Article Text

Abstract
Background/aim: The combination of chemotherapy and transpupillary thermotherapy, thermochemotherapy (TCT) has become an established part of the treatment plan in advanced retinoblastoma. The aim of this study was to identify safe indications, the complications as well as the limitations of this new treatment for retinoblastoma.
Methods: Tumour response and side effects of TCT with an indirect laser ophthalmoscope (spot size about 400 μm) in 55 tumours of 26 children with bilateral retinoblastoma were analysed. Using the Reese-Ellsworth classification system, nine of 35 eyes were classified as type I, 13 eyes as type II, 10 eyes as type III, and three eyes as type V. The mean age of the children was 0.74 (SD 0.61) years. The mean tumour height was 3.5 (2.3) mm with a mean diameter of 6.1 (4.1) mm. Treatment parameters were 4.3 (1.6) (median 5) thermochemotherapy sessions with a mean energy of 539 (211) mW and a mean duration of 13.5 (5.6) minutes. Chemotherapy courses (vincristine, etoposide, and carboplatin) were repeated every 3 weeks. The mean follow up period was 1.25 (0.6) years.
Results: Local recurrence occurred in 21 tumours (38%), with a mean onset of 3.2 (2.9) months after TCT. The risk of tumour recurrence was correlated with tumour height. The recurrence rate was 17% for tumours with a height less than 2 mm, 37% for tumours with a height between 2 and 4 mm, and 63% for larger retinoblastomas. Multivariate analysis identified fish flesh regression after TCT (p = 0.0007) as the most important risk factor for tumour recurrence besides tumour height (p = 0.001) and the necessity of increased laser power during TCT sessions (p = 0.018). Complications during therapy included transient corneal opacification in two eyes (6%), focal iris atrophy (three eyes, 8.5%), peripheral lens opacity (two eyes, 6%), circumscribed transient retinal detachment (one eye, 3%) and diffuse choroidal atrophy (one eye, 3%).
Conclusion: TCT using an indirect laser ophthalmoscope with a spot size of about 400 μm was efficient for retinoblastoma with a tumour height less than 4 mm. In larger tumours, the recurrence rate was unacceptably high. Fish flesh regression after TCT correlates with a higher rate of local tumour recurrence. Treatment related complications occurred in less than 9% of the treated eyes.
- retinoblastoma
- chemotherapy
- hyperthermia
- laser coagulation
Statistics from Altmetric.com
Treatment of advanced bilateral retinoblastoma has changed during the past 10 years. A decade ago external beam radiotherapy (EBR) was part of the standard strategy in the treatment of this hereditary disease. Publications in the early 1990s showed an increased risk for non-ocular malignancies after EBR in retinoblastoma patients with a germline mutation. This cumulative risk for secondary cancers was estimated to be 35% until the age of 30 years, and presumably higher if EBR was performed during the first year of life.1–4 As a consequence of this threatening long term complication, new treatment strategies for advanced bilateral retinoblastoma were developed.
