Article Text

Abstract
Background: The purpose of this study was to determine the age-adjusted incidence of retinoblastoma in the USA over a 30-year period from 1975 to 2004 using a review of existing databases.
Methods: Six hundred and fifty-eight patients with retinoblastoma (International Classification of Oncology (ICDO-3) codes C69.2 (retina) and C69.9 (eye, NOS)) were derived from the Surveillance, Epidemiology, and End Results (SEER) program database in the USA from 1975 to 2004. Nine historical SEER registries were utilised. The significance of trend in age-adjusted incidence rate was determined using the χ2 test, and 95% CIs were calculated. The patients were stratified according to age at diagnosis, laterality, gender and race.
Results: There were a total of 658 cases of retinoblastoma, representing 6.1% of all childhood cancers under age 5 years. The mean age-adjusted incidence of retinoblastoma in the USA was 11.8 per million children aged 0–4 years (95% CI 10.9 to 12.8). There was no significant trend in age-adjusted incidence for all races/genders, nor was there any significant variation of incidence between races or between genders. The proportion of bilateral cases (26.7%) versus unilateral cases (71.9%) remained stable over the 30-year period.
Conclusions: The mean age-adjusted incidence rate of retinoblastoma of 11.8 cases per million children aged 0–4 years in the USA is similar to rates reported from European countries. The age-adjusted incidence rate of retinoblastoma in the USA has remained stable for the last 30 years.
Statistics from Altmetric.com
Worldwide incidence rates of retinoblastoma in children aged 0–4 years vary from a low of 3.4 per million in Bulgaria to a high of 42.5 per million in Mali.1 2 Incidence rates have been noted to vary greatly within Asia (6.3 to 19.6) and Africa (10.6 to 42.5), while incidences in Europe (six to 12) and Australia (10.3) generally show less variability. Incidences in Central and South America range from 7 per million in Uruguay to 17.1 in Colombia.1 2 A summary of published reports on incidence of retinoblastoma in the USA appears in table 1.
To our knowledge, only two prior reports have assessed short-term trends in incidence of retinoblastoma in the USA.3 4 In view of recent literature regarding the role of environmental factors in the incidence of retinoblastoma, we decided to examine the incidence of retinoblastoma over the 30-year period from 1975 to 2004 to investigate any trends that might have an environmental aetiology.
Using the Surveillance, Epidemiology and End Results (SEER) Program database of the National Cancer Institute, we analysed variations in age-adjusted incidence of patients with retinoblastoma in the USA over a 30-year period between 1975 and 2004. The SEER Program of the National Cancer Institute is the only comprehensive source of population-based information on cancer incidence and survival rate in the USA. The SEER Program collects data from population-based cancer registries and covers approximately 26% of the USA. The population covered by SEER is comparable with the general USA population. In our study, nine historical SEER registries were utilised, as these were the only registries collecting data for the entire 1975–2004 period. These registries cover approximately 9.5% of the USA population.5
MATERIALS AND METHODS
The National Cancer Institute SEER Public Use CD-ROM for the period 1973–2004 was used.6 Nine historical SEER registries were utilised. For both morphology (retinoblastoma = 9510–9513) and topography (retinoblastoma included retina and eye (C69.2, C69.9)), International Classification of Oncology (ICDO-3) codes were utilised to define the cases for the study.7 The patients were stratified according to age at diagnosis, laterality, gender and race. Incidence rates were calculated per 1 000 000 and age-adjusted to the 2000 US Standard Population (single ages—Census P25-1130) standard; CIs are 95% for rates and trends. Percentage changes were calculated using 2 years for each end point; annual percentage changes (APCs) were calculated using the weighted least-squares method.8
RESULTS
There were 658 cases of retinoblastoma in the file for the 30-year period (table 2).
