Article Text

Abstract
BACKGROUND Subthreshold (retinal pigment epithelium) photocoagulation is a new photocoagulation method, which treats the retinal pigment epithelium (RPE) and avoids damage to the neural retina. The initial results in this prospective pilot study on various macular diseases are presented.
METHODS 12 patients with diabetic maculopathy (group I), 10 with soft drusen (group II), and four with central serous retinopathy (CSR) (group III) were treated and followed up for 1 year. Treatment was achieved using a train of repetitive short laser pulses (1.7 μs) of a green Nd:YLF laser (parameters: 527 nm, 100 and 500 pulses, repetition rate: 500 Hz, spot size: 160 μm, energies: 70–100 μJ). Laser energy was based on the visibility of test lesions on fluorescein angiography (50–130 μJ). Patients were examined at various times by ophthalmoscopy, fluorescein and ICG angiography, and infrared imaging.
RESULTS After 6 months hard exudates disappeared in six out of nine patients in group I and leakage disappeared in six out of 12 diabetic patients. In group II drusen were less in seven out of 10 patients. In group III serous detachment disappeared in three out of four cases. Visual acuity was stable in all cases. None of the laser lesions was clinically visible immediately. After 1 day most lesions were visible as yellowish RPE depigmentation. After 3 months some of the lesions were visible as hyperpigmented areas but most were not. Fluorescein angiography showed leakage only in the first week. Infrared imaging showed that most lesions can be visualised in groups I and II after a period longer than 1 week as hyperreflective areas.
CONCLUSION This study showed that subthreshold (RPE) photocoagulation is effective in some cases of diabetic maculopathy, drusens, and in CSR. Visibility of laser burns is not always necessary in the treatment of macular diseases presented here. Infrared imaging is an effective and non-invasive way of visualising subthreshold (RPE) laser burns.
- laser
- central serous retinopathy
- drusen
- retinal pigment epithelium
- diabetic macula oedema
- infrared
Statistics from Altmetric.com
Retinal photocoagulation has been used for more than 30 years in various diseases. Laser power is usually adjusted so that a grey or white retinal lesion appears. The value of retinal photocoagulation in various macular diseases—for example, in diabetic macular oedema, is well established. However, the benefit of retinal laser treatment is associated with severe destruction of retinal tissue. Subsequent heat conduction out of the retinal pigment epithelium (RPE), which is the primary absorption site, leads to irreversible thermal denaturation of outer and inner segments.1-5 The biological processes of the therapeutic effect of retinal photocoagulation are poorly understood and may be different in various diseases. In the treatment of diabetic macular oedema the beneficial effect is thought to be the restoration of a new RPE barrier.6 A similar effect is postulated in the treatment of drusen and in the treatment of central serous retinopathy (CSR). In proliferative diabetic retinopathy the most common hypothesis is the destruction of photoreceptors thereby reducing the oxygen consumption of the retina.7 Other theories suggest that laser restores the barrier function of the RPE and leads to the production of a variety of growth factors.8-11 If these latter theories are true, then the destruction of the photoreceptors would be undesirable and unnecessary.
Based on these concepts a photocoagulation technique was developed to treat selectively the RPE sparing of the photoreceptors.2 12 In animal experiments it was shown that this was only reproducibly possible by a train of short pulses and not with conventional continuous wave (CW) laser exposures of, for example, 100 ms duration.3 With short laser pulses energy remains confined to the RPE. No significant heat conduction occurs. Optimal pulse durations are of the order of microseconds (1 μs = 10−6 s) down to 200 ns.2 13
Because of the considerable side effects after conventional photocoagulation new photocoagulation techniques have turned on the use of immediate non-visible CW laser burns for treating, for example, diabetic macular oedema and soft drusen.14 15 Based on our theoretical and experimental work we have chosen to treat various macular diseases with a train of repetitive 1.7 μs pulses of a ND:YLF laser.
Patients and methods
We studied 26 patients, 12 diabetic patients with clinically significant macular oedema (group I), 10 patients with soft drusen (group II), and four patients with long standing central serous retinopathy (CSR) (group III). All patients gave written informed consent to the treatment protocol and to the prospective nature of this study. The protocol was approved by the institutional ethics committee.
