Article Text

Abstract
AIM To investigate changes in corneal touch sensitivity following excimer laser photorefractive keratectomy (PRK) using different beam configurations.
METHODS 20 subjects were given a unilateral −3.00 D correction with either a 5 mm (26 μm, n=10) or 6 mm (42 μm, n=10) beam diameter. Thirty subjects underwent a unilateral −6.00 D correction with 5 mm (62 μm, n=10), 6 mm (78 μm, n=10), or multizone (62 μm, n=10) treatments. The multizone treatment was 6 mm in diameter with the depth of the 5 mm treatment. Corneal sensitivity was measured using a slit-lamp mounted Cochet-Bonnet aesthesiometer before and at 1, 3, 6, and 12 months after PRK. Stimulus locations included points lying within the ablated zone (central) and outside (peripheral). These were compared with the equivalent locations in control (untreated) eyes.
RESULTS There was a significant reduction in corneal sensitivity within the central (ablated) zone in all treatment groups after PRK. In most groups a return to full sensitivity was achieved by 6 months with the exception of the multizone treatment group which showed significant corneal hypoaesthesia at 12 months. Peripheral corneal sensitivity was also reduced in this group up to 3 months after the procedure. A comparison between the −3.00 D and −6.00 D treatment groups showed no significant difference. However, combining data from all treatment groups, a significant correlation was found between the interocular difference in central corneal sensitivity and postoperative haze at 3 and 6 months.
CONCLUSIONS For corrections up to −6.00 D ablation depth and treatment zone diameter do not appear to be clinically important determinants of corneal hypoaesthesia. In contrast, postoperative corneal haze appears to correlate with sensitivity loss.
- photorefractive keratectomy
- corneal sensitivity
Statistics from Altmetric.com
Varying degrees of postoperative corneal hypoaesthesia have been described following a variety of refractive surgical procedures. Epikeratophakia is associated with a marked reduction in corneal sensitivity.1-3 Corneal touch thresholds within the donor lenticle are increased as long as 3 years after the procedure.3 Surprisingly there is also a mild loss of peripheral corneal sensitivity during the first postoperative year, presumably due to retrograde neural degeneration.3 Studies of corneal sensitivity after radial keratotomy (RK)3-4have produced equivocal results. Shivitz and coworkers4found increased touch thresholds for up to 1 year after RK but, in contrast, a recent study3 reported that corneal sensitivity was unaffected by radial corneal incisions.
Recently attention has been directed at the use of argon/fluoride excimer lasers as a means of permanently altering the corneal profile. Compos and coworkers5 were the first to investigate corneal sensation following excimer photorefractive keratectomy (PRK). They showed that corneal sensitivity was significantly depressed during the first few postoperative months; however, in the vast majority of cases corneal sensation had returned to normal by 6 months. Recent studies56 have suggested that the extent and duration of corneal hypoaesthesia is dependent on ablation depth. Following deep (>30 μm) ablation both central and peripheral (unablated) corneal sensitivity were reduced compared with a group receiving shallow ablations (<30 μm) Kohlaas et al 3reported that a small group of patients with severe subepithelial haze appeared to have a delayed recovery of sensitivity.
The aim of the present study was to investigate the effects of ablation depth and treatment zone diameter on central (ablated) and peripheral (unablated) corneal touch sensitivity which was measured using a Cochet-Bonnet aesthesiometer.
Materials and methods
SUBJECTS
Fifty patients were recruited from volunteers over the age of 24 with stable myopia of approximately −3.00 D or −6.00 D and with astigmatism less than 1.50 D. Exclusion criteria included diabetes and connective tissue disorders. A thorough screening examination excluded subjects with any ocular pathology. All patients were extensively counselled and gave their informed consent. Demographic details of patients are given in Table 1.
Demographic and beam configuration data
TREATMENT GROUPS
Twenty patients received −3.00 D PRK. These were randomly allocated to two treatment zone diameters—5 mm and 6 mm. Thirty patients received −6.00 D PRK, randomly allocated into three diameters, 5 mm, 6 mm, and multizone. The multizone ablation was a two stage procedure consisting initially of a 4.6 mm −5.00 D correction immediately followed by a 6 mm −1.00 D correction which was concentric with the first. This resulted in a 6 mm ablation having the depth of a 5 mm treatment but with a more tapered periphery.