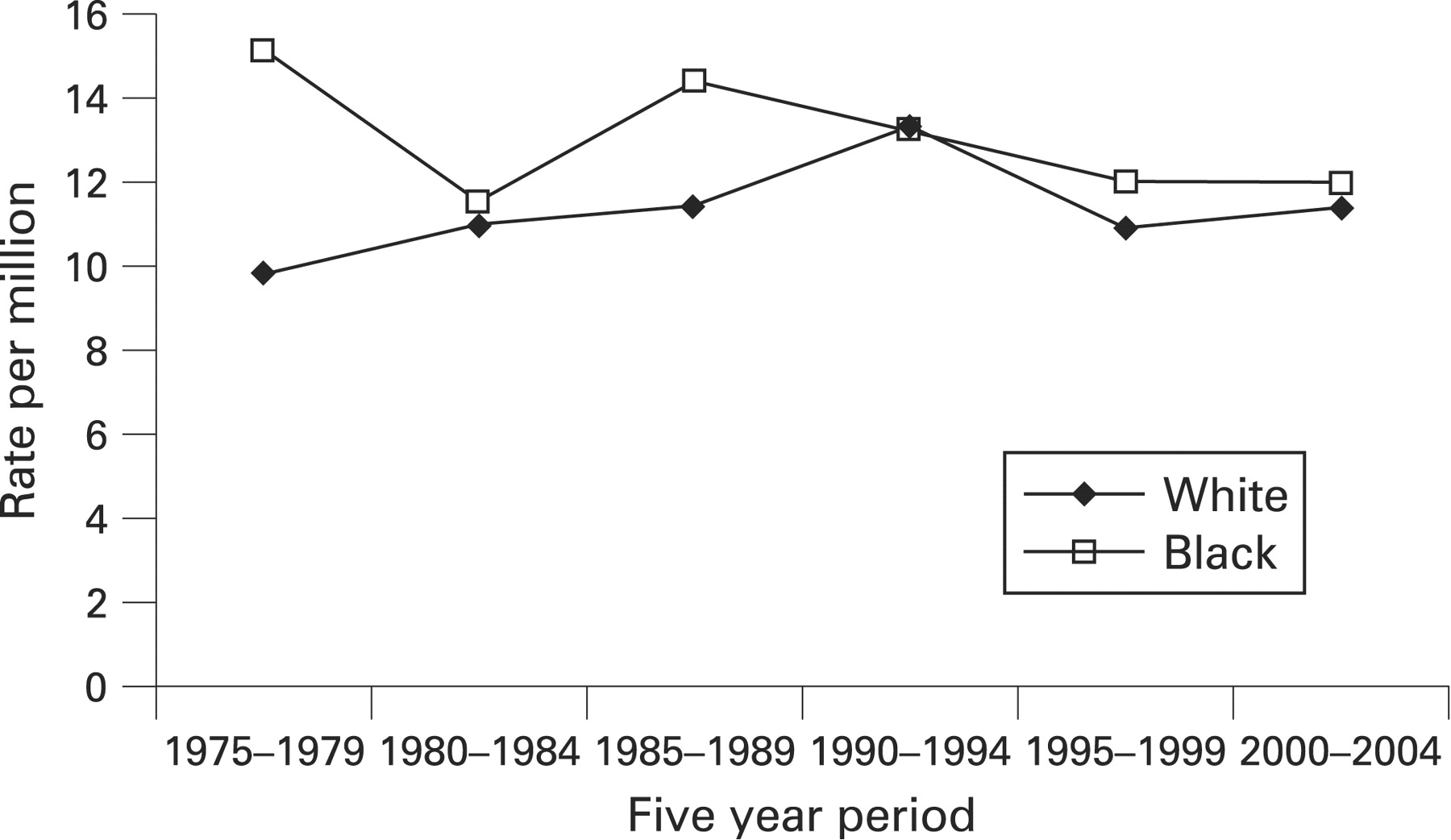
The overall mean age-adjusted incidence of retinoblastoma was 11.8 per million children aged 0–4 years (95% CI 10.9 to 12.8). When examined by gender, the overall mean age-adjusted incidence was 11.3 (95% CI 10.1 to 12.7) for males and 12.4 (95% CI 11.1 to 13.8) for females. When examined by race, the overall mean age-adjusted incidence was 11.3 for Caucasians and 13.0 for black individuals. There was no significant difference in incidence of retinoblastoma between Caucasians and black individuals for any of the 5-year time intervals (fig 1).

