Article Text

Abstract
Background To determine the incidence and potential risk factors of cystoid macular oedema (CMO) following Descemet membrane endothelial keratoplasty (DMEK) with or without simultaneous cataract surgery.
Methods In this study, 155 eyes of 88 patients suffering from Fuchs endothelial dystrophy (81%), bullous keratopathy (17.6%) or other corneal diseases (1.4%) underwent DMEK. 52% were pseudophacic (DMEK) and 48% received simultaneous cataract surgery (DMEK combined with cataract surgery (Triple-DMEK)) at the Eye Center at Albert Ludwigs University of Freiburg between May 2011 and June 2013. Spectral-domain optical coherence tomography (SD-OCT) was performed 6 weeks, 3 months and 6 months following (Triple-)DMEK and in unscheduled visits due to limited or decreased visual acuity. The medical records were reviewed for pre-existing comorbidities limiting visual acuity. Patients with a history of macular oedema were excluded. We estimated the incidence of CMO using the Kaplan–Meier method. Potential risk factors for CMO were analysed with a Cox regression analysis and Pearson's correlation. The Cox model included the following variables: patient age and axial length, simultaneous cataract surgery, rate of rebubbling, donor age and donor endothelial cell density.
Results 13% of all eyes developed a single episode of CMO at the end of the follow-up. After 6 months, 13.3% of eyes following Triple-DMEK and 12.5% of eyes following DMEK showed CMO. There was a statistically significant correlation between CMO development and best spectacle corrected visual acuity. Long axial length had a protective effect on CMO development (HR=0.3; p=0.03). Under medical therapy, central foveal thickness decreased in all patients. CMO did not have a relevant effect on long-term visual acuity.
Conclusions CMO is a frequent complication following DMEK in phacic and pseudophacic eyes. The prognosis is excellent given medical treatment. We recommend regular SD-OCT monitoring during the first 6 months following DMEK.
- Cornea
Statistics from Altmetric.com
Introduction
The treatment of corneal endothelial disorders such as Fuchs endothelial dystrophy (FED) and bullous keratopathy (BK) has changed greatly during the last few years. Compared with penetrating keratoplasty (PK), posterior lamellar keratoplasty techniques such as Descemet stripping automated endothelial keratoplasty (DSAEK) or Descemet membrane endothelial keratoplasty (DMEK) allow a faster and refractively neutral visual rehabilitation1–4 and have a reduced risk of rejection.5 This seems especially true for DMEK.6 However, this surgical technique is not as standardised as DSAEK or PK. The most frequent complication following DMEK is graft dislocation, which can be treated with a repeated air fill of the anterior chamber. However, the complete spectrum of complications is not yet well characterised.
Cystoid macular oedema (CMO) is a well-known complication following intraocular surgery.7 However, the pathophysiology is not completely understood.8 It can be measured by various methods, including fluorescence angiography or different kinds of optical coherence tomography (OCT).8 The incidence of angiographically proven CMO is about 10-fold higher than the incidence measured by OCT.9 As OCT is the less invasive procedure and known to show clinically significant CMO, it is often used for screening or the diagnosis of CMO.10 The incidence of CMO following uneventful cataract surgery is 0.1%–2.4%.11 After complicated cataract surgery (ie, posterior capsule rupture with or without vitreous loss or after laser capsulotomy), the risk can increase 10 times up to 21% during the first month.12 In patients with pre-existing systemic diseases such as diabetes mellitus, CMO is reported to occur in up to 28.6% of cases after cataract surgery within the first postoperative year.13
We hypothesise that CMO can also occur following DMEK because of the intraoperative manipulation inside the anterior chamber. To determine the incidence of CMO following DMEK (with or without combined cataract surgery), we performed repeated optical coherence tomographies following DMEK in a large consecutive case series.
Methods
Our consecutive study cohort comprises 155 eyes of 88 patients who underwent either DMEK (52%, 80 eyes) or DMEK combined with cataract surgery (Triple-DMEK; 48%, 75 eyes). All operations were performed at the Eye Center at Albert Ludwigs University of Freiburg between May 2011 and June 2013. The underlying diagnosis was predominantly FED, followed by BK and other indications, such as failure of a previous corneal graft. Table 1 shows the baseline characteristics stratified by DMEK versus Triple-DMEK.
