Article Text

Abstract
AIMS/BACKGROUND Proton beam radiotherapy can effectively treat primary uveal melanomas of any size. Some patients, however, develop adverse late effects following treatment and the purpose of this study was to determine which factors give rise to a poor local outcome.
METHODS The hospital records from a first cohort of 127 patients treated by protons from 1989 to 1992 were reviewed retrospectively. The presence of rubeosis was selected as a measure of significant ocular damage. Split file analysis was performed with 73 cases forming a test group with the remaining 54 cases acting as a validation group.
RESULTS Large tumour size and the presence of retinal detachment were significant, independent risk factors for developing rubeosis for both the test and validation groups. These factors also predicted subsequent enucleation for uncontrolled ocular pain. Patients with tumours too large to plaque and with an associated retinal detachment had a 90% chance of developing rubeosis within 4 years of proton beam radiotherapy.
CONCLUSIONS Patients with a uveal melanoma too large for plaque therapy and an associated retinal detachment run a very high risk of developing rubeosis after proton beam radiotherapy and one third of individuals developing rubeosis required enucleation for pain even if local tumour control was satisfactory.
- proton beam radiotherapy
- predictive factors
- rubeosis
- uveal melanoma
Statistics from Altmetric.com
Charged particle radiotherapy, either with protons or helium ions, is an effective treatment for uveal melanoma. No difference in survival has been reported for patients treated by charged particles and those whose eye is enucleated1 or who undergo brachytherapy using radioactive scleral plaques.2 Local tumour control rates after proton therapy are excellent with published series reporting local recurrence rates of 1.9%3 or less.1 Ocular radiotherapy is not without morbidity,45 however, and charged particle therapy is no exception6-12 with the side effects including eyelid damage, defective tear production and drainage, keratitis, cataract, scleral and corneal necrosis, radiation retinopathy and optic neuropathy, retinal detachment, glaucoma, iris rubeosis, and phthisis. Enucleation rates as high as 13% have been reported for treatment associated morbidity following particle beam radiotherapy.11
All of the major therapeutic modalities for ocular melanoma are available to patients treated in the Ocular Oncology Services at Moorfields Eye Hospital and St Bartholomew’s Hospital, London. Patients are therefore selected for the various treatment options according to the clinical characteristics of their melanoma and their general health status and wishes and not on the basis of availability of therapeutic techniques. At the time of introduction of proton therapy in London, and therefore during the study period, the major tumour factors influencing selection were size and location. Proton beam radiotherapy was recommended for tumours which were either too large or considered too close to the optic disc or nerve for brachytherapy by radioactive scleral plaque. Early in the study period we recognised that eyelid damage was severe after treatment of anteriorly located melanomas because the superficial sparing effect of the Bragg peak of protons was absent for such tumours. This effect was compounded by increasing modulation of the Bragg peak required to treat large melanomas and was especially troublesome when corneal toxicity followed damage to the upper eyelid after treatment of large, superiorly located tumours. Eyelid damage could be predicted on the basis of the tumour factors documented during the initial evaluation and treatment selection process and from an early stage proton beam radiotherapy was not recommended in London for patients at significant risk of this adverse effect. Nevertheless, we continued to observe a high morbidity rate, particularly in patients undergoing proton therapy for melanomas which were too large for plaque therapy. After treatment, many of these patients had chronically painful and cosmetically unsatisfactory eyes with a significant minority requesting subsequent enucleation for persisting symptoms of pain and irritation.
We therefore decided to perform a retrospective analysis of our first cohort of proton treated patients to see if we could identify risk factors for subsequent morbidity which, like those for eyelid damage, could be determined at the initial assessment. Our aim was to avoid subjecting patients to proton therapy if they were likely to suffer significant morbidity as a result of their treatment. We chose the presence of iris rubeosis as a marker of severe ocular damage because we had noted that all eyes enucleated for treatment associated morbidity had this feature and that neovascular glaucoma is stated in the literature to be the most common cause for subsequent enucleation.613
Materials and methods
PATIENTS
The present series comprised the first cohort of patients treated by proton beam radiotherapy from Moorfields Eye Hospital and St Bartholomew’s Hospital, from May 1989 to November 1992. The diagnosis was based on indirect ophthalmoscopy, supported in every case by B-scan ultrasonography and, where appropriate, by fluorescein angiography. The minimum follow up period was 24 months for all surviving patients and the median follow up period was 36 months. During the study period 127 patients were treated and complete information was available on 125 cases (missing data were handled in a leastwise manner). There were 81 males and 46 females whose ages ranged from 19.5 years to 82.7 years (mean 56.6 years, median 59.2 years). Melanoma was unilateral in every case and there were 64 right eyes and 63 left eyes.
