
Abstract
Aims To determine the overall reported incidence and causes of registrable blindness and visual impairment in the West of Scotland and any trends that have occurred in the previous 16 years since data from the same area were published.
Methods Data for analysis were obtained from BP1 registration forms returned to the Resource Centre for the Blind serving the Strathclyde region in the West of Scotland between 1 April 1996 and 31 March 1997.
Results A total of 1595 visually handicapped people were registered during the study year. Of these, 99 forms (6.2%) were excluded from further analysis because of insufficient information. The remaining 1496 completed BP1 Forms were in respect of 530 males and 966 females. Of these, 253 males and 450 females were legally blind (total 703 or 47.0%) and 277 males and 516 females were partially sighted (total 793 or 53.0%). The five leading causes of blindness, in decreasing frequency, were age-related macular degeneration (ARMD), glaucoma, diabetic retinopathy, myopic degeneration, and optic atrophy. ARMD and diabetic retinopathy were the most common causes of blindness in those over 65 years and persons of working age, respectively.
Conclusions In adults, cataract is no longer a significant cause of registrable visual impairment. The proportions of registrations owing to glaucoma, diabetic retinopathy, and myopia have not significantly changed since 1983 and the proportion owing to macular degeneration has increased. In children, congenital glaucoma, cataract, and corneal infection were no longer causes of registration, but impairment of vision caused by brain damage is now a significant contributor.
Similar content being viewed by others


Introduction
Since Sorsby1,2 published his extensive analysis of causes of blindness and Ghafour et al reported their analysis for 1983 for the Strathclyde region and Evans et al in 1990–1991 for England and Wales,3,4,5 there have been a number of developments in the management of many sight-threatening disorders. Cataract, glaucoma, age-related macular degeneration (ARMD), retinal detachment, diabetic retinopathy and other forms of retinal vasculopathy, tumours and trauma are treated differently. Notable advances include extracapsular and phacoemulsification cataract extraction, and vitreoretinal surgery. However, disorders such as myopic degeneration and most hereditary eye diseases remain untreatable. Changes in the statistics for registration of blindness and partial sight may therefore be anticipated.
Blind registration in the UK is voluntary. The principal criterion for registration is that the person is so blind as to be unable to perform any work for which eyesight is essential. Table 1 summarises the guidelines for registration by an ophthalmologist who completes BP1 Form for Scotland or BD8 Form for England and Wales. The data sought are very similar. Partial sight registration is carried out for those who are substantially and permanently affected by poor vision.6
The principal causes of blindness in the Strathclyde region in the West of Scotland, determined from blind registration data, were previously reported for the year ending 31 December 1980 by Ghafour et al.5 The aim of this study is to present the 1996–1997 blind and partial sight registration figures for the same geographic area.
Materials and methods
BP1 Forms submitted for the calendar year between 1 April 1996 and 31 March 1997 and returned to the Resource Center for the Blind in Glasgow and the West of Scotland were studied and analysed. These forms relate to people resident in the same territory as that described in the previous paper by Ghafour et al.5
The registrations were divided into ‘blind’ and ‘partially sighted’ according to the way in which the BP1 Forms had been completed by the examining ophthalmologist. As the registration of blindness and partial sight depends on the status of the better eye, a further evaluation of the forms was undertaken with respect to visual acuity and visual field loss. Accordingly, all forms were recategorised with reference to the definition on the BP1 Form described in Table 1.5
A total of 1595 visually impaired people were registered for the Strathclyde region during the year 1996–1997. In all, 99 incomplete forms (6.2% of the total) were excluded from further analysis because of lack of essential information. These rejected forms contained missing information about the cause of the visual handicap and the best corrected visual acuity of the person being registered. Most of these forms had been submitted from an area with no apparent abnormal incidences of the causes of blindness, as determined from a study of all other forms returned from the same area.
The data from the 1496 completed forms were recorded using the computer program Microsoft Excel 1997. These comprised age, sex, address, postal code, best corrected visual acuity, visual field data, and the primary cause of visual impairment in both eyes. The age at onset of visual handicap and the age at time of registration were also recorded.
The population estimate of the Strathclyde region of the West of Scotland for mid-1996 based on the 1991 census was 2.4 million (46% of the population of Scotland) and this compares with the population in the West of Scotland 16 years earlier, which was also 2.4 million.7,8
For the purpose of analysis, patients were divided into the following age groups: 0–16 years (children), 17–64 years (working ages), 65–74, 75–84, 85+ years. The census data8 were employed to determine the number of registrations per 100 000 population with respect to the age group presented.
