decreased to 20/125+2 caused by a subretinal haemorrhage involving the macular region and increase in retinal oedema. Fluorescein and ICG angiography revealed a CNV emanating from the leading edge of the peripapillary scar (Figure 1a-d). Since BCVA dropped to 20/200 even in the presence of oral medication because of CNV progression and enlarged subretinal haemorrhage in the following 2 weeks (Figure 1e), ICG-mediated photothrombosis was proposed to the patient. The decision for the combined procedure with intravitreous TA injection was based on the presence of residual vitreous cells at the last examination prior to treatment.

Red-free fundus photography demonstrating typical aspect of peripapillary scarring with fingerlike extensions oriented superiorly and inferiorly in the right eye. Subretinal haemorrhage and increased retinal oedema within the papillomacular bundle region was seen 2 weeks after presentation. A suspected focus of active choroiditis was seen along the superotemporal vessels (arrowhead). Peripapillary chorioretinal scar with superonasal fingerlike extension and pigment clumping was also seen in the left eye. (c) Late-phase ICG angiography at that time demonstrated hypofluorescent areas consistent with loss of choriocapillaris and RPE commonly observed in healed areas of serpiginous choroiditis. An active CNV adjacent to the leading edge of the old scar at the temporal aspect of the optic disc (arrows) was seen. Subretinal haemorrhage blocks fluorescence in the macular area. Mild hyperfluorescence at the suspected region of choroiditis was also seen (arrowhead). (d) Multiple hypofluorescent spots throughout the macula and the peripapillar region of both eyes were demonstrated by late-phase ICG angiography. Note that angiographic alterations were confined to the posterior pole. (e) At 2 weeks after CNV detection, further increase in the area of the subretinal haemorrhage and exudation was observed caused by the extension of the CNV inferiorly. Dotted lines represent the delineation of the suspected neovascular lesion. (f) Late-phase ICG angiography taken after laser treatment and 5 min before intravitreal triamcinolone injection. Two spots (dotted lines) positioned first over the inferior CNV part, and secondly over the superior part were used for laser applications. (g, h) Early-phase fluorescein and ICG angiography taken 12 weeks after combined treatment showed an absence of fluorescein leakage from neovascular lesion and resolution of subretinal haemorrhage. A well-defined irregular hypofluorescent region corresponding to the entire neovascular lesion seen in fluorescein angiograms before treatment was evidenced on ICG angiography. Note that the deeper choroidal vasculature within the area correspondent to the former CNV was preserved and no angiographic alteration was identified in the normal tissues involved in the treatment spot area.
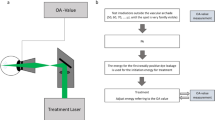
ICG-mediated photothrombosis is a modality of laser-dye treatment that uses large-spot, low-intensity 810-nm light to apply laser energy continuously to an area where ICG has been highly concentrated,4 used recently in the management of CNV associated with age-related macular degeneration.5 The study protocol was approved by the local institutional review board and a written informed consent was obtained before treatment. For the procedure, a loading dose of 2.0 ml of a highly concentrated solution of ICG (25 mg/ml (approximately 1 mg/kg body weight)) was administered as an i.v. bolus, followed immediately by a 5.0-ml saline flush. At 20 min after the loading dose, a second i.v. injection of 50 mg of ICG in 2 ml of solution was administered, followed by a 5.0-ml saline flush. At 90 s after the second flush infusion, a diode laser at 810 nm (Trimode-L, OPTO, São Carlos, Brazil) with a slit-lamp delivery system was used at an intensity of 5.6 W/cm2 over 90 s to deliver light to the fundus utilizing a 2.25 mm spot. The spot was positioned initially at the inferior part of the CNV and secondly at the superior CNV part. At 20 min after the conclusion of the first laser applications, light dose at the same parameters was applied a second time in the exactly same positions at the fundus (Figure 1f). An intravitreous injection of 0.1 ml containing 4 mg of TA was then performed 60 min after the second (and last) laser applications (Figure 2b). By 2 weeks, the BCVA improved to 20/50 and optical coherence tomography (OCT) demonstrated a reduction in retinal elevation and subretinal fluid (Figure 2 a, c). At 12 weeks, vision improved to 20/20-1, and OCT revealed a complete restoration of the macular architecture and a quiescent neovascular lesion in the peripapillary region (Figures 1g, h, and 2d). At 1 year after treatment, BCVA remained stable and no fluid was detected on OCT evaluation (Figure 2e, f). No significant alteration in intraocular pressure was seen during follow-up and there were no complications related to the procedure.