Baseline characteristics stratified by surgical procedure
All phacic eyes underwent Triple-DMEK. Axial length in the Triple-DMEK varied from 21.9 to 32.6 mm. Ocular comorbidities limiting the visual potential included central visual field defects (due to glaucoma or retinal vein occlusion) and dry age-related macular degeneration. Eyes with a history of CMO at the time of surgery or previous vitreoretinal surgery were excluded. During follow-up, no posterior capsulotomy was performed in the study eyes. In the DMEK group with pseudophacic eyes at the time of DMEK, previous complicated cataract surgery or capsular defects and CMO were excluded by querying the patients and their ophthalmologists. However, previous CMO could not definitely be excluded as no regular spectral-domain OCT (SD-OCT) controls were performed following cataract surgery at external centres. Additionally, we did not observe any signs of previous postsurgical inflammation (eg, following cataract surgery) at the time of (Triple-)DMEK. The corneal opacity rather explains best spectacle corrected visual acuity (BSCVA).
There were three patients suffering from diabetes mellitus without any signs of diabetic retinopathy at the date of surgery (3.4%). None of these developed CMO during follow-up. Among the eyes that developed CMO, none received topical antiglaucomatous medication such as prostaglandinanaloga, β-blocker, α-agonists or systemic carbonic anhydrase inhibitors.
All grafts came from warm storage according to the guidelines of the European Eye Bank Association. DMEK was performed under general anaesthesia as described elsewhere.14 The grade of lens opacity was mild to moderate in the phacic eyes. In the case of Triple-DMEK, a 2.2 mm clear corneal incision phacoemulsification was conducted before transplantation. We inserted an aspheric posterior chamber lens into the capsular bag in all cases (CT Asphina 409M, Zeiss, Germany). Afterward, 1% acetylcholine (Miochol-E, Bausch & Lomb) was administered into the anterior chamber to induce miosis for peripheral iridectomy.
Time was measured from the beginning of graft unfolding until attachment was achieved by the final air bubble (duration of DMEK; see table 1) as well as the duration of the whole surgical procedure, including an eventual cataract surgery (duration of surgery; see table 1).
Medical aftercare included preservative-free artificial tears (Vismed, TRB Chemedica AG) as well as topical dexamethasone (Dexa EDO, Dr. Gerhard Mann GmbH) 5× per day. This was tapered over 5 months. In the case of epithelial defects, dexpanthenol and ofloxacin ointment (Bepanthen, Bayer HealthCare; Floxal, Dr. Gerhard Mann GmbH) were administered until re-epithelialisation.
We performed SD-OCT (Spectralis-OCT, Heidelberg Engineering GmbH) 6 weeks, 3 months and 6 months following (Triple-)DMEK. Unscheduled visits including SD-OCT were conducted in the case of unexplained loss in BSCVA. BSCVA was performed at every visit.
We defined CMO as intraretinal or subretinal fluid spaces in the region of the foveola as seen in SD-OCT. For quantification, central foveal thickness was measured (1 mm subfield of the 1, 3, 6 mm Early Treatment Diabetic Retinopathy Study Thickness Map, HRA/Spectralis Viewing Module (V.5.1.2.0) Heidelberg Eye Explorer, V.1.6.2.0).
We treated episodes of CMO with prednisolon acetate (Predni POS 1%, Ursapharm Arzneimittel GmbH) and ketorolac–trometamol (Acular, Mtk-Pharma Vertriebs GmbH) four times daily each in addition to systemic acetazolamide (Diamox, Goldshield Pharmaceuticals, NLA Tower) 125 mg two times daily. This regimen was scheduled for 6 weeks, followed by repeated SD-OCT. In one case where CMO was not reduced by this regimen, we continued treatment with intravitreal injections of bevacizumab and triamcinolon.
To assess graft attachment, anterior segment OCT was conducted during the aforementioned controls (Casia SS-1000, Tomey, Japan). In the case of clinical relevant graft detachment, rebubbling was performed with complete refilling of the anterior chamber with air.
Statistical analysis of the correlations included a proportional hazards Cox model and Kaplan–Meier analysis to estimate the incidence of CMO. Pearson's correlation was used for bivariate correlations.