METHODS
Proton beam radiotherapy was administered at the Douglas Cyclotron, Clatterbridge. Patients were treated and followed according to a strict protocol as part of a phase 2 study funded by the Imperial Cancer Research Fund and the Medical Research Council. All patients first underwent insertion in London of at least four radio-opaque tantalum markers. These were sutured to the sclera at known distances from the tumour edge in order to allow precise tumour localisation for the treatment. The clips are completely inert and were left in place after radiotherapy. The treatment plan treated to the tumour edge plus a surrounding 2 mm safety margin. Radiotherapy was administered between 2 and 4 weeks after the insertion of the markers to eliminate any error resulting from maldistribution of the beam in tissue due to post-surgical swelling. A total dose of 52 cobalt Gray equivalents was given in four equal fractions over 4 days. Following radiotherapy, all patients were treated with topical dexamethasone 0.1% four times daily and cyclopentolate 1% twice daily for 4 weeks.
Patients with adequate tumour control who developed rubeosis were initially managed medically with topical cycloplegics and steroids as well as short term systemic carbonic anhydrase inhibitors. Where long term carbonic anhydrase inhibitors were required, preferred management was by cyclocryotherapy in the earlier part and cyclodiode laser therapy in the later part of the series. Only when this approach failed to control pain secondary to raised pressure or when tumour control was deemed inadequate was enucleation advised.
The patients’ hospital records were reviewed retrospectively. Data were collected on 22 clinical variables from the presenting visit. In addition, any adverse outcomes were also recorded including time to death, time to rubeosis, and time to, and indication for, enucleation where appropriate. Three variables showed no variation: no patients had rubeosis at presentation, none was on topical medication, and none had limbal injection. For a further three variables there was only one case positive for each; these were presence of pain, presence of keratic precipitates, and the presence of local extrascleral extension. A fourth variable, the presence of cataract, was present in only four cases. Variables which showed either no or insignificant variation were excluded, leaving 15 variables which are summarised in Table 1. Two of these 15 variables, anterior chamber cells and flare, were clearly co-correlated so were combined under a 16th heading, iritis (Table1).
Summary of the information collected for the predictor variables and how they were recorded
We performed split file analysis. The allocation into test and validation groups was made before performing any analyses. The test group comprised 73 cases and the validation group 54 cases.
Results
Of the 127 study patients, 43 (34%) developed rubeosis. Seventeen patients (13%) required subsequent enucleation and 16 died (13%) from metastatic disease within the study period.
ANALYSIS FOR THE DEVELOPMENT OF RUBEOSIS
The initial analysis for the predictor variables was confined to the 73 cases of the test group. The dichotomous variables, anterior chamber invasion, sex, side, and vitreous haemorrhage were specified as binary indicator variables for the analyses. A multivariate Cox’s proportional hazard model was constructed using a forward stepwise procedure and performed on the basis of the likelihood ratio statistic (probability for entry into the model of 0.04 or less and probability value for removal of 0.05 or greater). The model is summarised in Table2. The only two variables which appeared in the model were largest tumour diameter (LTD) and the presence of retinal detachment. Data for the validation group were collected and recorded in an identical manner. The Cox’s proportional hazard model was repeated with almost identical results (Table 3).