Horizontal 5 mm OCT scans passing through the fovea and colour fundus photography of the same patient of Figure 1. (a) Prior to treatment, increased retinal thickness and elevation caused by intraretinal and subretinal fluid accumulation in the subfoveal region (arrow) extending towards the optic disc was observed. Fragmentation and fusiform thickening of the reflective band corresponding to the RPE and choriocapillaris was seen in the area of the active choroidal neovascularization (arrowheads). (b) Fundus appearance immediately after intravitreal injection of TA. (c) Marked resolution of intraretinal oedema and subretinal fluid as well as restoration of the foveal contour (arrow) was seen 2 weeks after the combined procedure; a focal area of enhanced choroidal reflectivity corresponding to the quiescent neovascular lesion was disclosed by OCT (white arrowhead). (d) After 12 weeks of follow-up, OCT revealed normal retinal thickness and a small region of increased optical reflectivity from the choroid caused by some RPE atrophy within the area of the former neovascular lesion. (e, f) Fundus appearance 1 year after combined therapy; no further recurrences were seen and OCT revealed that the neovascular lesion remained quiescent and no change in retinal thickness was observed after 12 months of follow-up.
Comment
Management of peripapillary CNV remains an unsolved matter among retinal specialists. The particular CNV shape and the proximity of the optic disc may lead to difficulties in positioning the circular laser spot for light applications. In the case we described, light application had to be positioned in two separated spots to achieve complete CNV treatment. Additionally, we must consider that depending on the iatrogenic laser-induced damage to the inner retinal layers, irreversible visual field scotoma might occur. The use of an 810 nm laser as well as lower intensity levels for the treatment (at least 100 times lower than that commonly used for fundus photocoagulation) in association with ICG was sufficient to avoid such an effect. Similar association has also demonstrated promising results for the management of haemangiomas6 and metastasis7 involving the choroid.
Taking into consideration that some benefit was achieved after intravitreous TA in exudative age-related macular degeneration8 and that inflammatory factors may also be involved in the pathogenesis of serpiginous choroiditis,1 we believe that association of intravitreal TA to the laser-dye procedure in our patient might have played an important role in the final clinical outcome.
In conclusion, the location of the CNV in the case reported was within the papillomacular bundle, allowing the possibility of a severe visual acuity to occur if conventional laser photocoagulation was performed. Given the visual improvement in this patient, combined ICG-mediated photothrombosis and intravitreal TA may be an effective tool in the management of CNV in patients with serpiginous choroiditis. Whether or not the sole use of intravitreal TA or ICG-mediated photothrombosis responds in a similar manner to the combined technique for CNV treatment in serpiginous choroiditis requires further investigation.
References
Laatikainen L, Erkkila H . Serpiginous choroiditis. Br J Ophthalmol 1974; 58: 777–783.
Annesley Jr WH, Shields JA, Tomer T, Christopherson K . The clinical course of serpiginous choroidopathy. Am J Ophthalmol 1979; 87: 133–142.
Jampol LM, Orth D, Daily MJ, Rabb MF . Subretinal neovascularization with geographic (serpiginous) choroiditis. Am J Ophthalmol 1979; 88: 683–689.
Costa RA, Farah ME, Freymuller E, Morales PH, Smith R, Cardillo JA . Choriocapillaris photodynamic therapy using indocyanine green. Am J Ophthalmol 2001; 132: 557–565.
Costa RA, Farah ME, Cardillo JA, Belfort Jr R . Photodynamic therapy with indocyanine green for occult subfoveal choroidal neovascularization caused by age related macular degeneration. Curr Eye Res 2001; 23: 271–275.
Kamal A, Watts AR, Rennie IG . Indocyanine green enhanced transpupillary thermotherapy of circumscribed choroidal hemangioma. Eye 2000; 14: 701–705.
Puri P, Gupta M, Rundle PA, Rennie IG . Indocyanine green augmented transpupillary thermotherapy in the management of choroidal metastasis from breast carcinoma. Eye 2001; 15: 515–518.
Danis RP, Ciulla TA, Pratt LM, Anliker W . Intravitreal triamcinolone acetonide in exudative age-related macular degeneration. Retina 2000; 20: 244–250.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Navajas, E., Costa, R., Farah, M. et al. Indocyanine green-mediated photothrombosis combined with intravitreal triamcinolone for the treatment of choroidal neovascularization in serpiginous choroiditis. Eye 17, 563–566 (2003). https://doi.org/10.1038/sj.eye.6700457
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.eye.6700457
Keywords
This article is cited by
-
Indocyanine-green-mediated photothrombosis (IMP) with intravitreal triamcinolone acetonide for macular edema secondary to group 2A idiopathic parafoveal telangiectasis without choroidal neovascularization: a pilot study
Graefe's Archive for Clinical and Experimental Ophthalmology (2007)
-
Indocyanine green-mediated photothrombosis with intravitreal triamcinolone acetonide for subfoveal choroidal neovascularization in age-related macular degeneration
Graefe's Archive for Clinical and Experimental Ophthalmology (2005)