In group I six of 12 patients had focal and six had diffuse macula oedema. The mean age of this group 59.3 (SD 7.7) years. Mean visual acuity was 20/20.8 (20/133). There were 11 males and one female patient. The mean of HbA1c was 8.1% (2.1%). In group II (drusen) four patients were male and six female. The mean age was 71.9 (8.3) years. Nine of 10 had soft drusen in one eye, while the fellow eye had already a choroidal neovascularisation, and the remaining one had bilateral soft drusen. Visual acuity was 20/28.2 (20/71.4). The mean age of the four patients with CSR was 44.25 (5.1) years. The duration of the exudation was longer than 3 months in all cases.
Before treatment the following tests were performed on all patients—visual acuity measurements, fundus examination, colour photography and fluorescein angiography, and infrared imaging (Heidelberg Instruments). Infrared imaging was performed by using the Heidelberg machine (Heidelberg Instruments, Heidelberg, Germany), which illuminates the fundus in a confocal mode by 810 infrared light. Indocyanine green angiography (ICG) was performed in all patients with CSR and drusen (Heidelberg Instruments).
After treatment all patients in groups I and II (diabetic macular oedema and soft drusen) were followed after 2 hours, 1 day, 1 week, 1, 3, and 6 months. Examination included visual acuity measurement, fundus documentation, fluorescein angiography, and infrared imaging. Additionally ICG angiography was carried out in group II. All patients in group III (CSR) were followed after 2 hours, 1 day, 1 week, 2 weeks, 3 weeks, and 4 weeks, and later. Examination included visual acuity measurements, fluorescein angiography, and infrared imaging.
All patients in group I (diabetes) had a follow up of 6 months. In group II (drusen) five patients had a follow up of 6 months and the other five patients had a follow up of 1 year. The follow up time of the patients in group III (CSR) varied between 2 months (one patient), 6 months (two patients), and 1 year (one patient).
LASER
For treatment a clinical prototype of a ND:YLF laser was used. The wavelength was 527 nm. The pulse duration of a single pulse was 1.7 μs (full width half maximum). The laser was coupled in a slit lamp (Zeiss, Jena, Germany). During each treatment the pulse shape was recorded by an oscilloscope and saved to a PC. The spot size of the laser beam, as analysed by a beam analyser (Spicron LBA-100A) was about 160 μm in air. Each laser lesion was created by a train of a different number of repetitive laser pulses and different energies. The number of laser pulses applied was 100 or 500. The repetition rate was 500 Hz. Single pulse energy, which varied between 30 μJ and 130 μJ, was evaluated before each treatment by measuring the average power using a power meter (Scientech 100). Laser exposure was applied by using a plano concave Goldmann lens.