SURGICAL PROCEDURE
All patients were treated by the same surgeon using a Summit Technology Omnimed laser (emission wavelength = 193 nm, fixed pulse repetition rate = 10 Hz, radiant exposure = 180 mJ cm−2). Ablation profiles were determined by computer controlled expansion of the aperture of an iris diaphragm. Details of surgical procedure and postoperative regime are presented elsewhere.7
ASSESSMENT OF HAZE
Haze was assessed objectively as described previously.8 Briefly, a video image of a corneal slit section was captured using a frame grabber and haze quantified by computer analysis in grey scale units.
ASSESSMENT OF CORNEAL SENSITIVITY
Corneal sensitivity (CS) was determined using a slit-lamp mounted Cochet-Bonnet aesthesiometer (Fig 1). This instrument, which is essentially a modification from an original description by Boberg-Ans,9 was mounted on a slit-lamp biomicroscope to allow smooth and accurate stimulus application.10 The Cochet-Bonnet stimulus consists of a nylon filament which can be varied in length from 0 to 6 cm. The force exerted by the nylon, when the filament touches the cornea is inversely proportional to its length. Sensitivity was determined for treated and untreated (control) eyes before and at 1, 3, 6, and 12 months after PRK. For each eye five corneal locations were assessed These included three paracentral points, which for the treated eyes lay within the ablated zone, and two peripheral points (one inferior and one temporal) located 1 mm in from the limbus. The procedure for measuring CS was as follows. The patient was asked to indicate when the stimulus was felt; the filament, which was held in constant focus through the slit-lamp binocular, then approached the cornea smoothly and perpendicularly using its corneal reflection to determine proximity to the cornea; contact was detected by the slightest bend of the nylon; CS was taken as the length of filament which gave a 50% positive response from a minimum of four stimulus applications; subject reliability was tested by bringing the filament close to the cornea without actually touching.
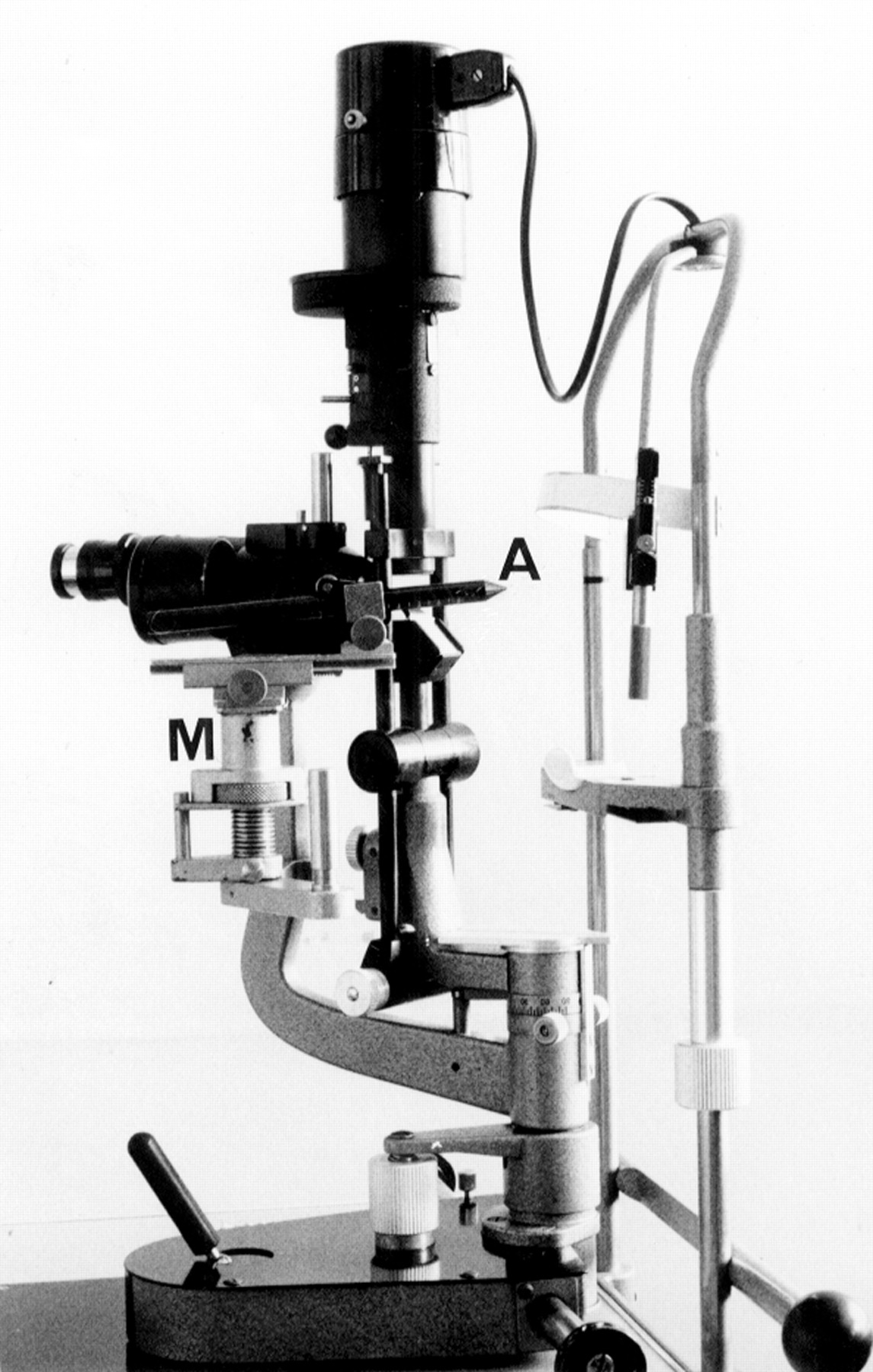
Shows the slit-lamp mount (M) for the Cochet-Bonnet aesthesiometer (A). This allows control over filament orientation in the XYZ planes.
Several subjects continued to wear a soft contact lens in the untreated eye during the postoperative period. They were instructed not to wear the lens on the day of examination to allow for recovery of the small sensitivity loss due to soft lens wear.11
STATISTICAL ANALYSIS