The institutional ethics committee approved our trial. Informed consent was collected from all study patients prior to the measurements. Our non-interventional study adhered to the tenets of the Declaration of Helsinki.
Results
The cumulative incidence of CMO following Triple-DMEK and DMEK is displayed in figure 1.

Kaplan–Meier estimation of CMO following DMEK and Triple-DMEK. Most CMO occurred in the early postoperative period. There was no considerable difference between DMEK and Triple-DMEK. CMO, cystoid macular oedema; DMEK, Descemet membrane endothelial keratoplasty; Triple-DMEK, DMEK combined with cataract surgery.
Follow-up data were available for 6 months in 146 eyes (94%). At the end of the follow-up period, 13% of all eyes had developed singular CMO (13.3% of eyes following Triple-DMEK and 12.5% of eyes following DMEK). The mean central foveal thickness was 401 µm in the CMO group and 303 µm in the group without CMO (p<0.001). There was a negative association between BSCVA and episodes of CMO (p<0.01; Pearson's correlation). Following the first diagnosis of CMO, these eyes showed lower BSCVA than eyes without CMO (figure 2). In both groups, there is an increase in BSCVA. The difference in BSCVA between both groups decreases with time.
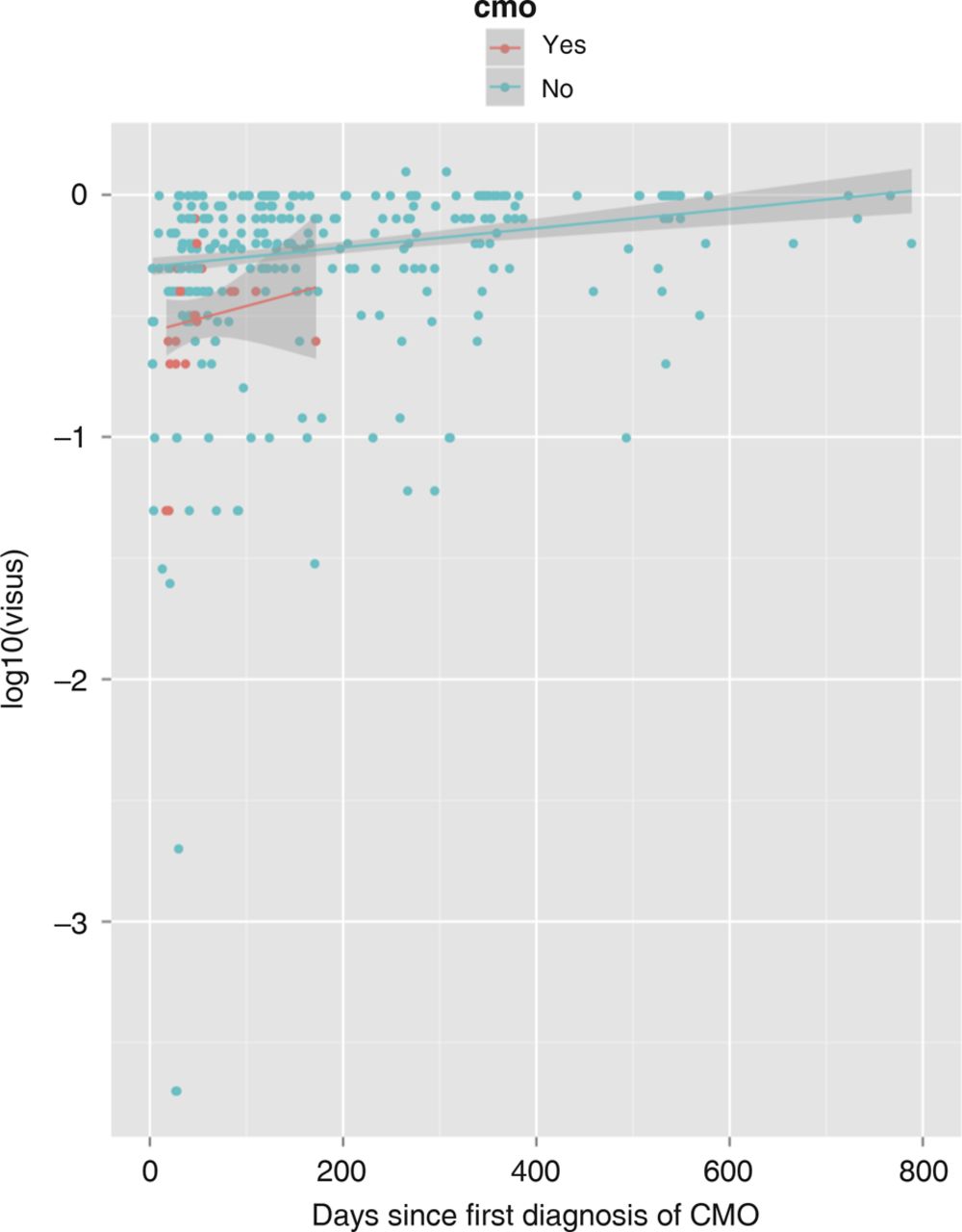
Trajectories of BSCVA in patients with and without CMO following the first diagnosis of CMO. Eyes suffering from CMO show lower BSCVA at the time of diagnosis compared with eyes without CMO. BSCVA, best spectacle corrected visual acuity; CMO: cystoid macular oedema.