Possible alternatives include intensified use of local treatments such as cryotherapy, laser coagulation, or brachytherapy with low energy γ or β ray plaques. Owing to limitations of these treatments, however, EBR could not be replaced in advanced disease.5–8 Chemotherapy had been an established treatment for extraocular extension of retinoblastoma,9 although a significant effect of systemic chemotherapy on intraocular retinoblastoma was observed.10–13 Chemotherapy alone, however, does not lead to complete destruction of intraocular retinoblastoma.14 Only the combination of systemic chemotherapy with local treatments such as laser or cryocoagulation or brachytherapy results in acceptable local tumour control rates.10,12,15 Another variation of a combined treatments is thermochemotherapy (TCT)—that is, the combination of chemotherapy with local tumour hyperthermia. The amplification of the cytotoxic effect of platinum analogues was demonstrated in cell lines,16,17 and in phase I/II studies in retinoblastoma.12,18 A transpupillary infrared diode laser system can be used to selectively increase the temperature in the tumour, with the intention of avoiding adverse side effects in surrounding normal ocular tissues. Transpupillary thermotherapy is normally used for the treatment of tumours at the posterior pole of the eye. Treatment of tumours in the periphery of the retina may produce an increased rate of severe thermal side effects in the anterior segment of the eye. During treatment of anterior tumours in the eye the effective diameter of the pupil is reduced by the consequential angle between the laser beam and the optic axis of the eye. If the laser beam hits the iris there is a consecutive increased risk for thermal effects in the iris resulting in iris burns and focal lens opacifications with subsequent visual impairment
New approaches with trans-scleral application are currently the subject of investigation and may avoid these side effects.19,20 The first clinical results of thermotherapy and TCT are encouraging.20,21
Since May 1997 we have treated advanced intraocular retinoblastoma with systemic chemotherapy and selected tumours in the affected eyes were treated in combination with local hyperthermia. The purpose of this retrospective study was to identify safe indications, complications, and limitations of the new treatments.
PATIENTS AND METHODS
The treatment of the patients was performed in two medical centres by the same ophthalmologists. The indications for treatment, the chemotherapy protocol, the local treatment modalities, the additional local and systemic treatment, as well as the follow up examinations during and after the end of the systemic therapy were identical in both centres. Data were collected in a single computer database.
The indication for thermochemotherapy was an untreated retinoblastoma posterior to the equator in children with bilateral retinoblastoma. We included small juxtapapillary, juxtamacular, or submacular retinoblastoma, and large retinoblastoma at the posterior pole where massive visual impairment was expected after single local treatment with laser coagulation or brachytherapy. In cases with an exudative retinal detachment, chemotherapy was initially given to reduce the tumour size followed by thermochemotherapy after the subretinal fluid had resolved.22 Twenty four tumours of 12 children (14 eyes) received this initial chemoreduction. The treatment protocol for initial chemoreduction is listed in Table 1. In these cases, the mean number of chemoreduction cycles before the start of thermochemotherapy was 2.6 (SD 1.2, median 2.5; range 1–5). No other treatments were used before thermotherapy in the 55 evaluated tumours. Tumours in the periphery of the retina not eligible for thermotherapy were treated either by cryotherapy or laser coagulation or by β ray brachytherapy, depending on their location and size. Exclusion criteria for this study were unilateral sporadic disease, functional blindness, tumour infiltration of the optic disc, or tumour extension into the anterior segment of the eye.
Chemotherapy regimen used in 14 patients for chemoreduction. Regimen was repeated after course 3
Thermochemotherapy was performed in all cases after extensive mydriasis within 2 hours after the end of the infusion of carboplatin under general anaesthesia. The chemotherapy protocol used for TCT is listed in Table 2. In all cases an indirect ophthalmoscope attached to an infrared diode laser was used for hyperthermia. A laser from Iris Medical (Iris Medical OcuLight Slx, Iris Medical Instruments Inc, CA, USA) was used in the centre in Essen; in the other centre a diode laser manufactured by Zeiss (Visulas Diode II, Zeiss Oberkochen, Germany). Owing to the indirect delivery system in combination with a 20 D lens, the spot size was about 400 μm. The aiming beam of the laser was focused on the surface in the centre of the tumour during the whole treatment session. To reduce the complication rate in the anterior segment, a protective contact lens, which covered the periphery of the cornea and iris allowing laser treatment through the optic centre of the eye, was used. In small tumours, the laser energy was adjusted to achieve a just visible grey-white discoloration of the tumour at the end of the treatment session. Following published recommendations treatment started with 400–500 mW in tumours with a height of about 4 mm, and 500–700 mW for larger retinoblastomas.12 In cases without a visible effect after the first minutes of treatment, the laser power was increased until a slight discoloration of the tumour at the end of the TCT session was achieved. The planned duration of treatment varied between 10 minutes for small tumours and approximately 20 minutes for larger tumours. The patients were examined under general anaesthesia every 3 weeks during the treatment period. End point for chemotherapy was a complete tumour regression. Following completion of systemic treatment, the children were re-examined every 3–6 weeks.