The results of the Cox’s proportional hazard model using forward selection on the basis of the likelihood ratio statistic for the test group
The results of the Cox’s proportional hazard model using forward selection on the basis of the likelihood ratio statistic for the validation group
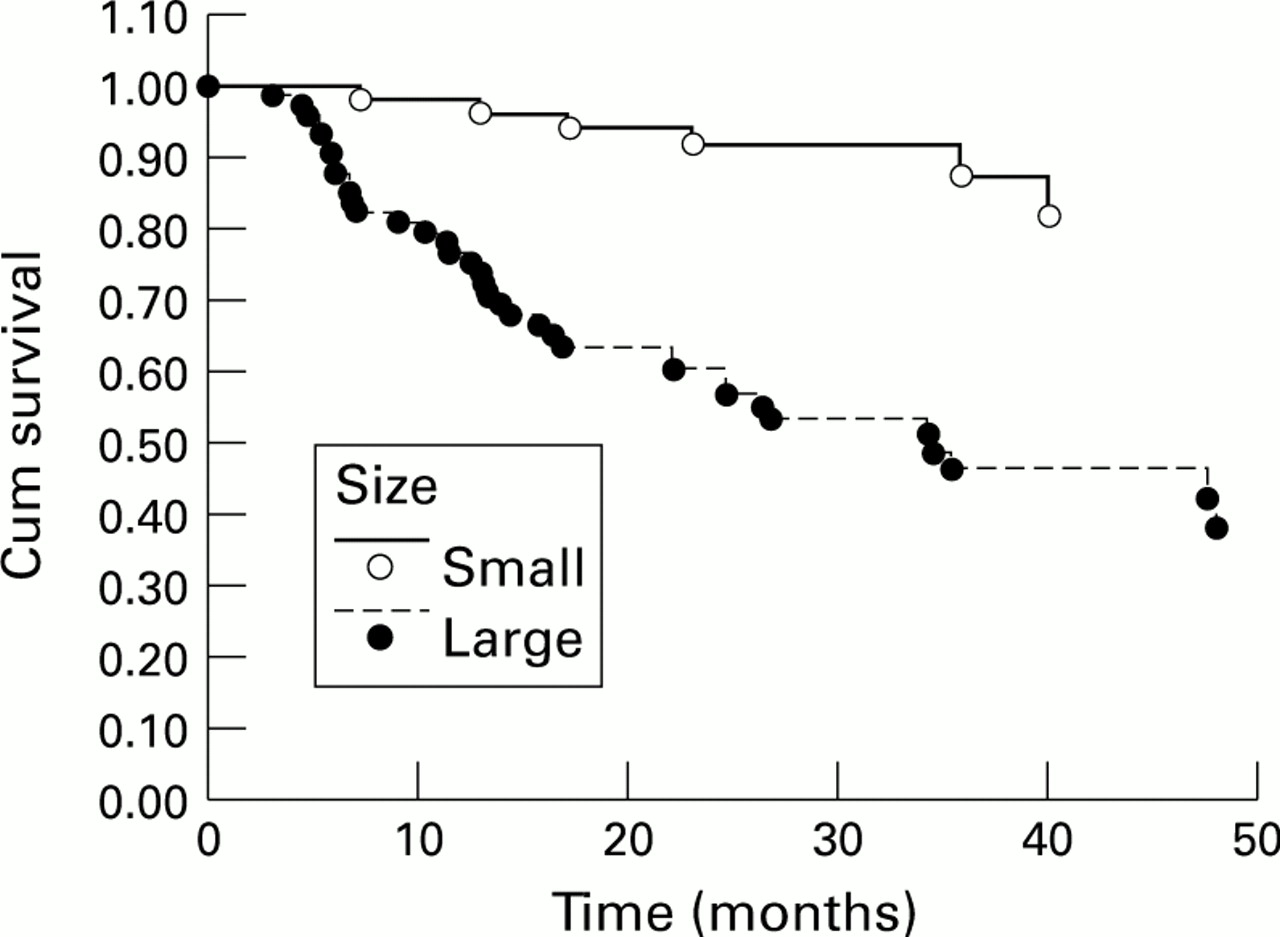
As the analyses from the test and from the validation groups agreed, the two groups were merged to form a single large group and the analyses re-run. The univariate statistics are summarised in Table 4and the final model in Table 5. The two variables that proved to be consistently predictive for the development of rubeosis were LTD (see Fig 1) and the presence of retinal detachment (see Fig 2). The presence of lipofuscin and anterior location of the tumour (determined by location 1 and location 2 in Table 1) were both highly significant on univariate tests but did not appear in the final model because these variables co-correlate with tumour size. The reasons for the co-correlation are as follows. All anterior tumours had been selected for protons because they were too large to plaque. By contrast, some posterior melanomas were small enough to plaque but had been selected for protons because of their juxtapapillary location. Presence of lipofuscin also incorporated a measure of size as it included information on the presence of a collar stud growth pattern in which orange lipofuscin cannot usually be detected (Table1).