All CMO except one (which had to be treated with intravitreal injections) disappeared with the aforementioned medical treatment followed by visual recovery (figure 3). There was no recurrence of CMO during the follow-up period. Among the 67 patients undergoing (Triple-)DMEK in both eyes, bilateral CMO did not occur. None of the diabetic patients developed CMO.

{kind=link}
{kind=link}
{kind=link}
Dynamics of central foveal thickness (A) and BSCVA (B) following (Triple-)DMEK. There is a spike in central foveal thickness at the time of occurrence (day 0). Afterward, the central foveal thickness constantly decreases (A). Following occurrence and medical treatment of CMO, BSCVA rises constantly during the entire investigated postoperative period (B). CMO, cystoid macular oedema; DMEK, Descemet membrane endothelial keratoplasty; Triple-DMEK, DMEK combined with cataract surgery; BSCVA, best spectacle corrected visual acuity.
In the proportional hazards Cox model of the whole group, none of the possible risk factors reached statistical significance (table 2).
Proportional hazards Cox model for DMEK and Triple-DMEK patients
However, when looking at the Triple-DMEK patients (table 2) alone, short axial length was statistically significantly associated with CMO (p<0.01, table 2).
We observed the following complications:
-
Graft detachment or dislocation (20%; treated by air refilling of the anterior chamber)
-
Graft failure with persisting corneal oedema (2.6%; treated with repeated DMEK or with secondary PK)
-
Persistent CMO in one case (successfully treated with intravitreal injections).
Discussion
Incidence of CMO following DMEK
In this study, we observed a considerably elevated incidence of CMO (13%). The incidence of CMO following DMEK is higher than the frequency of CMO measured by OCT following uncomplicated cataract surgery (0.1%–2.4%11). Many groups have not yet investigated the incidence of CMO following DMEK or other lamellar endothelial keratoplasty methods. In particular, we are not aware of any other homogenous large cohort study investigating CMO following DMEK on the basis of SD-OCT controls.
Dapena et al15 were the first to report a CMO risk of 0.7% in 135 uneventful DMEK surgeries. The incidence of CMO following DSAEK is reported to be higher: Suh et al16 indicate a CMO incidence of 5% following 118 DSAEK procedures. The difference between our data and the literature may be due to our routinely performed screening procedure with SD-OCT. After uncomplicated intraocular surgery, routine controls are performed less frequently, and SD-OCT often is not performed when BSCVA improves.
Do we overestimate the incidence of CMO in comparison with the background of Dapena et al?15 This could be the case if CMO is not clinically significant because it would have resolved spontaneously, as it is known to do following cataract surgery.11 However, we observed a significant correlation between CMO and BSCVA (p<0.01 in Pearson's correlation). The maximal central foveal thickness was measured at the time of onset of CMO (figure 3A), but BSCVA of the whole cohort improved continuously at that time point (figure 3B). Separating the eyes suffering from CMO in the trajectory of BSCVA (figure 2), there obviously is a lower BSCVA in the period following the first diagnosis of CMO confirming statistical significance in the Pearson's correlation (p<0.01). Thus, CMO may slow visual rehabilitation. Following (Triple-)DMEK, the correlation between CMO and BSCVA may be superposed by any other wound healing process, such as regression of corneal oedema. Therefore, no definite correlation of CMO and BSCVA can be drawn from our study.