Chemotherapy regimen used for TCT
Between May 1997 and November 1999, 26 children (15 boys, 11 girls) with newly diagnosed bilateral retinoblastoma were treated with TCT. Clinical parameters regarding the treated tumours and the treatment parameters are listed in Table 3. In 17 eyes of the 26 children complete tumour control was achieved either by local therapy or by enucleation. Thermochemotherapy was used for the treatment of 55 retinoblastoma in 35 eyes. Using the Reese-Ellsworth classification system, nine eyes (26%) were classified as type I, 13 eyes (37%) as type II, 10 eyes (29%) as type III, and three eyes (8%) as type V. The 67 other tumours in these 35 eyes were treated either using laser coagulation and cryotherapy (n=64) or ruthenium-106 brachytherapy (n=3, representing cases with mid-sized retinoblastoma in the periphery of the retina).
Tumour size and location before treatment and treatment parameters used during TCT. The mean total energy was calculated as sum of laser power and duration of treatment. Initial tumour volume was calculated as a cone shaped model based on tumour diameter and height before TCT
TCT was repeated every 3 weeks. The children received between three and 14 courses of chemotherapy. The clinical variables, tumour parameters and treatment parameters during and after the end of systemic treatment were documented in a single computer database. Every tumour treated by TCT was handled as a single observation in the database.
Statistical analysis was performed using the sas system for multivariate analysis and JMP statistical package for descriptive and univariate statistics. In multivariate statistics end point for Cox proportional hazard analysis was local tumour recurrence after TCT or enucleation respectively external beam radiotherapy of the eye. Univariate statistical analysis was performed using Wilcoxon ranked pair test for continuous parameters and contingency table with χ2 test for nominal parameters. The continuous and discrete clinical variables were tested as predictors for complete tumour destruction after TCT using a multivariate model. For parts of univariate statistical testing the treated tumours were divided in groups depending on initial tumour height (tumour height less than 2 mm, between 2 and 4 mm, and more than 4 mm) respectively in groups with or without local tumour recurrence.
Some analysed parameters were calculated based on ultrasound measurements and documented laser settings. The total energy used for the treatment of the tumours was calculated as the sum of the product of laser power and duration of the treatment sessions in the individual tumour. In addition, a hypothetical cone-shaped tumour volume based on the initial mean diameter and the initial tumour height was calculated using the formula: volume = (mean diameter × tumour height × ∂)/3. Based on these parameters the relative applied energy per mm3 tumour volume was calculated by dividing the calculated total energy applied to the tumour during all treatment sessions by the initial tumour volume.
RESULTS
Treatment parameters like mean number of thermochemotherapy sessions, mean duration of the treatment sessions, mean cumulative duration, and laser power used during TCT are listed in Table 3. The mean total energy used for the treatment and the mean relative energy per tumour volume was calculated (Table 3).
The treatment parameters for three groups of retinoblastoma with a tumour height less or equal to 2 mm, between 2 and 4 mm, and for tumours larger than 4 mm are listed in Table 4. The number of TCT session was smaller for tumours with a height less than 2 mm, but there was no significant difference between the groups with larger retinoblastoma tumours. The laser power, total duration of TCT, as well as the applied energy during the whole TCT was tiered for larger tumours. The calculated mean relative energy per tumour volume was significantly smaller for larger retinoblastoma (Table 4).
Therapy parameter as a function of tumour height. (Values are mean (SD))
To achieve complete tumour regression, one session of TCT was required in one tumour, two sessions in 11 tumours, three sessions in seven tumours, four sessions in seven tumours, five sessions in 10 tumours, and six sessions in 19 tumours. The regression patterns of the retinoblastomas after TCT were comparable with those observed after external beam radiotherapy like cottage cheese appearance (type I), fish flesh appearance (type II), or a mixture of these two regression types (type III). At the end of thermochemotherapy, 16 tumours showed a type III regression (29%), one tumour a type II regression (2%), 15 tumours a type I regression (27%), and 21 tumours disappeared and showed a flat scar (38%) (Figs 1 and 2). Two tumours did not demonstrate any typical regression (4%).