The univariate statistics, using the proportional hazards model, for the variables predicting rubeosis for the merged groups
The results of the Cox’s proportional hazard model for predicting rubeosis for the merged groups.

Kaplan–Meier curves showing the effect of size on the subsequent development of rubeosis for the merged groups. Small refers to tumours smaller enough to be plaqueable and large means that they were too large for brachytherapy to be an option.

Kaplan–Meier curves showing the effect of the presence or absence of an associated retinal detachment for the subsequent development of rubeosis for the merged groups.
CONSTRUCTING A CLINICAL SCORE TO PREDICT RUBEOSIS
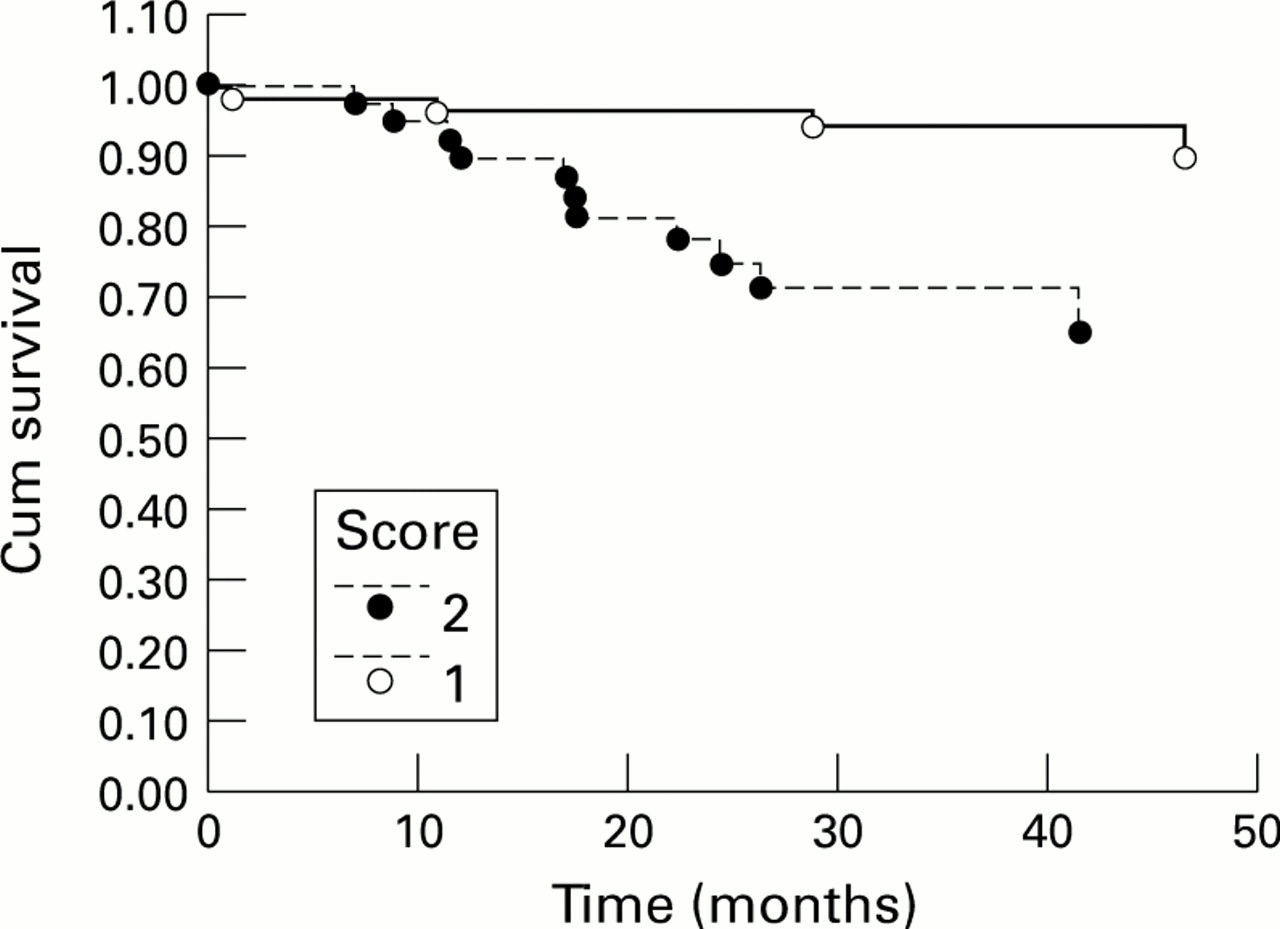
We constructed a clinical score to predict the development of rubeosis on the basis of the two predictive variables, LTD and presence of retinal detachment. For a system to be practical in clinical use, it must be simple and easy to remember. We took as a surrogate measure of size as whether the tumour was small enough to treat by plaque were it not for its location. In our practice this means a tumour up to 14 mm base by 5 mm height for a ruthenium-106/rhodium-106 plaque or 12 mm base by 8 mm height for an iodine-125 plaque. We chose these measures for size as they have to be determined routinely on all patients when assessing the treatment options. Retinal detachment was characterised as being either present or absent. These two simplified variables had very similar coefficients, of 1.6 for size and 1.4 for retinal detachment, when the two were entered together in a Cox’s model and so were given equal weights in the scoring system. We gave one point for a tumour too large to be treated by plaque and another point to presence of a retinal detachment visible on indirect ophthalmoscopy. The total score is marked out of 2 and is the sum of these two variables. This simple scoring system divided our patients into three groups of nearly equal size. Thirty five eyes scored 0, 52 scored 1, and 40 scored 2. This scoring system was highly predictive for the subsequent development of rubeosis (log rank test, p<0.00005) with 35/40 (88%) of cases scoring 2 developing rubeosis by 4 years compared with 19/52 (37%) scoring 1 and 3/35 (9%) scoring 0 (see Fig3).