TREATMENT PROTOCOL
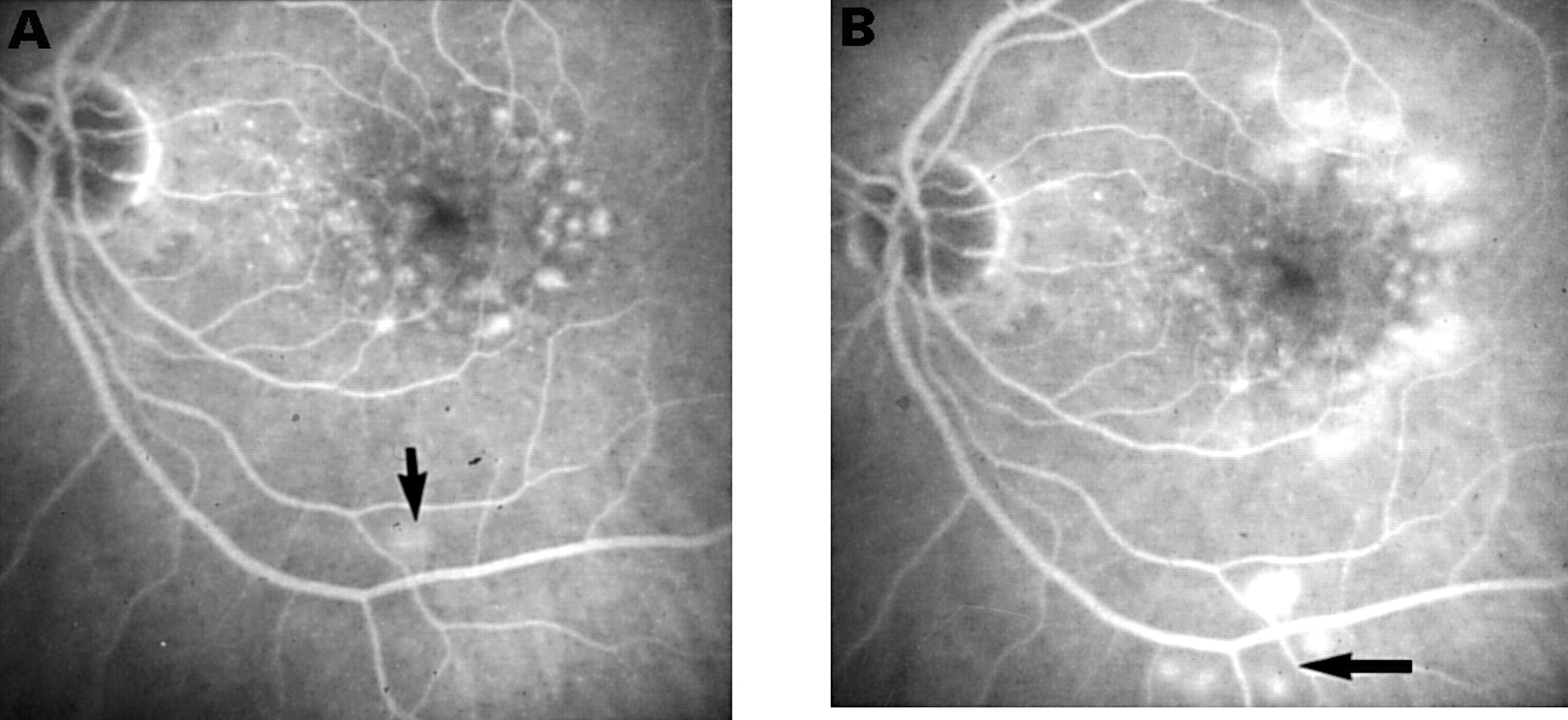
Since the energy necessary for subthreshold (RPE) photocoagulation with this laser technique was unknown, each patient received test exposures to the lower temporal arcades (see Fig 1). Two to 12 test lesions with various parameters were applied to the fundus of each patient. The different laser parameters were recorded in relation to the preoperatively performed fluorescein angiogram picture. Variation of the laser parameters included energy (30, 50, 70, 100, and 130 μJ) and number of pulses (100 or 500). Initially patients were treated by 500 pulses at 500 Hz. Since the total exposure time of 1 second turned out to interfere with occasional eye movements in some patients the total number of pulses was changed to 100 during the study. No test lesion was visible during or immediately after photocoagulation. Fluorescein angiography was performed 2 hours after test exposure. The test exposures were usually not visible 2 hours after exposure. Based on the evaluation of these test lesions the energy necessary for treating the macular pathology was chosen. The macular pathology was treated with the lowest energy, which produced RPE disruption, as evaluated by the test exposures. Energy chosen for treating the macular area, was based only on the test exposures and was not increased because of, for example, pre-RPE fluid. Central photocoagulation was performed on the same day as the test exposures were done. None of these laser burns were visible during or 2 hours after application. Table 1 shows the laser settings for laser energy and number of pulses for treating the macular pathology.

Early (A) and late (B) phase of test exposures in the lower part of the macula with various number of pulses and energy, showing RPE disruption.
Number of patients given treatment of the macular pathology with various laser settings of a Nd:YLF laser (527 nm, 160 μm, 500 Hz)
In the treatment of diabetic macular oedema photocoagulation was performed to the area of exudation as evaluated by fluorescein angiography. A total of 20–120 exposures were applied, depending on the area. In group I (diabetic macular oedema) 38.6 (22.1) laser spots were applied to the macular region. The intention was not to treat the focal point directly, as seen in angiography. In treating soft drusen, 23.16 (11.7) laser spots were applied in a 270 degree horseshoe-shaped pattern around the temporal to the foveal area. In treating CSR 6–15 laser exposures were applied around the focal point of leakage.