Hereditary juxtapapillary retinoblastoma with a tumour height of 2.4 mm and a diameter of 4.5 mm in a 3 week old girl. The tumour is beside the optic disc and fovea.
Same eye as in Figure 1 after five courses of TCT. Complete tumour regression with fibrotic remnants in the scar without optic nerve atrophy.
The complications induced by local laser treatment included transient corneal opacification in two eyes (6%), focal iris atrophy in three eyes (8.5%), and peripheral focal lens opacification in two eyes (6%). Complications in the posterior segment were a transient circumscribed retinal detachment in one eye (3%) and in one case a massive choroidal necrosis after the second course of thermochemotherapy (3%). There were no cases with clinically significant epiretinal gliosis, persistent occlusion of retinal vessels, vitreous haemorrhage, or the development of a vitreous seeding during or after TCT. The development of small haemorrhages within the tumour during thermotherapy was considered to be a treatment effect.
The mean follow up period was 1.6 (0.6) years after the first presentation of the children and 1.25 (0.6) years (range 1 month to 2.3 years) after cessation of thermochemotherapy. A local tumour recurrence after TCT occurred in 21 tumours (38%) in 16 eyes of 15 children (Figs 3 and 4). The mean interval between the end of TCT and the diagnosis of tumour recurrence was 3.2 (2.9) months (median 2.6 months; range 1 week to 12 months).

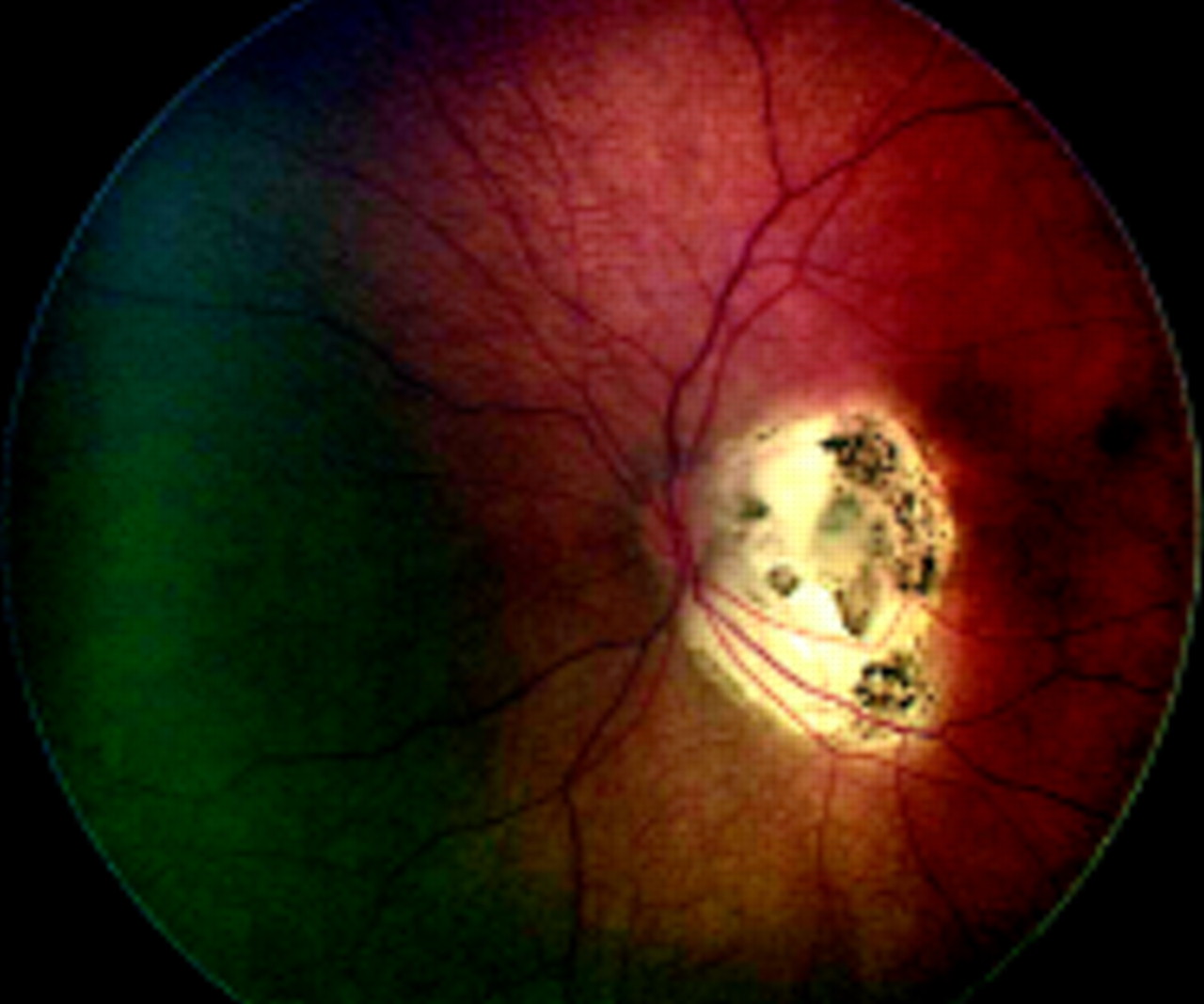
Finding in a 10 months old girl 5 months after four courses of TCT. Tumour recurrence started in the unpigmented part of the scar. Complete regression occurred after additional diode green laser coagulation.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Finding 4 months after six courses of TCT (initial tumour height 5.7 mm). Typical occurrence of tumour relapse at the border and at the apex of the remnants with fish flesh regression. Additional −106 ruthenium brachytherapy achieved complete cottage cheese regression.