Kaplan–Meier curves showing the predictive effect of the 2 point scoring system for the subsequent development of rubeosis for the merged groups.
ANALYSIS FOR SUBSEQUENT ENUCLEATION
Fifteen patients underwent enucleation as a result of treatment related morbidity and one underwent enucleation for failure to control the primary tumour (and this case was handled as a censored observation for the subsequent analyses). This number of events was too small to justify a multivariate analysis. Univariate testing, using Cox’s proportional hazards model showed that the presence of a retinal detachment was predictive of subsequent enucleation for morbidity (p=0.006) and tumour size approached significance (p=0.07). We therefore tested our scoring system for predicting subsequent enucleation for morbidity. There were 0/35 enucleations for the cases scoring 0, 4/52 for the cases scoring 1, and 11/40 for the cases scoring 2 and this was highly significant (log rank test, p=0.0001) (Fig 4).
Kaplan–Meier curves showing the predictive effect of the 2 point scoring system for subsequent enucleation for morbidity for the merged groups.
SURVIVAL ANALYSIS
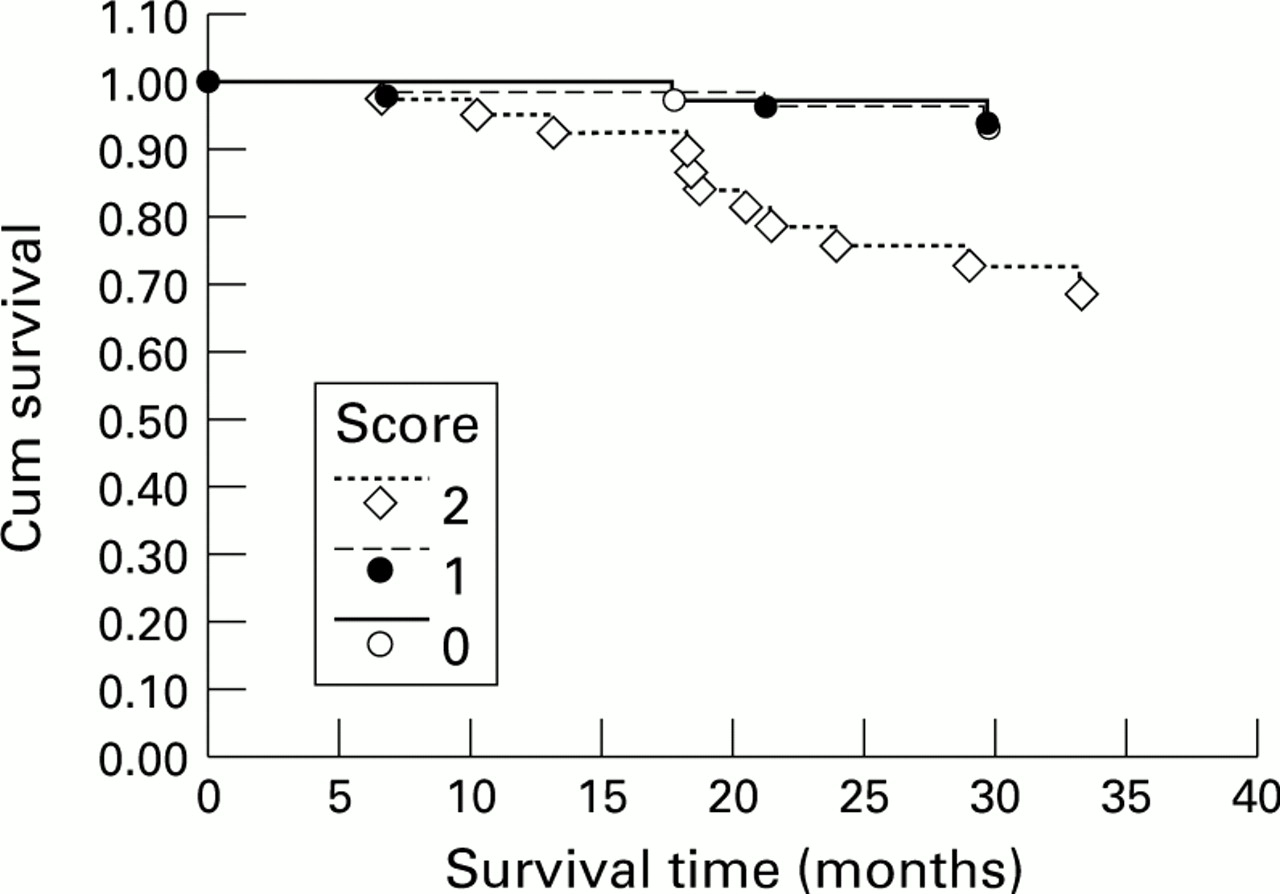
There were 16 tumour related deaths. This number was also too small to justify full multivariate modelling. However, it was noted on univariate testing with the proportional hazards model that both the largest tumour diameter (p=0.0006) and retinal detachment (p=0.008) were predictive of metastatic spread. We therefore tested to see if the two point scoring system could predict metastatic disease. There were two deaths out of 35 patients scoring 0, 4 out of 52 scoring 1, and 11 out of 40 scoring 2 (log rank test p=0.0016) (Fig 5).