OUTCOME ASSESSMENT
The primary outcome in group I (diabetic macular oedema) was the change of hard exudates and the change of exudation. We compared preoperative and postoperative (6 months) fundus photographs and fluorescein angiograms. Both variables were judged as less, more, or equal. The primary outcome in group II (soft drusen) was change in number of drusen. This was qualified as less or not by comparing the fundus pictures obtained preoperatively and 6 months after treatment by subjective clinical impression. No specific morphometric analysis was performed, because the situations where changes happened were very obvious. The primary outcome in group III (central serous retinopathy) was disappearance of fluorescein exudation.
Secondary outcomes were visual acuity, infrared behaviour, and angiographic findings.
Results
We did not find any obvious difference in the clinical outcome of patients treated with 100 or 500 pulses and we therefore analysed them together.
MAIN OUTCOMES
In group I (diabetic macular oedema) six out of nine patients had hard exudates. The exudates were less after a period of 6 months (Fig2). In five out of 12 patients leakage was less as evaluated by fluorescein angiography (Fig 3). Table 2 shows the results in the group treated for diabetic macular oedema. Visual acuity in group I remained unchanged over the period investigated (preoperative: 20/20.8 (20/133) versus 20/20 (20/200) postoperative)

Fundus picture of a 48 year old diabetic patient with hard exudates (A). The corresponding fluorescein angiogram shows diffuse leakage (B). Angiogram 2 hours after a grid and a focal treatment to the area of hard exudates was performed (C). Fundus image 6 months after photocoagulation (D). Apart from two areas of hyperpigmentation (arrows) no laser scars can be seen.

Late phase (10 minutes) of a diabetic patient showing clinically significant exudation before treatment (A). The corresponding angiogram 1 day after treatment (B) shows RPE disruption due to the laser effects. Early (C) and late (D) phase of the angiogram 6 months later: no exudation is detectable in the late phase (10 minutes) (D), however microaneurysms are still visible.
Leakage and hard exudates in diabetic macular oedema after treatment with subthreshold (RPE) laser exposure
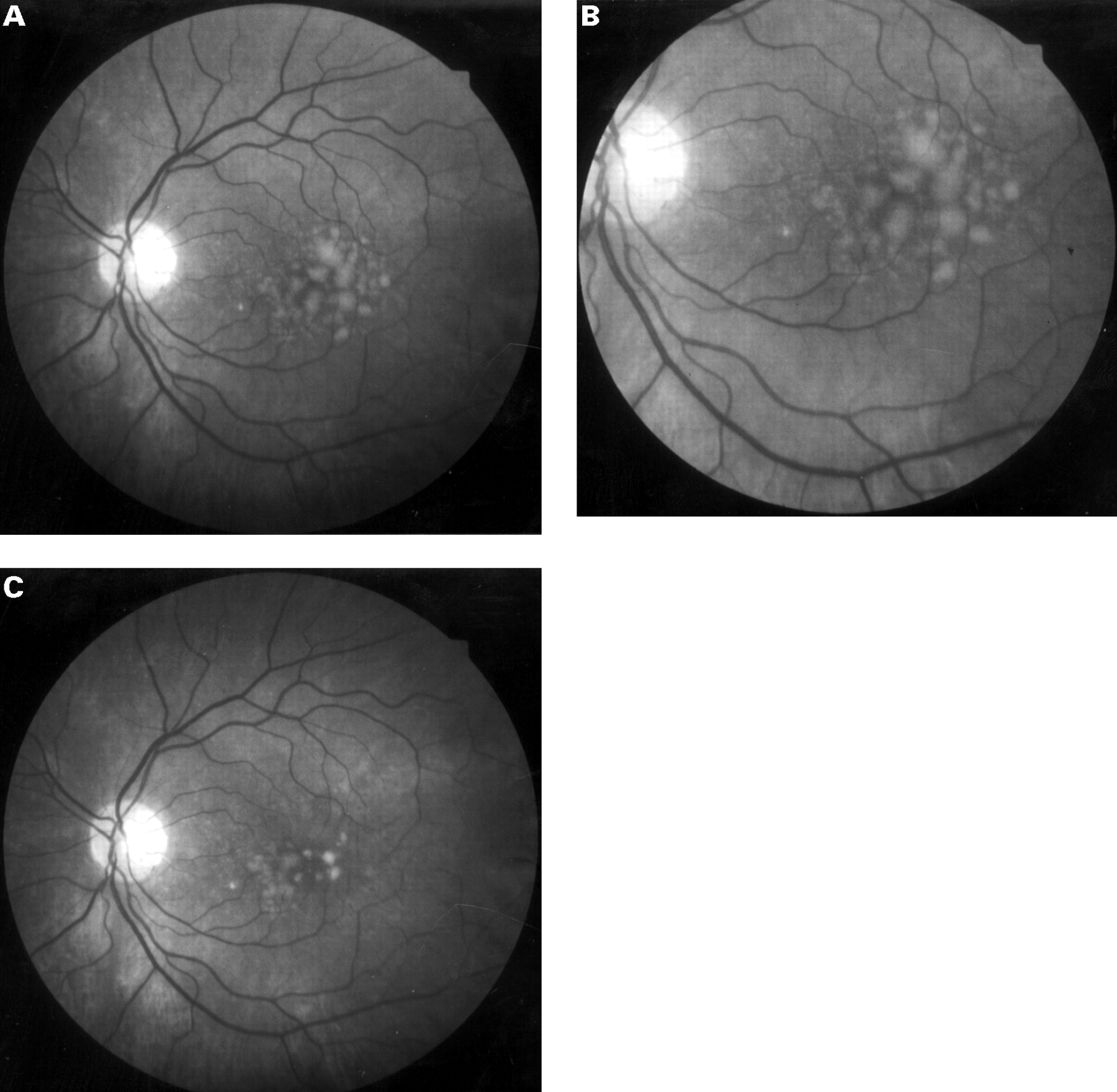