Recurrences at the margins of the tumour remnants were initially treated with laser coagulation in 17 cases. Brachytherapy with β ray plaques was performed in 14 tumours in 12 eyes. Indications for the latter therapy included massive recurrence or local recurrence at the apex of a tumour remnant, which was not suitable for laser coagulation. External beam radiotherapy was used in four eyes (two children) to treat multifocal recurrent subretinal seeds or reactivation of vitreous seeding in eyes with a good visual prognosis. After additional treatment complete tumour regression was observed in nearly all retinoblastomas initially treated with TCT. Enucleation was indicated in two eyes with a massive tumour recurrence in virtually blind eyes. None of the children developed metastatic disease during the follow up period.
Univariate statistical analysis was performed to find significant differences between the groups with and without tumour recurrence. The results are listed in Table 5. The group with recurrence showed a significantly larger tumour diameter and tumour height, while the distance between the tumour and the optic disc, the age of the children or the number of tumours at the beginning of TCT did not have any statistical effect on tumour recurrence. Further treatment parameters such as the number of TCT sessions or the total duration of the treatment did not influence tumour recurrence. The mean laser power and the mean total energy used during the TCT sessions as well as the mean energy per tumour volume showed significantly larger values in the group with tumour recurrence. The majority of recurrent tumours showed an initial tumour height of more than 2 mm, only four tumours with recurrence were smaller than 2 mm. If statistical analysis was performed selectively for tumours with a height of more than 2 mm, the mean relative energy per tumour volume showed a significant smaller value than in the group without recurrence (Table 5).