Kaplan–Meier curves showing the predictive effect of the 2 point scoring system for subsequent tumour related death for the merged groups.
Discussion
Our analysis revealed that the significant factors for predicting rubeosis following proton beam radiotherapy were the presence of retinal detachment and large tumour size. We performed split file analysis and these factors were significant in both the test group and the validation group. The final analysis was performed on the whole cohort of patients.
There are several possible mechanisms for the development of rubeosis after radiotherapy for intraocular tumours. Rubeosis is known to be a response to ischaemia. A long term effect of radiation is damage to blood vessels. If radiation induced retinal ischaemia is a determinant of rubeosis after proton beam radiotherapy it is not surprising that large tumour volume is a risk factor since the total dose of radiation received by the eye is proportional to tumour volume. Chronic retinal detachment is also a known cause of iris rubeosis and this effect may similarly depend on retinal ischaemia. It is not unexpected, therefore, that tumour associated retinal detachment is an independent risk factor for rubeosis after proton treatment and that this effect is additive to that of tumour size. A further possible determinant of rubeosis is the release from the irradiated tumour of humoral factors which stimulate neovascularisation. Rubeosis is also seen after irradiation of other vascular tumours including metastatic carcinomas, retinoblastomas, and benign vascular lesions such as retinal capillary haemangiomas. The common factors when rubeosis occurs after treatment of these other tumours seem to be retinal detachment together with a high total dose of radiation and large fraction size similar to those employed in the treatment of melanoma. Any angiogenic effect is therefore unlikely to be specific to melanoma or as potent as the effects of simple ischaemia whether induced by radiation or by retinal detachment.