Statistical analysis was carried out using spss for Windows. Mean central CS was calculated from the three paracentral points and mean peripheral CS from the two peripheral points. The mean central and peripheral differences in CS between eyes at each time point were then compared with the differences preoperatively using a Wilcoxon signed ranks test. Intergroup comparisons were made using a Mann–Whitney test. A Pearson rank correlation was used to analyse the effects of haze on hypoaesthesia.
Results
Mean preoperative CS for all subject groups is given in Tables 2and 3. In order to show the temporal variation in CS after surgery, the interocular differences in CS between the treated and control eyes were plotted against time after laser ablation (Figs 2 and 3). Both −3.00 D treatments (5 mm and 6 mm) showed a similar temporal variation in sensitivity. In each case there was significant hypoaesthesia compared with preoperative levels within the central ablated zone up to 3 months after surgery (Table 4). Corneal sensitivity thereafter returned to baseline levels. In contrast, with the exception of the 6 mm group at 1 month, peripheral corneal sensitivity was unaffected in patients undergoing −3.00 D ablations.
Baseline (preoperative) sensitivity values for −3.00 D corrections
Baseline (preoperative) sensitivity values for −6.00 D corrections

Mean difference in corneal sensitivity (CS) between control and treated eyes plotted against time after PRK for (A) 5 mm and (B) 6 mm −3.00 D treatments (*represents statistically significant hypoaesthesia).

Mean difference in corneal sensitivity (CS) between control and treated eyes plotted against time after PRK for (A) 5 mm, (B) 6 mm, (C) multizone −6.00 D treatments (*represents statistically significant hypoaesthesia).
Statistical analysis for −3.00 D corrections. The treated eye was compared with the fellow eye at each time point using a Wilcoxon signed rank test
Both 5 mm and 6 mm −6.00 D treatments showed similar levels and durations of central corneal hypoaesthesia to the −3.00 D groups. However, in the case of the −6.00 D multizone treatment a significant loss of central corneal sensitivity was observed at each time point after surgery. Moreover, in this group peripheral sensitivity was significantly reduced over the same timescale (Table5).
Statistical analysis for −6.00 D corrections. The treated eye was compared with the fellow eye at each time point using a Wilcoxon signed rank test
Comparisons of differences in mean CS between the −3.00 D and −6.00 D treatment groups were not significant for central or peripheral cornea (p>0.05).