Differences between tumours with and without local recurrence after TCT. (Values are mean (SD))
Statistically significant parameters predicting tumour recurrence according to the multivariate analysis using Cox proportional hazard included fish flesh regression pattern at the end of thermochemotherapy (risk ratio 4.88, p = 0.0007) and greater tumour height (risk ratio 1.36, p = 0.0009). Treatment related parameters identified were an increasing treatment power (risk ratio = 1.004, p = 0.018) and increasing cumulative energy per tumour volume (risk ratio = 1.001, p = 0.0001). Parameters which did not show any significant effect in multivariate analysis were initial calcification in the tumour (p = 0.38); initial retinal detachment (p = 0.22); total number of tumours at the commencement of TCT (p = 0.94); tumour distance to the optic disc (p = 0.42); diameter of the treated tumour (p = 0.96); age at the beginning of TCT (p = 0.22); chemoreduction before TCT (p = 0.82); number of TCT sessions (p = 0.86); and total duration of the TCT (p = 0.31). We did not perform a multivariate analysis for the end point enucleation, as only two eyes were lost and their loss was not the result of treatment with TCT.
DISCUSSION
The concept of additional tumour hyperthermia to increase the toxicity of chemotherapeutic agents to tumour cells is an accepted treatment option in oncology. Initial attempts by Lagendijk to use a microwave device to increase the temperature in the eye has found little clinical acceptance to date.23,24 The availability and application of infrared diode lasers in ophthalmology was a precondition for the use of the “hyperthermia concept” in the treatment of intraocular tumours. The actual disadvantage of this technique is the limitation to tumours at the posterior pole. DNA bound carboplatin showed significant therapeutic levels 2.5 and 5 hours after intravenous administration of 560 mg/m2 of carboplatin for human retinoblastoma. Further, increased levels of DNA bound carboplatin were observed after additional hyperthermia in a rabbit model with hamster derived non-pigmented green melanoma cells.12 The additive effect of hyperthermia and chemotherapy with carboplatin in murine retinoblastoma cells was investigated by Murray et al.17 These authors showed thermal enhancement ratios between 1.1 and 25.8, dependent on temperature level and exposure time.17 The results of first clinical trials of TCT in retinoblastoma are promising. Based on a three drug chemotherapy (carboplatin, etoposide, vincristine), Murphree reported a success rate of 100% in retinoblastoma of less than 8 disc diameters.12 Local recurrence was observed by Levy et al in nine of 15 retinoblastomas with a diameter between 1.5 and 10 mm after TCT based on a two drug chemotherapy (carboplatin, etoposide).21 In a study on thermotherapy in 188 retinoblastoma, Shields et al used thermotherapy in tumours smaller than 4 mm and TCT based on a three drug chemotherapy (vincristine, etoposide, carboplatin) in larger retinoblastomas.20 The overall tumour control rate for both groups was 85.6%.20 Other groups achieved comparable eye salvaging rates of 79% with chemoreduction and chemothermotherapy in combination with local treatment options.25 Thermochemotherapy with a carboplatin based chemotherapy regimen in combination with thermotherapy (without chemotherapy) 1 week after TCT was published by Lumbroso et al. Laser treatment in these cases was performed with a microscope delivery system that allowed laser spot sizes up to 2 mm during treatment. With a mean laser spot size of 1.2 mm TCT in combination with thermotherapy resulted in a tumour recurrence rate of about 7%.26 A clinical problem in thermotherapy and thermochemotherapy of retinoblastoma is the unknown effect of the laser treatment on the temperature in the individual tumour during the treatment session. Different chemotherapy regimens, different laser delivery systems with different spot sizes, and different treatment parameters complicated a comparison with the published studies.12,20,21
In this retrospective study, we had a very high local recurrence rate in tumours with a height of more than 2 mm. This high rate in larger tumours occurred despite longer laser exposure time and higher laser power delivered during TCT. The idea of laser energy input in a defined tumour volume appears to be a useful model to describe the physical effect of thermotherapy.