In group II the drusen disappeared in three of 10 eyes (see Figs 4 and5). In these patients (one patient with bilateral drusen) a change in drusen appearance could be detected 3 months after treatment and became obvious after 6 months. Visual acuity remained stable over the period investigated (preoperative: 20/28.2 (20/71.4) versus 20/26.7 (20/60) postoperative). In two of the three patients, where drusen disappeared, improvement in visual acuity coincided with the disappearance of the drusen. In the first patient visual acuity increased from 20/28 to 20/22 and in the second one from 20/40 to 20/28. The third patient had already an initial visual acuity of 25/20 which remained unchanged over a period of 1 year. In one patient, where drusen did not change over a period of 1 year, a hyperfluorescent, localised exudation was noted after 1 year. This exudation was classified as occult choroidal neovascularisation (CNV). It was not related to any laser site, as evaluation of fluorescein angiography showed.

Fundus image of a patient with soft drusen before (A) and 2 hours after a grid treatment has been applied to the temporal macula (B). Fundus image 1 year after treatment (C). Most drusen have disappeared. The photocoagulation pattern is shown in Figure 7B, visible as bright hyperfluorescent areas due to disruption of the outer blood-retinal barrier.

Fundus image before (A) and 6 months after subthreshold RPE treatment (B). A change in the drusen pattern is notable (arrows).
In group III (CSR), leakage disappeared promptly within 3 weeks in two out of four cases (Fig 6), delayed in one, and none in the last case. Table 3 shows the clinical characteristics before and after photocoagulation.

Fundus image of a patient with recurrent central serous retinopathy before (A) and 2 weeks (B) after photocoagulation Corresponding fluorescein angiogram before (C), 2 hours (D), and 2 weeks (E) after photocoagulation. Exudation has disappeared after 2 weeks. Note laser scars (arrow) of previously done conventional treatment.
Disappearance of exudation in central serous retinopathy after treatment with subthreshold (RPE) laser exposure
SIDE OUTCOMES
Ophthalmoscopy
No laser lesions were detectable by biomicroscopy during or immediately after photocoagulation. After 1 day the laser lesions appeared as yellow sites, similar in appearance to drusen. After a period longer than 4 weeks, most lesions were regularly undetectable by ophthalmoscopy or biomicroscopy. Occasionally some laser lesions were seen as hyperpigmented areas (see Fig 2D).