Results
Of the 1496 completed BP1 Forms, 703 (47.0%) were for blind registered patients and 793 (53.0%) were for the partially sighted. (The numbers of forms that were recategorised were 13 for partial sight registration to blind registration and 118 for blind registration to partial sight registration.) Thus, the overall registered blindness rate was 29.7 per 100 000 population and the partial sight rate was 33.5 per 100 000 population per annum. The 1496 completed BP1 Forms were in respect of 530 males and 966 females. The male-to-female ratio was 1 : 1.8 for the total registrations, for both the blind registrations and the partial sight registrations. The male-to-female ratio in the population as a whole in the Strathclyde region is 1:1. Table 2 compares the information from completed BP1 Forms in both the 1980 and 1996–1997 1-year study periods.
Table 3 shows the number of blind and partial sight registrations, and the registrations per 100 000 population for both males and females in the different age groups. As expected, the numbers of the legally blind and partial sight registrations become greater with advancing age, and the registration rate rises sharply over 65 years of age. The peak for registrations occurred in the 75 to 84-year age group. In all, 37.8% of all registrations fell in this age group and 76.7 % of all registrations were for those aged 65 years and above. There is a higher rate of blind and partial sight registration of women in the older age groups.
Registration is usually carried out some time after the onset of visual impairment; thus the distribution for ‘age at registration’ is shifted to an older age than that for ‘age at onset’. The median time between the onset of the visual defect and registration was 1 year. In total, 65.9% of registrations were made within 2 years of the onset of blindness, but 1.8% (27) registrations were made more than 25 years after the person became visually impaired.
Tables 4 and 5 show the data concerning the numbers of the primary causes of visual impairment for both the legally blind and the partially sighted in the different age groups. The age distributions of the different disorders reflect the expected patterns of presentation.
Discussion
The population of the Strathclyde region is relatively stable and homogeneous, and both the environment and the level of health care are uniform. Although the guidelines described in the Introduction are provided to aid the ophthalmologist in deciding whether a patient should be registered ‘blind’ or ‘partially sighted’, some subjectivity evidently enters into the decision. To minimise this subjective element, the UK criteria for legal blindness and partial sight were applied to the data as described for the 1980 study.5
Comparisons with other studies are difficult because many different definitions of blindness are in use; the World Health Organization has accepted some 65 definitions of blindness.9 In this study, we used the same criteria for definition of blindness and a similar method of analysis used in the previous study of the same region.
The overall numbers and the number per 100 000 population for blind and partial sight registration have more than doubled since 1980 (Table 2). This may reflect a greater awareness of the benefits of registration by doctors and patients alike. The introduction in 1985 of a fee paid to ophthalmologists for registering patients may also have contributed. A real increase in the incidence of specific disorders such as ARMD is also potentially a factor. Aging of the population as a whole may also be a contributory factor.
For both males and females, the rates of blind and partial sight registration remain low until age 55 years, after which there is a considerable increase, especially after the age of 65 years (Table 3). The higher numbers of women in the older age groups who have been registered are consistent with previous studies. Greater life expectancy, a greater desire among women to be registered, and differences in disease prevalence may all contribute.
Compared with the data presented in the study by Ghafour et al,5 the rate of blind registration is similar in the younger age groups (0–64 years), although the sample size was small, making it difficult to draw any definite conclusions. In the present study, cortical blindness and optic atrophy comprise the most common causes of blind registration in children (0–16 years old). These diagnoses did not figure in the study by Ghafour et al.5 This may be explained by the increased recognition of these cases in a recently established vision assessment clinic in Glasgow. This clinic is specialised in examining and assessing mentally and visually handicapped children. Retinal dystrophies were also a common reason for blind registration in this age group. Unlike the previous study, congenital glaucoma, congenital cataract, and corneal infections were not recorded as causes of registrable blindness, presumably on account of improved ophthalmic services for this age group.
Diabetic retinopathy was the most common reason for blind registration in the working age group (17–64 years old). The percentage of diabetic retinopathy as a cause of blind registration has improved marginally from 8.5% in the study by Ghafour et al5 to 7.0% in our data, but the total number registered has increased. The number of cases registered with retinitis pigmentosa has also increased compared to the previous study. This may similarly relate to a retinitis pigmentosa clinic established since the previous report.
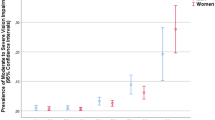
The proportion of cases of ARMD as a cause of blind registration rises from 54% among the 65- to 74 years olds, to 64% among the 75- to 84-year olds, and to 83% among the 85+ year old age group. Registration for blindness and partial sight Owing to ARMD appears to be increasing as a proportion of overall registrations (Sorsby 1955–1960: 26.9%; Ghafour 1980: 29.8%; Avon study 1985–1986: 49%; present study 1996–1997: 52.4%).1,2,5,10 In the present study, as age increases, the number of patients registered blind per 100 000 population Owing to ARMD increases from 39.3 in the age group 65- to 74-year olds to 288 in 85-year olds and over.
Glaucoma was found to be the second most common cause of blind registration over the age of 65 years. The percentage for glaucoma has shown little change (13.8% in our data and 14.6% in the Ghafour et al study). Whether this represents a true increase or reflects greater numbers of registrations being carried out is unknown.