Correlation of the applied energy with the initial tumour volume showed a coincidence between massive reduced energy levels per tumour volume and local tumour recurrence (Table 4). Assumed that the total energy per tumour volume applied to the tumour during TCT may be a parameter for the incline of the temperature in the tumour, we have to conclude that this intended objective of thermotherapy was not achieved in larger tumours. A further increase in energy level and duration during TCT appears to be an obvious solution to increase the effect of thermotherapy in these tumours. Side effects such as laser absorption in the anterior segment or haemorrhage in the tumour limit the amount and duration of energy, however, which can be applied.
The laser spot size is important in thermotherapy. The diameter of the laser beam in this study was about 400 μm in emmetropic or slightly hyperopic patients. Other groups used a laser delivery system attached to a microscope.20 This device allows larger spot sizes between 800 μm and 2000 μm, which produce larger and deeper hyperthermia zones with significant temperature related tumour destruction.12,20,21,27 If the results of transpupillary thermotherapy in melanoma are applicable in retinoblastoma, the decrease of temperature around the laser area might be about 5°C per mm distance.27 Depending on the temperature within the direct laser area (during treatment unknown) and the depth of maximal light absorption in the tumour tissue, it could be supposed that tumour parts around the laser area became heated to a temperature less than the critical 45°C. The smaller the ratio between spot size and tumour size, the higher seems to be the risk of areas with insufficient incline of temperature. An argument for this theory is our observation that recurrences after TCT normally occur at the border or at the apex of the regressed tumours (Fig 4). The small spot size might be one possible explanation for the high local recurrence rate in this study, in particular in larger tumours. The reason for the four recurrent tumours in initially small sized retinoblastoma might be an insufficient absorption of infrared light in flat scars after the first session of TCT. The typical finding in these cases was a recurrence within unpigmented areas in the scar (Fig 3).
To identify risk factors after TCT, we compared the group with and without tumour recurrence. Multivariate analysis identified fish flesh regression following TCT as the most important predictor for a local recurrence (risk ratio 4.88) apart from greater tumour height and necessity of higher laser power to achieve a discoloration of the retinoblastoma during TCT. An explanation for the high risk ratio of fish flesh regression after TCT might be that viable tumour cells were judged as a fish flesh or a mixed regression type (type III).
Recurrent tumours were treated in the majority of cases by laser coagulation or β ray brachytherapy. Indications for the latter were recurrences at the apex of the regressed tumour or multifocal recurrences in the treatment area after TCT. External beam radiotherapy was necessary in four eyes of two children and was indicated by recurrent vitreous seeding or multifocal recurrent subretinal seeds in the periphery of the retina. Regular control under general anaesthesia and immediate additional local treatment allowed preserving 94% of the eyes. Only two eyes in this group had to be enucleated due to virtual blindness.
The results of this retrospective study should be judged with caution. The indication for TCT was based on the idea to bypass EBR in advanced cases. With an eye salvaging rate of 94% our results are comparable to the results published after EBR. TCT was part of a complex treatment plan including different treatments in the same eye during the same treatment period. It is not possible to exclude influences of the additional local treatment on TCT. Based on our experience, we suggest primary TCT with an indirect ophthalmoscope and a small laser spot size for juxtapapillary or juxtamacular retinoblastoma if the central margin of the tumour is very close to these critical structures. If TCT results in a partial or complete fish flesh regression, additional local treatment or, at least, regular short term follow up is recommended. In larger tumours, TCT with a small laser spot size resulted in a high recurrence rate. The decision for systemic chemotherapy with its possible short and long term side effects must be made with great hesitancy. External beam radiotherapy in bilateral retinoblastoma induced secondary non-ocular malignancies decades after treatment.1 Serious side effects of systemic chemotherapy in retinoblastoma cannot be excluded.28–30 Whenever possible, local treatment options such as laser coagulation, cryotherapy, or brachytherapy with γ ray or β ray plaques should be preferred. The larger the retinoblastoma treated by TCT with small laser spot sizes, the higher the risk for a local recurrence. Regular control under general anaesthesia after cessation of TCT and immediate local treatment of recurrent tumours result in an excellent long term tumour control rate in retinoblastoma.