Angiography
None of the laser lesions, either test lesions or therapeutic lesions, were visible by ophthalmoscopy and biomicroscopy during or immediately after RPE photocoagulation. There were laser exposures which did not produce RPE disruption. RPE disruption was defined as a bright hyperfluorescence 2 hours after laser photocoagulation. Laser lesions were detectable only by fluorescein angiography. In group I (diabetes) 31.1 (8) out of 38.58 (22.31) laser exposures applied to the macular pathology did show RPE disruption. In group II (drusen), 20.3 (10.8) of 23.16 (11.74) lesions showed RPE disruption 1 day after laser treatment. Occasionally we observed laser test lesions which showed no RPE disruption by angiography after 2 hours, but 4 hours after laser exposure there was a disruption (Fig 7). In 25 of 26 patients the disrupted RPE barrier was re-established after 1 week. The only patient in whom the RPE barrier was not restored after 1 week was an 81 year old woman with drusen. The RPE barrier was re-established after 4 weeks. After 1 week or more the fluorescence pattern of most laser lesions in group I and II took a ring pattern. Laser lesions in group III (CSR) did not show this ring pattern. Most were undetectable for weeks after photocoagulation although a few showed slight RPE mottling.
Fluorescein angiogram 2 hours (A) and 4 hours (B) after photocoagulation. Test exposures (parameters: 500 pulses each 70 μJ and 100 pulses each 70 μJ) have been applied to the test area. While 2 hours after treatment (A) one laser exposure (parameter: 500 pulses, 70 μJ) is visible (arrow), 4 hours after treatment (B) all four laser exposures have led to disruption of the RPE barrier (arrow).
In the follow up period ICG was performed only in group II to rule out any choroidal neovascularisation. No additional information was obtained by ICG angiography. By ICG angiography the laser lesions appeared slightly hyperfluorescent in the late phase as long as the there was RPE disruption (< 1 week) and they appeared as a dark homogeneous blockage of ICG fluorescence as soon as the RPE barrier was re-established.
INFRARED IMAGING
All laser lesions were undetectable by infrared imaging immediately and after 1 day in groups I, II, and III. The laser lesions appeared as bright hyperreflective sites in some cases after 1 week and nearly always after a period of 4 weeks in group I and II (Fig8).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Fundus image of a patient treated for soft drusen 6 months after treatment (A). The photocoagulation pattern is shown in (B). Corresponding infrared images 1 day (C) and 1 week (D) after treatment. While no laser lesions are visible after 1 day all laser exposures can be visualised after 1 week (D).
Discussion
The value of conventional laser photocoagulation is well established for a variety of retinal diseases. Despite the different nature of the various underlying diseases the treatment regime remains fundamentally the same. In nearly all cases a more or less visible laser burn is applied to the retina. After photocoagulation this treatment leads to photoreceptor destruction.1-5 Based on our experimental data on rabbits, which showed that the RPE can be selectively photocoagulated by using repetitive μs laser pulses,12 we started this pilot study. The clinical findings in this study confirm the subtle nature of subthreshold (RPE) photocoagulation and show that these laser burns are different from the standard laser photocoagulation regime. All laser exposures, which produced RPE disruption, were detectable only by fluorescein angiography and were not visible by ophthalmoscopy during or 2 hours after photocoagulation. This finding is similar to that found in experimental studies.12 Ophthalmoscopic visibility of a white laser lesion always means a change in scattering properties of the retina because of tissue coagulation of photoreceptors. Individual dosimetry at the lower arcades showed that energies used for treating the diseased area were at the threshold of RPE damage. Whether the energies used for central photocoagulation were really at threshold can be deduced only indirectly. Since the macula is slightly more susceptible than the periphery, laser lesions to the macula could be slightly suprathreshold.16 However, the difference would be balanced by the pre-RPE fluid in diabetic macular oedema and CSR. The difference in the number of laser exposures applied to the central pathology and the number of lesions, which finally produced RPE disruption (group I: 38 v 31 and group II: 23 v 20) may reflect the fact that the laser exposures were at the threshold of RPE disruption in the central part, too. In some cases, the results indicated that the energy chosen was so subtle that the RPE barrier was broken up only after 4 hours, but not after 2 hours.
The main results of this prospective pilot study after a period of 6 months indicate that subthreshold (RPE) photocoagulation is sufficient and effective in some cases. In 50% of the patients suffering from diabetic macular oedema this treatment led to a reduction of leakage and to a disappearance of hard exudates. In three out of 10 patients soft drusen disappeared and in three out of four patients with central serous retinopathy this treatment regime led to a disappearance of the leakage point. These results suggest the mechanism to be an indirect RPE related effect. It also indicates that conventional laser strategies, which recommend visible laser burns (for example, Early Treatment Diabetic Retinopathy Study Research Group17), grossly overtreat in macular diseases.