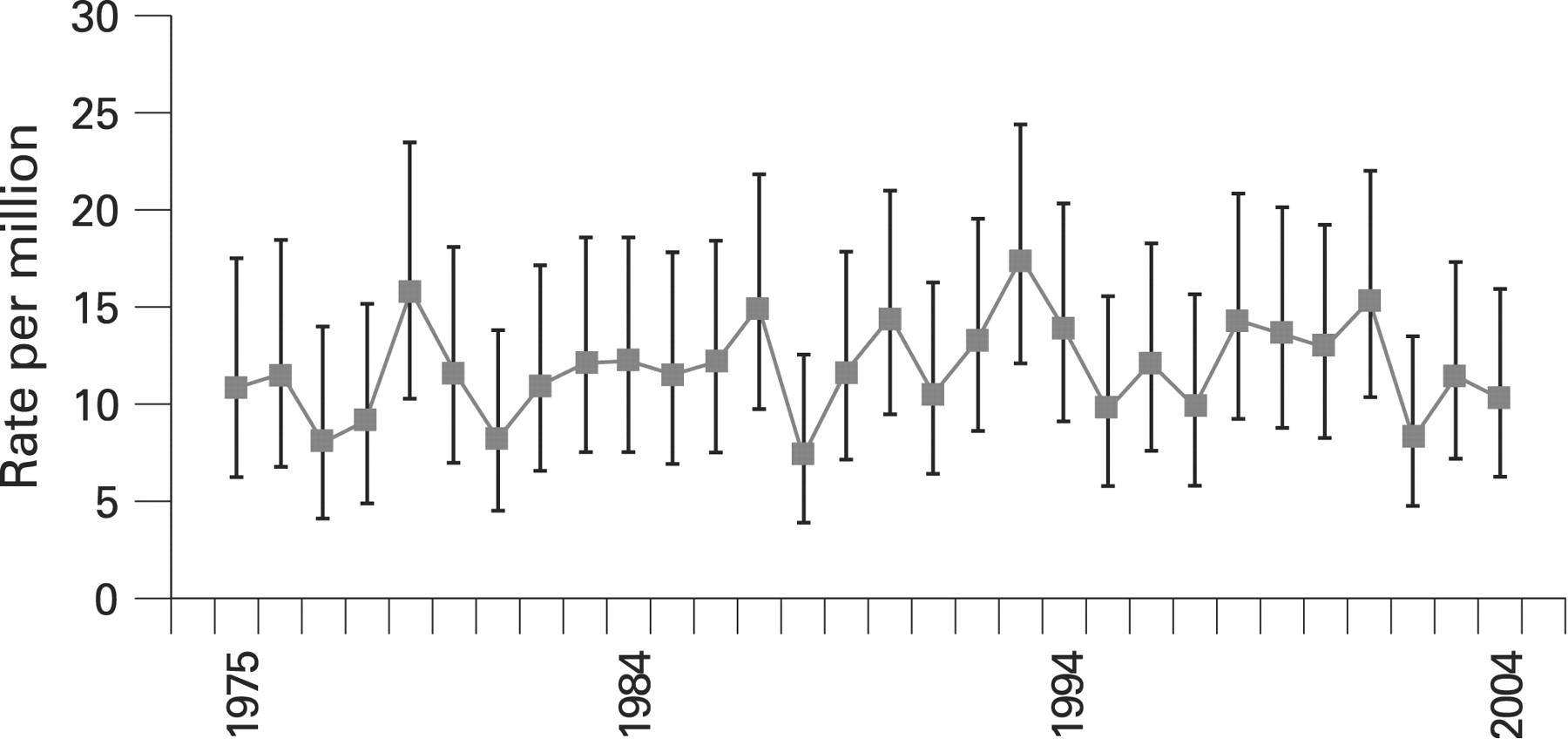
The overall incidence rate of retinoblastoma did not vary significantly between 1975 and 2004 (fig 2). There is no notable trend in incidence over the 30-year period when analysed by the least-squares method. In addition, there was no significant variation between genders or between races over the 30-year period.

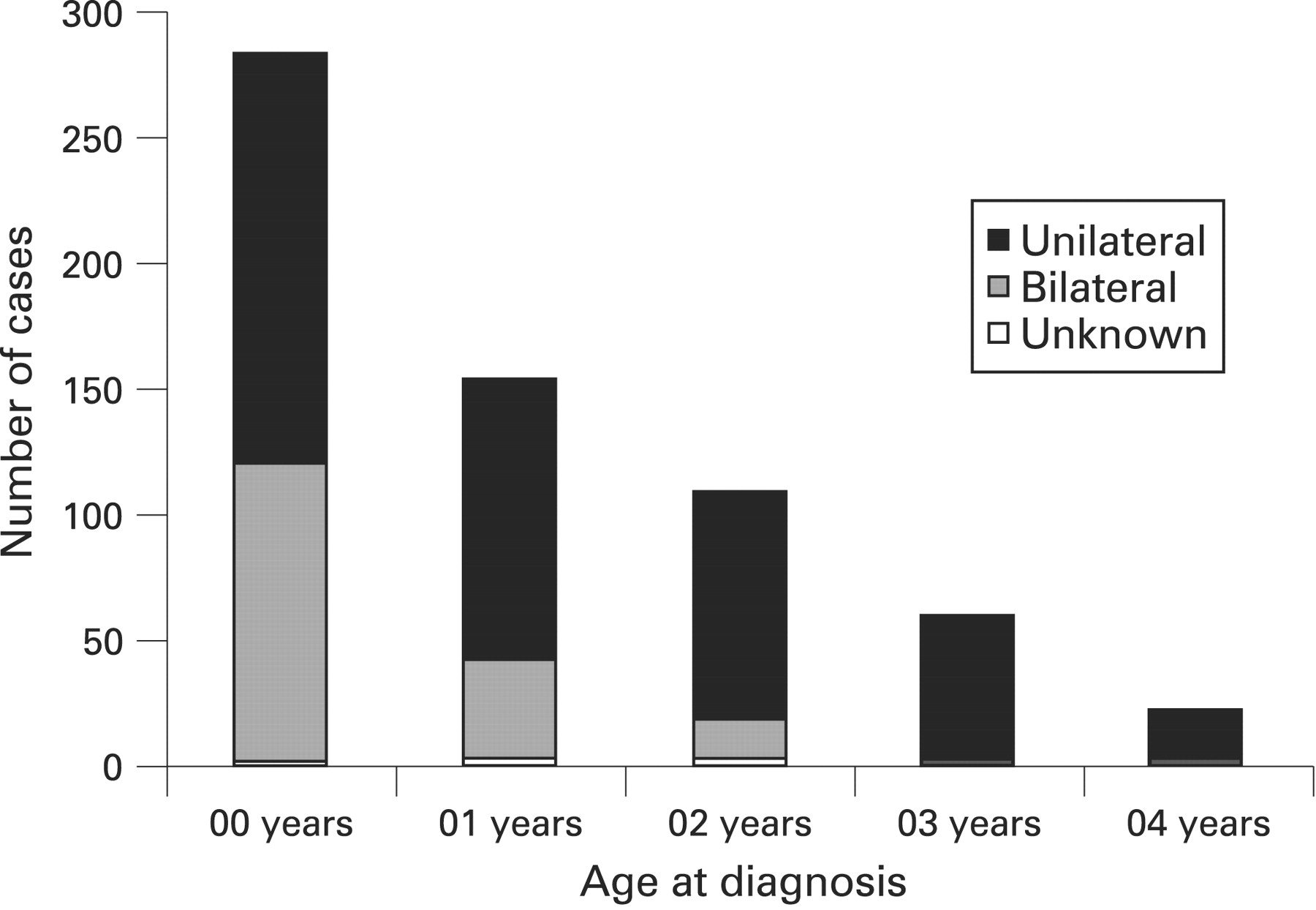
There were 473 unilateral cases, 176 bilateral cases and nine cases where laterality was unknown. The percentage of cases that were bilateral decreased with increasing age at diagnosis ranging from 41.5% in the age <1 year group to 3.6% in the age 5–9 year group. The percentage of cases that were unilateral increased with increasing age at diagnosis from 57.8% in the age <1 year group to 96.4% in the age 5–9 years group (fig 3). Sixty-seven per cent, 89% and 98% of bilateral cases were diagnosed by ages 1, 2 and 3 years, respectively. The overall mean age-adjusted incidence of retinoblastoma was 8.3 for unilateral and 3.2 for bilateral cases per million children aged 0–4 years. The distribution of laterality did not change over time.

{kind=link}
{kind=link}
{kind=link}
DISCUSSION
It is difficult to accurately study trends of a rare disease, such as retinoblastoma as random variation from year to year will inevitably produce notably wide incidence rates. A newer option for calculating the incidence, namely one based on birth cohorts, provides the least variation in annual incidence rates.9 However, birth cohort analysis was not possible with the SEER registry data, as the birth cohort information was not obtainable for each of the member areas. As retinoblastoma is predominantly a disease of early childhood, reporting of incidence in the susceptible age group (age less than 5 years or 10 years) appears to be justified.