Potential risk factors for CMO following DMEK
To evaluate potential mechanisms for the development of CMO following DMEK, we assessed potential confounders.
-
High axial length: the longer the patient's eyeball is, the longer the diffusion pathway to the macular region. In the case of inflammatory mediators, a gradient of the molecules forms along this distance, leading to an increasing dilution toward the macular region. The significant and protective impact of axial length on CMO following DMEK found in this study supports this hypothesis (table 2).
-
Duration of surgery and amount of manipulation: it is known that manipulation of the iris causes inflammation. This may increase the risk of CMO.11 As Triple-DMEK and DMEK patients showed identical rates of CMO (figure 1) and Triple-DMEK was not a significant risk factor for CMO in the whole group (table 2), this may not have had any impact on CMO in our cohort. But, in contrast to uncomplicated cataract surgery, (Triple-)DMEK includes more manipulation on the iris (eg, iridectomy and graft unfolding under intracameral air). This may explain an increased rate of CMO in Triple-DMEK compared with cataract surgery alone in standard cases.
-
Eyes with rebubbling: speculating on an increase in inflammation with repeated surgery and intracameral air, a negative effect of rebubbling on CMO could be expected.17 ,18 This was not the case (p=0.42, see table 1) indicating that rebubbling only may cause minor stress on the ocular tissues.
-
Donor characteristics such as donor age or preoperative endothelial cell density do not seem to influence the risk of CMO (table 2).
-
Diabetes mellitus does not seem to be a pronounced risk factor for CMO following Triple-DMEK in our cohort as no diabetic patient developed CMO.
Triple-DMEK versus DMEK as risk factors for CMO
We found a negligible difference of 13.3% CMO following Triple-DMEK and 12.5% following DMEK alone after 6 months of follow-up (figure 1). On first glance, this may seem to be a paradox: in Triple-DMEK, the risk for CMO could be higher, as more surgical manipulation is needed and the geometrical situation of the anterior segment is changed more severely than following DMEK alone.
In addition, pseudophacic eyes with endothelial insufficiency often have opaque and thick corneas because of previous complicated surgery. Because these corneas tend to have more haze blurring vision during surgery, they require more delicate unfolding procedures with more manipulation. Furthermore, all phacoemulsifications in the Triple-DMEK group were uncomplicated, so a low rate of CMO induction would have been expected. Laaser et al19 are the only other group to compare a Triple-DMEK and a DMEK cohort. They also reported no elevated complication rate in Triple-DMEK compared with DMEK alone.
Taken together, anatomical respectively geometrical conditions of the patients eye may be relevant for the development of CMO, whereas intraoperative or perioperative factors affecting the grade of inflammation do not seem to be relevant in our cohort. Compared with cataract surgery alone (without iridectomy or intracameral air), (Triple-)DMEK may lead to increased rate of CMO because of this regularly performed manipulation on the iris.
Open questions for further studies may be the rate of CMO following DMEK in phacic eyes without simultaneous cataract surgery as well as the rate of CMO following cataract surgery in eyes with previous DMEK.
In conclusion, we recommend considering SD-OCT during the first 6 months following DMEK or Triple-DMEK, at least in eyes with insufficient visual rehabilitation. Eyes with short axial length require special attention. DMEK-related CMO could be effectively treated with the first-line medical treatment routinely applied in CMO following cataract surgery. Concerning prophylactic therapy, the surgeon has to perform a thorough risk analysis because, on the one hand, frequency of CMO following DMEK seems to be higher than following cataract surgery. On the other hand, and in contrast to CMO following cataract surgery, DMEK-related CMO in one eye does not seem to increase the risk for the fellow eye.
References
Footnotes
-
Contributors Each author has contributed substantially to acquisition of data, analysis and writing the manuscript according to the ICMJE guidelines for authorship.
-
Competing interests None.
-
Ethics approval Institutional ethics committee of the Albert Ludwigs University of Freiburg, Germany.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance