Article Text

Abstract
AIM To evaluate sub-Tenon’ s anaesthesia as an alternative to peribulbar anaesthesia.
METHODS 109 consecutive patients listed for various eye operations (including cataract, trabeculectomy, and vitrectomy) under peribulbar anaesthesia were operated on under sub-Tenon’s anaesthesia instead. After topical anaesthesia a buttonhole was fashioned through the conjunctiva and Tenon’s capsule 10 mm posterior to the limbus. 1.5 ml of lignocaine 2% was then delivered to the posterior sub-Tenon’s space using a blunt cannula. The surgical procedure was performed immediately after the completion of the anaesthetic procedure. Chemosis, conjunctival haemorrhage, degree of akinesia, and pain scoring were analysed.
RESULTS There were no anaesthesia related complications. The administration of the block was painless for 99.1% of the patients. In all, 97.3% reported no pain during surgery. There was no akinesia when assessed just after the completion of the block and akinesia was limited when assessed after surgery. Chemosis and conjunctival haemorrhage were frequent but caused no intraoperative problems.
CONCLUSION Sub-Tenon’s anaesthesia is an efficient and safe anaesthetic technique. It is a good alternative to peribulbar anaesthesia.
- sub-Tenon’s anaesthesia
- peribulbar anaesthesia
Statistics from Altmetric.com
Peribulbar or retrobulbar anaesthesia, while providing excellent analgesia and akinesia, have been associated with rare1 but numerous ocular complications including diplopia,2 orbital haemorrhage,3 globe perforation,4 central retinal vein or artery occlusion,5 brainstem anaesthesia,67 optic nerve trauma,8 and ptosis.9 In addition, preoperative intravenous sedation is often required because patients find the injection painful and frightening. Recently there had been renewed interest in sub-Tenon’s anaesthesia.10-12 It is not a new technique since it was described as early as 1884 by Turnbull.13 This prospective study reports our experience of sub-Tenon’s anaesthesia using a blunt cannula for various anterior and posterior segment eye operations.
Materials and methods
From February1996 to July 1996, 109 consecutive patients (47 males, 62 females with a mean age of 66) scheduled for peribulbar anaesthesia underwent surgery under sub-Tenon’s anaesthesia instead. Seventy six had phacoemulsification cataract extraction (temporal corneal or scleral tunnel incision), five underwent combined phacoemulsification with trabeculectomy, three pterygium removal, five trabeculectomy, six had a three port pars plana vitrectomy for dislocated fragments of lens in the vitreous following cataract surgery, three a pars plana vitrectomy for vitreous haemorrhage, three had silicone oil removal, one radial keratotomy, one secondary lens implantation, one artificial lens removal for chronic endophthalmitis, two hyphaema evacuation, and three necessitated surgical treatment of iris prolapse following cataract surgery.
Duration of surgery, site of sub-Tenon’s anaesthesia, conjunctival chemosis (0 = no chemosis; + = chemosis involving one quadrant; ++ = chemosis involving two quadrants; +++ = chemosis involving three or four quadrants), subconjunctival haemorrhage (0 = no haemorrhage; + = haemorrhage involving one quadrant; ++ = haemorrhage involving two quadrants; +++ = haemorrhage involving three or four quadrants) were all noted on a chart. Patients were asked to score the pain during the anaesthetic procedure and during the surgery (0 = no pain, no sensation; 1 = slight ‘sensation’ or discomfort but no pain; 2 = slight pain; 3 = moderate pain; 4 = intense pain). Akinesia was assessed by the surgeon just after the completion of the sub-Tenon’s anaesthesia and at the end of the surgical procedure using a subjective four category scale where 0 represents complete movement remaining, 1 moderate movement, 2 slight movement, and 3 no movement.
ANAESTHETIC TECHNIQUE
All the patients were monitored and had intravenous access. Four drops of topical 1% preservative free amethocaine (tetracaine) were applied to the cornea and conjunctiva. The patients were prepared and draped and a lid speculum inserted. The patients were asked to move their eye so as to expose the area to be injected. Using blunt scissors, a buttonhole through the conjunctiva and Tenon’s capsule was fashioned 10 mm posterior to the limbus. A specially designed blunt cannula (Greenbaum sub-Tenon’s flexible cannula for 82 patients, length of the cannula 15 mm, and Visitec sub-Tenon’s rigid cannula for 27 patients, length of the cannula 26 mm) was then passed through the buttonhole and slid 5 to 7 mm along the bare sclera. A volume of 1.5 ml of lignocaine 2% was then administered. The anaesthetic solution was delivered in one of the four quadrants of the globe delimited by the recti muscles. The best exposed quadrant or the quadrant the further away from the operative section (in cases of scleral incision) was chosen to be the site of injection—50 patients had an inferonasal approach, 10 superonasal, 44 inferotemporal, and five superotemporal.
In all cases the operation was started immediately after completion of sub-Tenon’s anaesthesia without use of oculopression.
Three anxious patients received mild intravenous preoperative sedation (propofol 10 mg).
Results
There were no anaesthesia related complications. No patients scheduled for peribulbar anaesthesia were considered unsuitable for the sub-Tenon’s anaesthesia. In no case was sub-Tenon’s anaesthesia changed to peribulbar anaesthesia.
Figures 1 and 2 report pain scoring during the sub-Tenon’s anaesthesia procedure and during operation. Figures 3 and 4 show the degree of akinesia. Figure 5 represents chemosis and Figure 6 subconjunctival haemorrhage.
Pain scoring for the delivery of the sub-Tenon’s anaesthetic procedure (0 = no pain, no sensation; 1 = slight ‘sensation’ or discomfort but no pain; 2 = slight pain; 3 = moderate pain; 4 = intense pain).

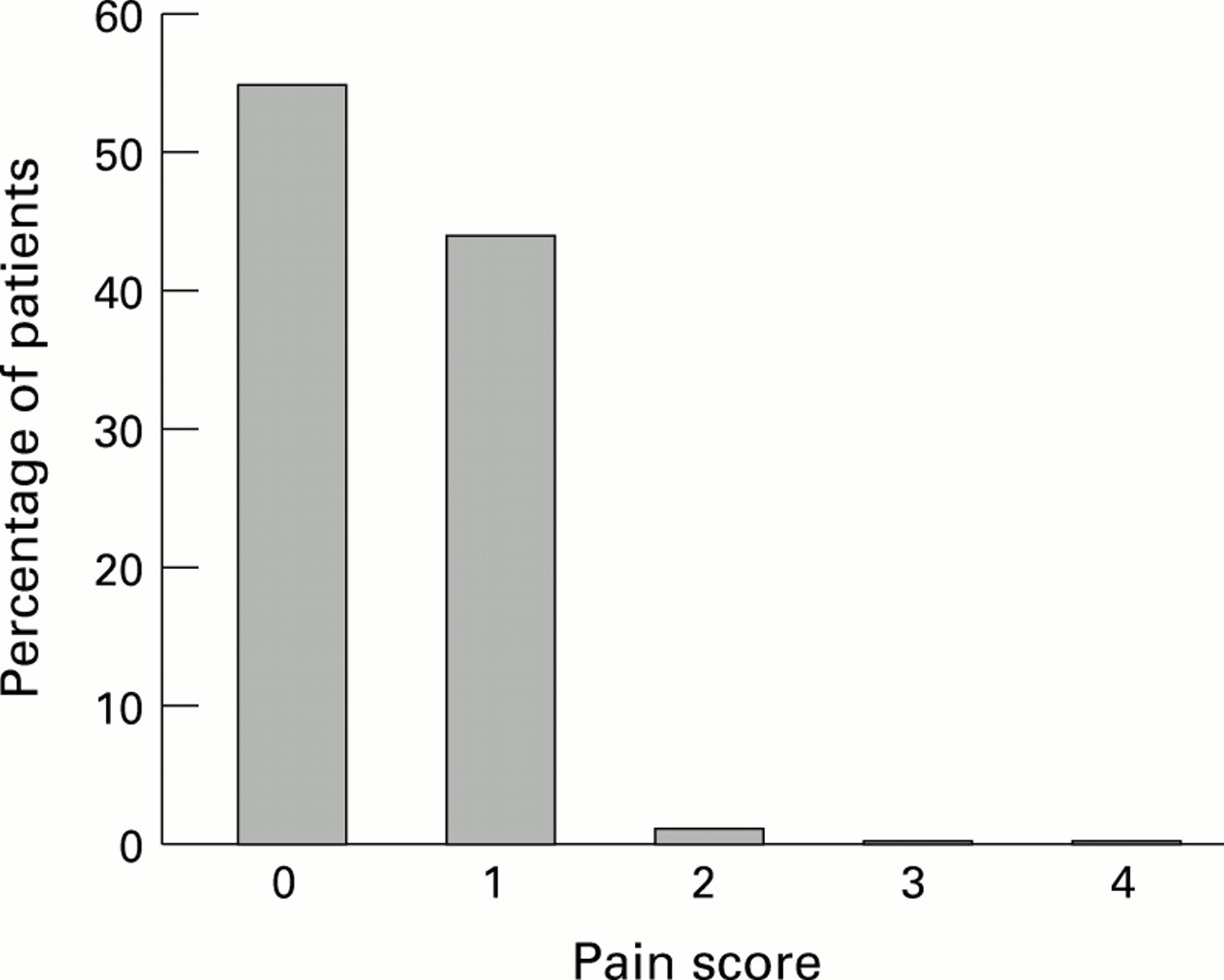
Pain scoring recorded for the operative procedure (0 = no pain, no sensation; 1 = slight ‘sensation’ or discomfort but no pain; 2 = slight pain; 3 = moderate pain; 4 = intense pain).
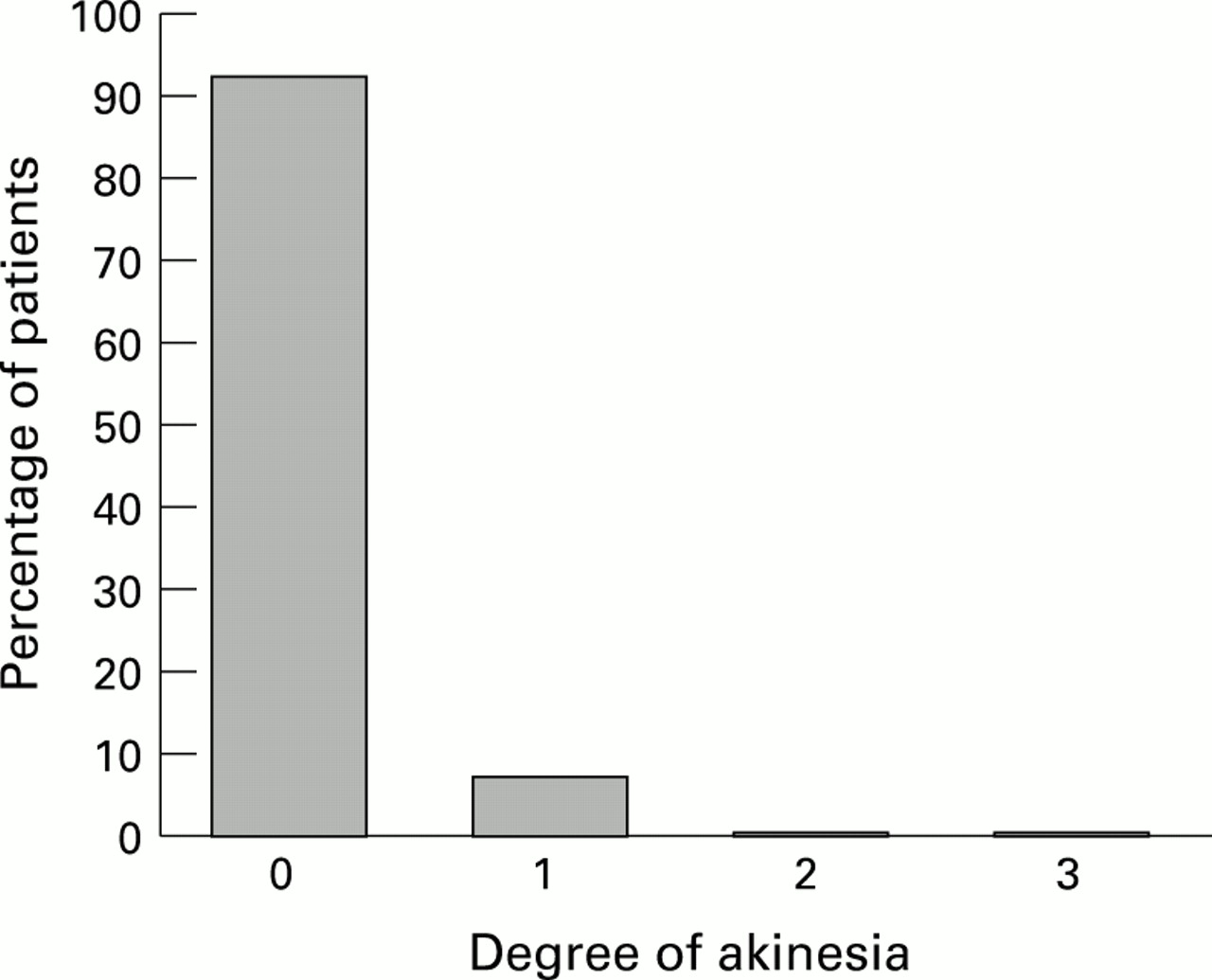
Degree of akinesia just after sub-Tenon’s anaesthesia (0 = complete movement remaining; 1 = moderate movement, 2 = slight movement, and 3 = no movement).
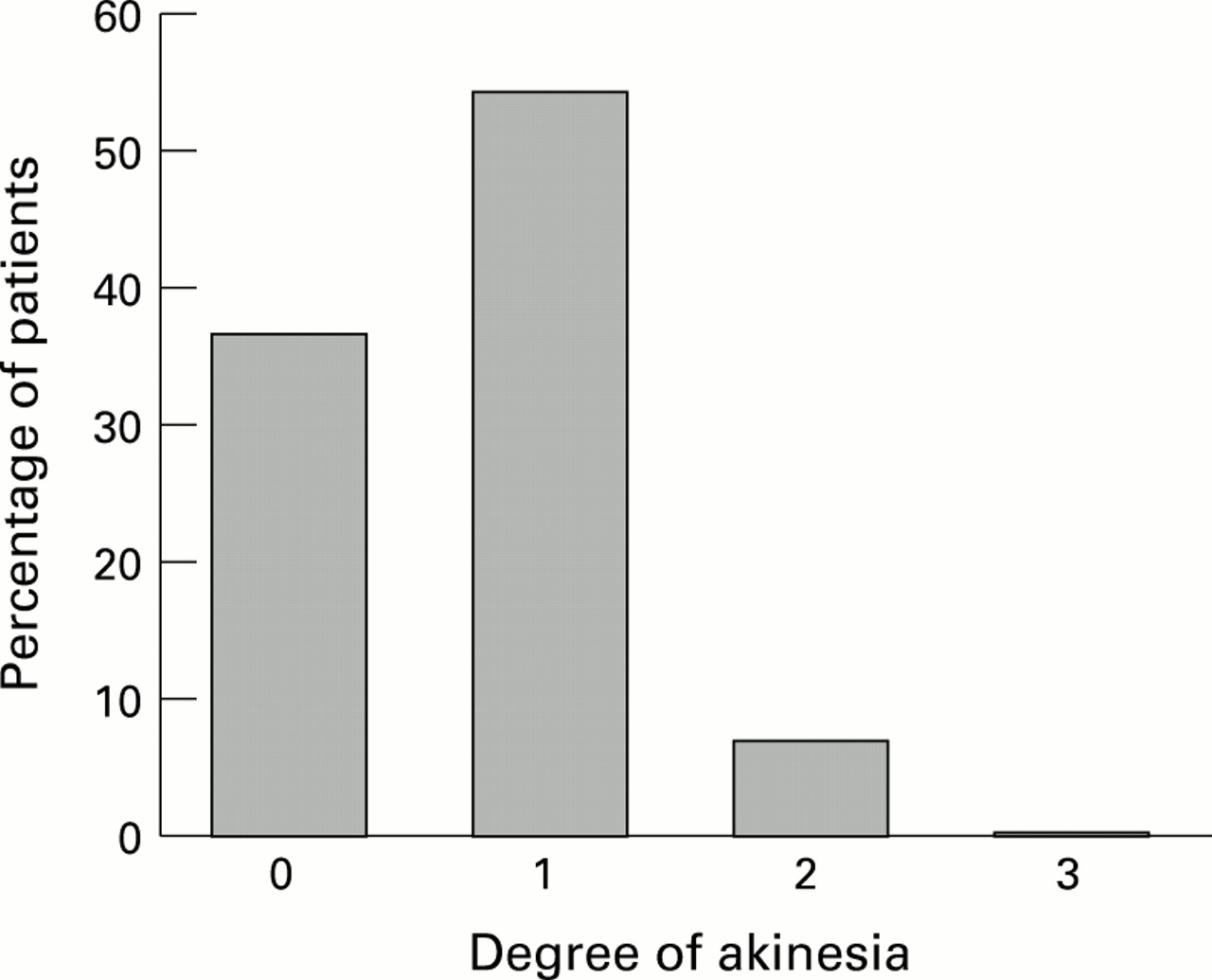
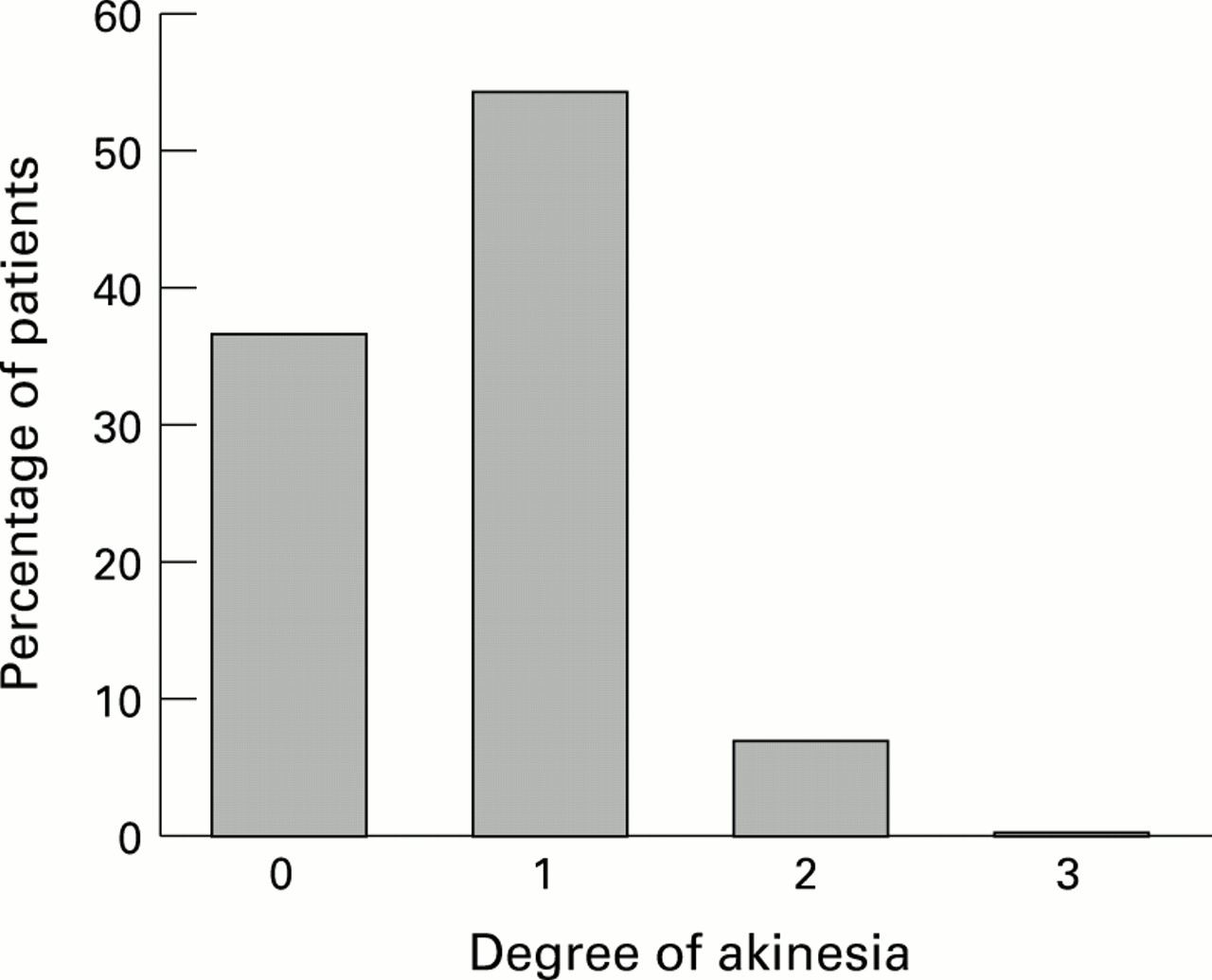
Degree of akinesia at the end of surgery (0 = complete movement remaining, 1 = moderate movement, 2 = slight movement, and 3 = no movement).
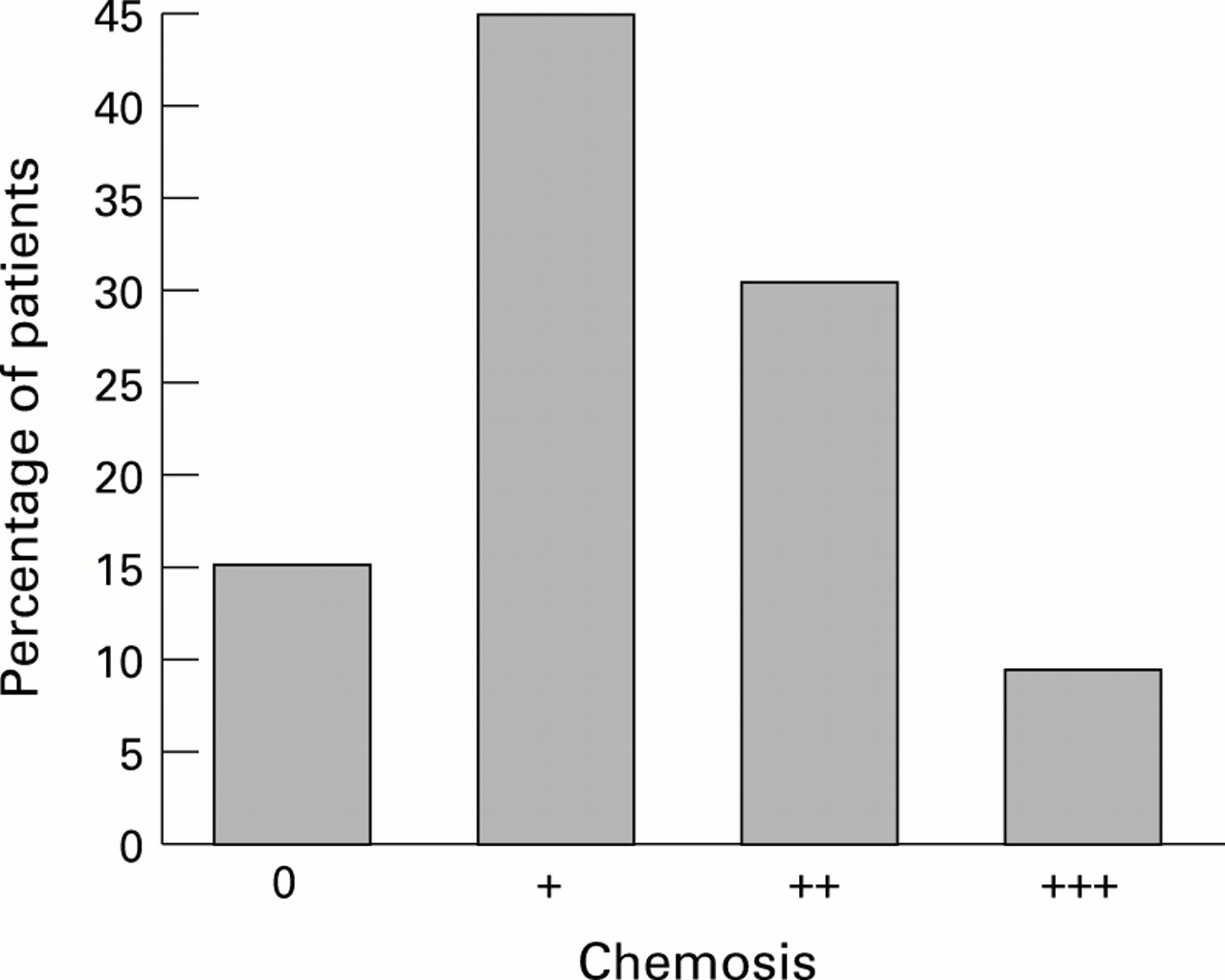
Chemosis (0 = no chemosis; + = chemosis involving one quadrant; ++ = chemosis involving two quadrants; +++ = chemosis involving three or four quadrants).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
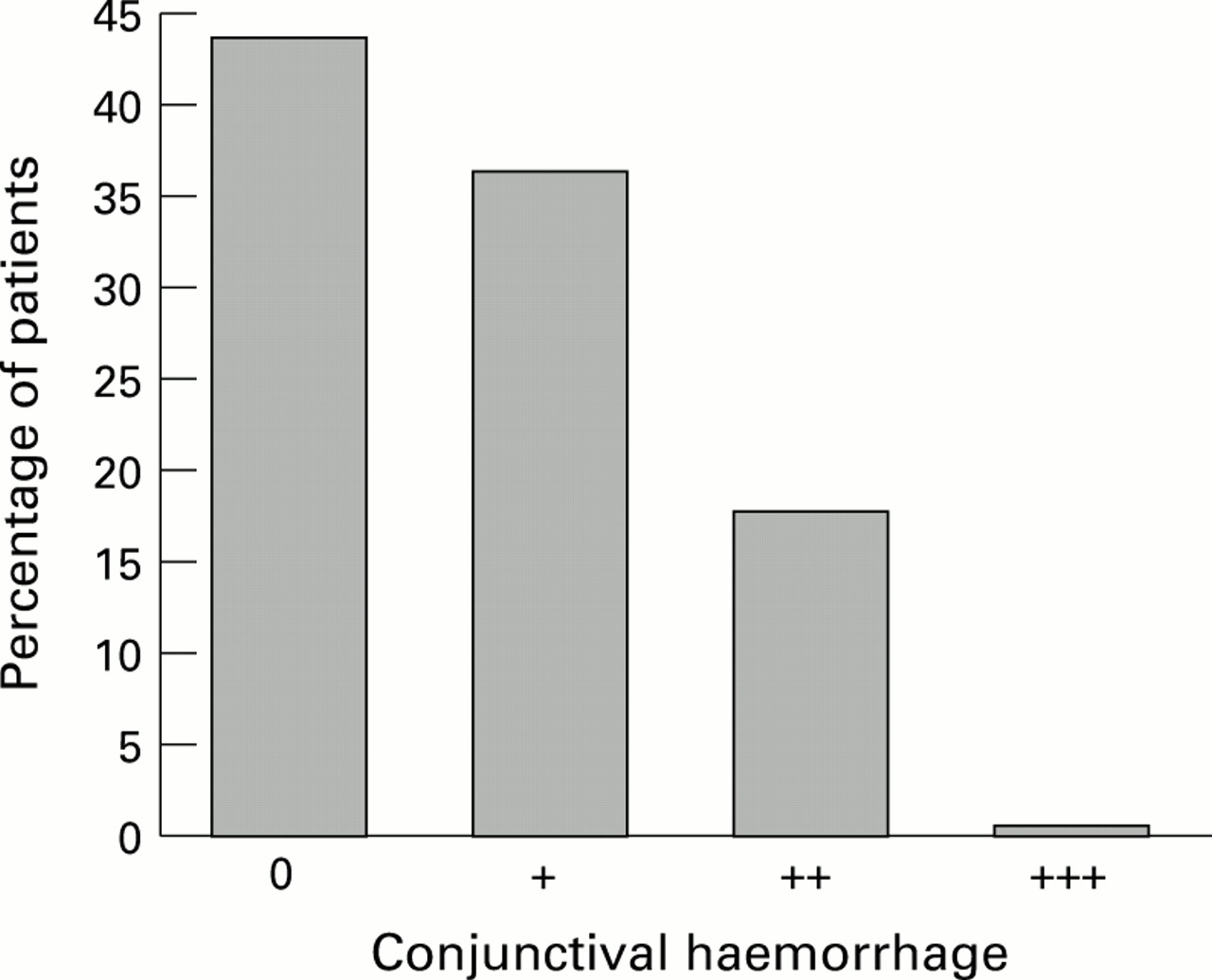
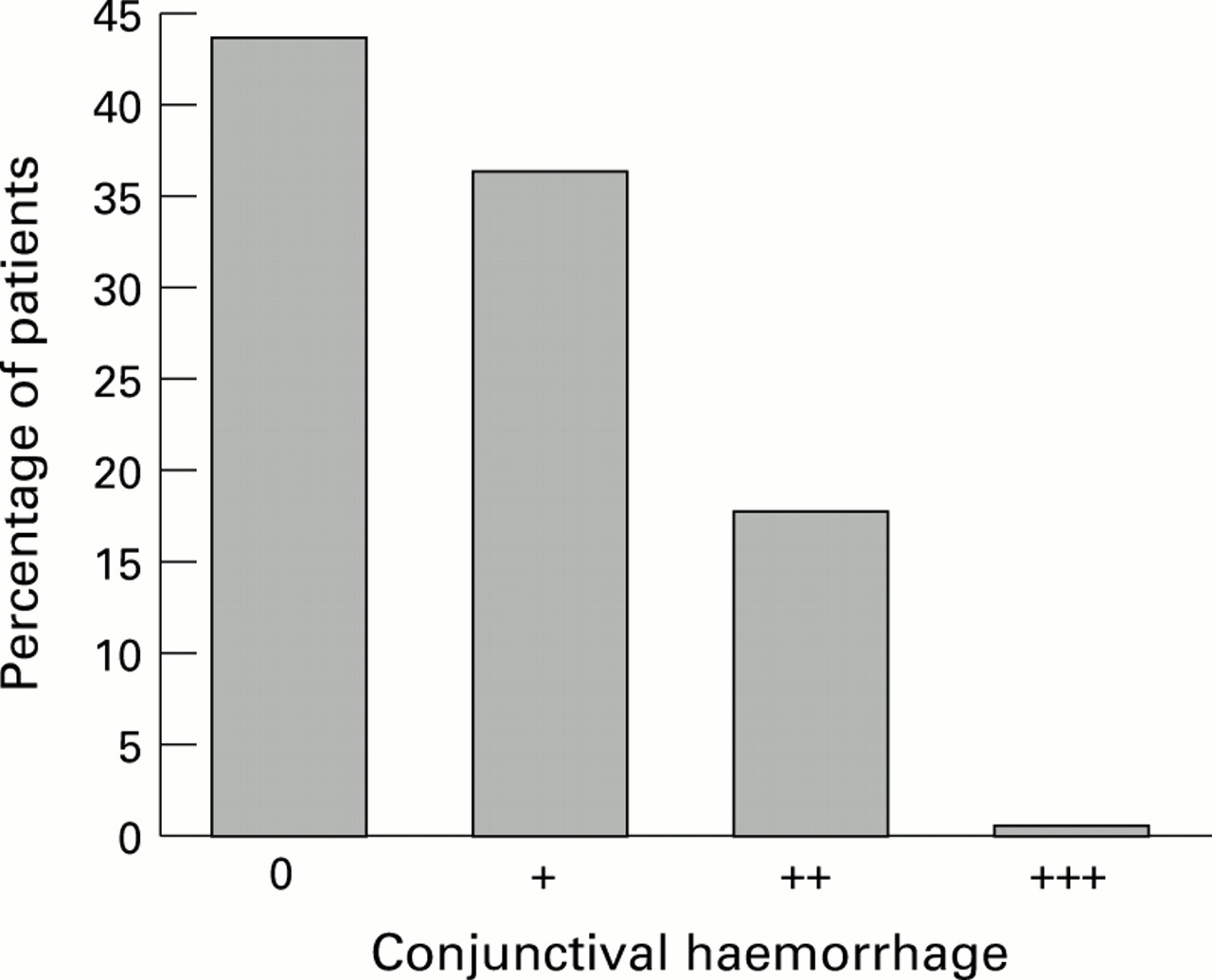
Conjunctival haemorrhage (0 = no haemorrhage; + = haemorrhage involving one quadrant; ++ = haemorrhage involving two quadrants; +++ = haemorrhage involving three or four quadrants).
Complications during surgery (one capsular rupture during phacoemulsification, one hyphaema following iridectomy during trabeculectomy) were not related to the anaesthetic method. The operating time ranged from 10 minutes to 1 hour and 10 minutes (mean 35 minutes).
Discussion
ANALGESIA
The sub-Tenon’s anaesthesia procedure was painless for 99.1% of the patients (Fig 1); 55% reported no pain or ‘sensation’, and 44.1% only ‘sensations’ during this procedure. The patients’ satisfaction is enhanced by warning them just before the injection that they might experience a mild ‘sensation’ like a pressure or even discomfort but they will not feel pain. Stevens10 reports a median score of 1 (slight discomfort) on a 0 to 10 graded pain scale for the delivery of the sub-Tenon’s block.
The anaesthetic block was very efficient; 97.3% of the patients (Fig2) reported no pain during surgery (87.2% reporting no pain nor sensation and 10.1% only ‘sensation’). The deepness of analgesia has been reported by all the authors using this technique for cataract surgery,10-121415pan-photocoagulation,16 retinal detachment and vitreous surgery,1718 and strabismus surgery.19 The cannula follows the contour of the globe under Tenon’s capsule until posterior to the equator and delivers the solution to the posterior sub-Tenon’s space. Then, the solution diffuses back to the intraconal region blocking the long ciliary and the short ciliary nerves as they enter the globe and further back the ciliary ganglion.
AKINESIA
In our experience akinesia was always limited. When assessed just after the anaesthetic injection (Fig 3), complete eye movement remained for 93.7% of patients and no patients had total akinesia. At the end of the surgical procedure (Fig 4), no patients reached complete akinesia and 37.6% had no akinesia at all. None of the patients who had cataract surgery had good akinesia (they were all graded 1 or 2). Our study agrees with Tsuneoka et al 14 who also report poor akinesia using 1 ml of a 2% lignocaine solution. Other authors have a different experience. Mein and Woodcock18 report complete akinesia, after a four quadrant injection of 1.5 ml of an anaesthetic solution of lignocaine 1% and bupivacaine 0.375% mixed with hyaluronidase, in 58 cases of vitreoretinal surgery (the time to obtain complete akinesia is not mentioned). Greenbaum12 reports good akinesia within 1 minute of anaesthetic administration using a 2 ml solution of a 4% lignocaine and 0.75% bupivacaine 50:50 mixture. Stevens10reports complete akinesia (assessed 15 minutes after completion of the sub-Tenon’s procedure using a 50:50 mixture of lignocaine 2% and bupivacaine 0.5% solution) in 27 out of 50 patients who underwent cataract surgery. Difference in the time of assessment and in the volume or mixture of the anaesthetic solution administered can explain the various reports of akinesia depending on publications.
Some surgeons find difficult to work without akinesia; however, as reported by many authors1420 the lack of akinesia does not cause intraoperative difficulties. Stabilisation of the globe is adequate during a two handed procedure (as during phacoemulsification or vitrectomy). Most of the time the patients do not have eye movement. If necessary, unwanted movements can be controlled by forceps fixation. Lack of akinesia can even be helpful to the surgeon when asking the patient to look in a particular direction to expose a desired area. No complications have occurred during surgery because of ocular motility. Nevertheless, in cases of patients completely unable to cooperate (patients suffering dementia or unable to understand the language), we would rather use peribulbar or retrobulbar anaesthesia.
CHEMOSIS
Chemosis is frequent; 39.4 % of the patients had a chemosis involving more than one quadrant (Fig 5). It takes a little practice to limit chemosis by ensuring that the anaesthetic solution is truly delivered to the posterior sub-Tenon’s space and not to the anterior subconjunctival space.
Subconjunctival haemorrhage is caused by fine vessels inevitably severed on making the conjunctival cut. In our study (Fig 6), it was frequent; more than half the patients (56%) had conjunctival haemorrhage. Most of the time it was limited (only one patient had three quadrants involved), and no patient had sufficient haemorrhage to cause a problem. Stevens10 reports subconjunctival haemorrhage involving at least one quadrant in 32% of the patients. Some authors12 advocate using cauterisation before making the buttonhole to lower the incidence of haemorrhage.
The benefits of sub-Tenon’s anaesthesia over peribulbar or retrobulbar anaesthesia are: it eliminates the risks of the ‘needle’ techniques (however, these procedures if performed by skilled clinicians are not painful and most complications result from poor training) the analgesia is immediate and the anaesthetic volume being minimal, there is no rise in ocular pressure21 and no need for globe compression no preoperative sedation is necessary.
Yet, because of the poor akinesia we do not consider sub-Tenon’s anaesthesia to be adequate for patients unable to cooperate (no cases in our study) and for surgery necessitating a wide opened eye such as in keratoplasty or manual extracapsular extraction (no cases in our study).
With cataract surgery, topical anaesthesia2223 is also advocated as a safe and atraumatic technique. The main advantages of topical over sub-Tenon’s anaesthesia are the absence of chemosis and subconjunctival haemorrhage and a quicker visual recovery. Yet, topical anaesthesia is not as efficient as sub-Tenon’s anaesthesia and spread on the zonules and iris sensitivity sometimes causes ‘sensations’ or even slight pain as reported by many authors.24-26Fukasaku and Marron,15 comparing sub-Tenon’s and topical anaesthesia, found that 1% of the patients under sub-Tenon’s anaesthesia reported pain as against 31% in the topical group. We still use topical anaesthesia for standard cataract surgery but in cases of very anxious patients or patients whose pupillary dilatation is not sufficient (risk of iris chafing) we favour sub-Tenon’s anaesthesia. During topical anaesthesia, if the patients feel any discomfort, we perform a supplementary sub-Tenon’s anaesthesia.
We did not notice any difference between the two cannulas. However, the Visitec cannula is rigid and longer than the Greenbaum cannula. This could be an advantage to ensure reaching the posterior sub-Tenon’s space; however, it could theoretically be more damaging to a vortex vein. We did not find any advantage or disadvantage in the different routes used to infuse the anaesthetic solution: the access and the efficiency of the block was the same in the four quadrants.
Conclusion
Sub-Tenon’s anaesthesia is a simple, safe, atraumatic technique. Its benefits are numerous. It can be proposed as a good alternative to peribulbar or retrobulbar anaesthesia in anterior and posterior segment eye surgery.