The incidence in the USA of 11.8 per million children aged 0–4 years is comparable with the previously reported incidence within the USA3 10 and incidence in other countries such as The Netherlands,11 northern Europe9 and Singapore.12 The incidence of retinoblastoma in the USA has remained stable for the last 30 years, extending previous observations from the 1980s3 and 1990s.4 Stability of incidence of retinoblastoma has also been observed in the UK,13 14 The Netherlands,11 northern Europe9 and Singapore.12
The retinoblastoma with unilateral involvement has a higher incidence than with bilateral involvement, and unilateral cases are diagnosed at an older age as compared with bilateral cases. The proportion of bilateral cases decreases with increasing age at diagnosis (fig 3); 98% of bilateral cases were diagnosed by age 3 years. Since most unilateral cases are sporadic and non-heritable, one might expect the incidence of unilateral cases to vary over time if environmental factors contributed to the aetiology of these cases. Given that the incidence of retinoblastoma has remained stable over the past 30 years, a role for environmental factors, such as dietary intake or viral infection, in the aetiology of retinoblastoma seems unlikely. In addition, the incidence was stable for bilateral cases, indicating a stable germline mutation rate.
In summary, the overall mean age-adjusted incidence of retinoblastoma was 11.8 per million children ages 0–4 years (95% CI 10.9 to 12.8). There were no gender- or race-dependent variations in the incidence, and the incidence of retinoblastoma did not change over time.
REFERENCES
Footnotes
Competing interests: None.
Linked Articles
- At a glance