There was a significant correlation between objective haze and interocular difference in CS at 3 months (r= 0.3121, R2= 0.096, p=0.027) and 6 months (r= 0.5318, R2= 0.2828, p = 0.0001), but not at 12 months. Scatter plots are illustrated in Figure 4.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Scatter plots showing the relation between subepithelial haze and interocular difference in corneal sensitivity (CS) at (A) 3 months and (B) 6 months postoperatively. Scatter plots showing relation between objective subepithelial haze and corneal touch threshold.
There was no correlation between loss of corneal sensitivity and residual refractive error.
Discussion
The innervation of the cornea derives predominantly from ciliary branches of the ophthalmic division of the trigeminal nerve, which enter the cornea radially at mid stromal level and divide repeatedly as they pass superficially to contribute to a rich plexus of nerves immediately under Bowman’s membrane. The epithelium receives its supply of terminal axons from this plexus via branches through Bowman’s membrane.12 This particular neural arrangement would explain the hypoaesthesia observed after PRK in this and in other studies.56 The surgical procedure in PRK involves mechanical debridement of the epithelium followed by ablation through the subepithelial plexus. It therefore results in significant neural loss. The degree of damage to deeper stromal nerves is dependent on ablation depth. The present study showed that in most cases a return to preoperative sensitivity levels occurred within the first 6 months postoperatively. This would suggest prolific nerve regeneration. A recent study of nerve regrowth after PRK in rabbits13 has detected regenerating axons as early as 24 hours after the procedure, and showed a reformed subepithelial plexus after 4 months. However, confocal imaging of the human cornea after PRK failed to detect subepithelial nerves in the central area up to 2.5 years after treatment.14 This is surprising in view of the rapid restoration of sensitivity observed in this and other studies. A return of touch sensitivity appears to be dependent on the re-establishment of a normal epithelial nerve pattern.15 The inability of confocal imaging to detect such nerves may be due to a limitation in the resolving power of the confocal microscope or regenerating axons may have a similar refractive index to the surrounding tissue. These factors may therefore cause a significant underestimation of the degree of neural regeneration post-PRK.
In contrast with a previous study6 we did not find a significant relation between corneal hypoaesthesia and ablation depth. Regenerating neurons after PRK and anterior stromal keratectomies derive from the subepithelial plexus adjacent to the wound margin as well as from deeper stromal fibres.13-17 Although greater stromal nerve damage would be expected with deeper ablations, reinervation from the subepithelial plexus would be independent of ablation depth. Animal studies of reinervation following keratectomy demonstrate a prolific neurite outgrowth from the subepithelial plexus during the first month after surgery. These axons make a major contribution towards epithelial terminal density.17
In the present study the longest duration of hypoaesthesia occurred after the −6.00 D multizone treatment. This group showed a significant reduction in central corneal sensitivity 1 year after surgery. The reason for this loss in sensitivity is unclear. However, several subjects after the multizone treatment showed severe and persistent subepithelial haze which may have been a determining factor in the delayed recovery of this group. The present study found a significant linear correlation between haze and corneal hypoaesthesia. Since residual refractive error did not show the same relation, changes in epithelial thickness are unlikely to explain the sensitivity loss. An alternative explanation is that alterations in the extracellular matrix which occur in corneal remodelling may exert an influence on neural regeneration.
Glycosaminoglycans (GAGs) have been shown to inhibit neurite outgrowth in vitro.18 The degree of inhibition appears to be dependent on the type and concentration of the GAGs. The inhibitory effect was reduced with appropriate concentrations of neurotrophic factors. Since altered synthesis of GAGs occurs in corneal scar formation19 the interplay between these molecules and the levels of neurotrophic factors may be important in determining the time course of reinervation and the subsequent recovery of tactile sensitivity.
In terms of the clinical significance of the findings it can be concluded that, with the exception of a minority of patients showing severe haze, the observed corneal hypoaesthesia after PRK is small and in the majority of cases shows a rapid return to preoperative levels. Furthermore, the ablation depth does not appear to be a major determinant in corneal sensitivity loss for corrections up to −6.00 D.
Acknowledgments
We thank the Williams Fellowship for Medical and Scientific Research, University of London (to MCC) and the Iris Fund for the Prevention of Blindness