There are two mechanisms suggesting how the RPE reacts to laser photocoagulation and how the therapeutic effects can be explained—one way could be that that the RPE cells at the edge of the lasered site react by spreading and migrating; this has also been shown in organ culture.18 19 Other studies have described RPE cells mitosis as a mechanism of replenishing the RPE after conventional CW photocoagulation.4 5 20 It is known that even with conventional argon laser photocoagulation, microaneurysms in diabetic maculopathy are not directly be influenced, because the laser power is far too low to occlude them directly. Marshall et al showed cell division in retinal endothelium cells after photocoagulation remote to the lasered site, suggesting an indirect effect of laser photocoagulation.9 Drusen are located beneath the RPE and Bruch's membrane, which is the primary target of our photocoagulation technique. The mechanism by which drusen disappear is unclear. In our three patients the disappearance of drusen occurred far away from the lasered sites, suggesting that direct photocoagulation is not necessary. After selective RPE photocoagulation in rabbits it has been shown that the RPE is reacting in a wide area around the lasered site.12 A similar effect seems to prevail in the treatment of central serous retinopathy. In none of the patients treated for CSR was the focal point of leakage treated directly, only indirectly by applying a few laser shots in the immediate neighbourhood around the focal point of exudation.
The value of this photocoagulation technique needs to be clarified in a controlled clinical study comparing subthreshold RPE photocoagulation with conventional photocoagulation. The main problems of this photocoagulation technique are related to dosimetry. Unclear variables are appropriate laser energy, necessary number of laser burns, and individual RPE reaction. Owing to the subtle nature of this photocoagulation technique these lesions are only visible by fluorescein angiography immediate after treatment, and not by ophthalmoscopy or infrared imaging. Unless active feedback mechanisms like, for example, the detection of the RPE autofluorescence21 are available, dosimetry is cumbersome and requires an additional fluorescein injection. Owing to the subtle nature of this photocoagulation technique it remains unclear how many laser burns are necessary in a given situation. It seems reasonable to assume that the number of laser burns necessary for achieving a therapeutic effect could be different between conventional photocoagulation techniques and extremely mild (RPE) subthreshold laser effects. Since tissue response with conventional photocoagulation techniques is more pronounced because of the larger magnitude of the cellular response, it could be that more laser burns are necessary with subthreshold (RPE) effects. In the treatment of drusen with subthreshold diode laser burns, which seem to spare mostly the inner nuclear layer and the nerve fibre layer, it takes a significantly longer time for drusen to resolve compared with standard treatment modalities.22 If this technique works on the level of RPE, attention should be drawn to the fact that RPE reaction could be different in different individuals. The infrared findings in our study are consistent with these ideas. The detection of the laser lesions after 1 week by infrared imaging goes along with the restoration of the RPE barrier. It is, however, worthwhile noting that the laser lesions can usually not be detected by infrared imaging in group III. Group III (CSR) is a population which has a significant lower age (mean age 44 years) compared with the other groups (mean age 59.7 years). One explanation could be that the RPE has reacted by spreading in those patients where the lesions can detected by infrared imaging. Since the melanin content in these cell extensions is lower more reflected infrared light can penetrate the newly formed RPE layer. It has been shown histologically in older patients that a thin cellular layer of RPE cells exists after conventional laser photocoagulation.23 In the younger group (CSR) the RPE could be still capable of cell division. Newly formed RPE cells should have a normal melanin content and the reflected light should appear normal when compared with the other cells.
Independent of the potential problems of this laser technique, the clinical findings in this study show that in some diseases it is not always necessary to produce retinal blanching and destroying the photoreceptors in order to achieve a therapeutic effect. If the therapeutic effect is a RPE effect this photocoagulation technique would avoid localised scotoma and would allow retreatment. Future experimental and controlled clinical studies are needed to clarify the value of this type of photocoagulation.
Acknowledgments
Presented in part as a poster at the Annual Meeting of the American Academy of Ophthalmology, San Francisco, 1997.
Commercial interest: One of the authors (RB) has a patent on the laser technique used in this study.