In the present study, cataract was not a major cause of blind registration and was only described as a cause of visual impairment in 13 patients. In most of the BP1 Forms in which cataract was mentioned as a cause of visual impairment, the registering ophthalmologist mentioned that the patient was unwilling or unfit to undergo cataract surgery. It is encouraging to note that the registrations attributable to senile cataract signify an improvement since the 1980 study5 where 10% of registrations were for this reason.
Myopic degeneration is still one of the five leading causes of blind registration. It remains a major contributor to ophthalmic morbidity in the working age group, and is still an important cause of blind registration in those above the age of 65 years. Optic atrophy is present in all age groups. Compared to Ghafour's study there appears to have been no significant change over the years.
The causes of partial sight registration closely follow those of blind registration except homonymous hemianopia caused by stroke, which was the third most common cause of such registration. ARMD was found to be the most common and glaucoma the second most common cause.
Care is required in the interpretation of registration figures with regard to the prevalence of blindness and visual impairment in the population in general. Our results must be interpreted in the context that registrations reflect hospital-based practice, but do not fully reflect the prevalence of visual impairment in the community.11,12
Two studies have shown that the number of people on the blind and partial sight register is only half of those eligible for registration.11,12 For those who were not registered, the major causes of visual impairment encountered were cataract, glaucoma, diabetic retinopathy, retinal vein occlusion, and ARMD in descending order of frequency.11 Owing to the large number of cataract operations performed and the advances in techniques of cataract extraction, cataract is no longer a major cause of blind and partial sight registration.
References
Sorsby A . The incidence and causes of blindness in England and Wales 1948–1962. Reports on Public Health and Medical Subjects, No. 114, HMSO: London, 1966.
Sorsby A . The incidence and causes of blindness in England and Wales 1963–1968. Reports on Public Health and Medical Subjects, No. 128, HMSO: London, 1972.
Evans JR . Causes of blindness and partial sight in England and Wales 1990–1991. Studies on Medical and Population Subjets Reports No. 57, HMSO: London, 1995.
Evans JR, Rooney C, Ashwood F, Dattani N, Wormald R . Blindness and partial sight in England and Wales: April 1990–March 1991. Health Trends 1996; 28: 5–12.
Ghafour I, Allan D, Foulds WS . Common causes of blindness and visual handicap in the West of Scotland. Br J Ophthalmol 1983; 67: 209–213.
BP1 Form for certification of blindness or defective vision. Issued by the Scottish Office Home and Health Department, St Andrew's House: Edinburgh.
Registrar General, Scotland. Annual Estimate of the Population of Scotland, 1980. HMSO: Edinburgh, 1981.
Registrar General, Scotland. Annual Estimate of the Population of Scotland, 1996. HMSO: Edinburgh, 1996.
World Health Organization. Blindness. World Health Organization Epidemiological and Visual Statistics Report, No. 19, 1966; pp 433–512.
Grey RHB, Burns-Cox CJ, Hughes A . Blind and partial sight registration in Avon. Br J Ophthalmol 1989; 73: 88–94.
Robinson R, Deutsch J, Jones HS, Youngson-Reilly S, Hamlin DM, Dhurjon L et al. Unrecognised and unregistered visual impairment. Br J Ophthalmol 1994; 78: 736–740.
Wormald RPL, Wright LA, Courtney P, Beaumont B, Haines AP . Visual problems in the elderly population and implications for services. BMJ 1992; 304: 1226–1229.
Acknowledgements
We gratefully acknowledge the contribution made by Dr Shona Burman-Roy at the Glaxo Department of Ophthalmic Epidemiology. We also thank Mrs Cath Simpson, Mr Jim Agnew, and Mrs Diane Lawrence at the Centre for the Sensory Impaired People, Glasgow City Council, for their support and help in collecting the data. We also thank the Glasgow City Council, Planning and Research Department for their help in conducting the above study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bamashmus, M., Matlhaga, B. & Dutton, G. Causes of blindness and visual impairment in the West of Scotland. Eye 18, 257–261 (2004). https://doi.org/10.1038/sj.eye.6700606
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.eye.6700606
Keywords
This article is cited by
-
Markedly decreasing incidence of cause-specific blindness in Saxony (Eastern Germany)
Graefe's Archive for Clinical and Experimental Ophthalmology (2021)
-
Two- and three-dimensional topographic analysis of pathologically myopic eyes with dome-shaped macula and inferior staphyloma by spectral domain optical coherence tomography
Graefe's Archive for Clinical and Experimental Ophthalmology (2017)
-
Prevalence and progression of visual impairment in patients newly diagnosed with clinical type 2 diabetes: a 6-year follow up study
BMC Public Health (2011)
-
A genome-wide association study for myopia and refractive error identifies a susceptibility locus at 15q25
Nature Genetics (2010)
-
Rhegmatogenous retinal detachment in Scotland: research design and methodology
BMC Ophthalmology (2009)