Each of the two significant factors can be ascertained at the presenting clinic visit when treatment method is chosen. We were able to construct a scoring system in which a tumour too large to treat by plaque and the presence of a retinal detachment each score one point. Marked out of a maximum score of 2 points, this practical scoring system divides the patients into three nearly equal sized groups and is strongly predictive of subsequent development of rubeosis, loss of the eye from late morbidity, and development of metastases. Thirty two per cent of our tumours scored 2 and this group had nearly a 90% chance of developing rubeosis, a 27.5% chance of dying, and a 27.5% chance of requiring enucleation by 4 years.
Our analysis reached slightly different conclusions from that performed by Egan and colleagues in Boston, USA.13 In their study there were 64 enucleations from 994 cases but one major methodological difference was that these authors did not separate eyes enucleated for failure to control the primary tumour from eyes enucleated as a result of complications. The underlying factors are probably very different in the two situations: enucleation for failure of local control of the ocular primary is due either to tumour radioresistance or targeting error when delivering the treatment,1113 whereas enucleation for complications depends upon large tumours size and the presence of a retinal detachment. In the Boston series, 75% of enucleations were performed for complications and 25% for failure of local tumour control. Consequently, treatment associated morbidity was the major end point measured. The three major factors in the Boston model for predicting enucleation were tumour height, anterior tumour margin involving the ciliary body, and posterior margin within two disc diameters of the fovea. These last two factors seem slightly contradictory and they may be acting as surrogate measures for tumour size since large tumours are more likely to involve a particular structure than small ones. In their Cox’s model, however, the presence of a retinal detachment was also a significant risk factor for subsequent enucleation, with a relative risk of 1.7 and 95% confidence interval of 1.1–2.7. Thus our analyses are in broad agreement.
A study from San Francisco, USA by Kim and colleagues6investigated the risk of developing neovascular glaucoma. Again size was the predominant risk factor. The presence of subretinal fluid was not a significant risk factor in the San Francisco study.
Our simple scoring system would also appear to be of possible prognostic significance, though this was not the major aim of this study. Tumour size is a well established risk factor for metastasis from uveal tract melanoma13-17 and this has been confirmed for cases treated by charged particle radiotherapy.1819 Although retinal detachment is not a well recognised risk factor, its significance is not surprising since the presence of subretinal fluid is an established marker of disease activity predicting subsequent enlargement of suspicious choroidal naevi.2021 The subgroup scoring 2 not only sustain local morbidity following proton beam radiotherapy, they also have a high mortality rate. Nearly one third of these patients had died within 3 years. We would expect the 10 year mortality rate for this subgroup to exceed 50% and to approach 80% if they follow published survival curves for high risk cases.
Our study complements the report from Char and colleagues2who compared the results of treating small and medium sized tumours treated either by iodine-125 plaque or by charged particle therapy using helium ions. Both arms of this study did well and there was no difference in the rates of developing metastatic disease. The complication rate was significantly higher for charged particle radiotherapy than for plaque therapy and, in particular, the rate of severe visual loss was higher in the helium ion treated group than in the group treated with iodine-125 plaque radiotherapy. The local tumour control rates, however, were significantly better after charged particle therapy. Taking our results in conjunction with Char et al’s, it is apparent that eyes with melanomas small enough to treat by brachytherapy will do similarly well with charged particle therapy. Furthermore, we have shown that tumours too large to treat by plaque but with no retinal detachment did well with proton beam radiotherapy. Morbidity is unacceptable, however, following proton therapy of melanomas which are too large to plaque and which also have an associated retinal detachment. In our opinion, tumours in this category are best treated by local resection where it is possible and enucleation where it is not. In the future, combinations of radiotherapy, either by plaque or by protons, with other treatments such as hyperthermia may enable us to treat larger tumours by radiation than is currently possible. It remains to be seen whether such treatments will have fewer side effects than proton beam radiotherapy. It is possible that the success of local resection depends substantially on the relatively rapid resolution of the retinal detachment that the operation brings about. Conversely, it may be the very slow resolution of retinal detachment following proton therapy compared even with plaque therapy for tumours of a similar size that leads to rubeosis. If combined treatments can speed resolution of the detachment then at least one of the risk factors for rubeosis will have been eliminated and there is reason to hope for better outcomes.
We present a simple flow diagram summarising our conclusions for treatment (Fig 6). We have not investigated local resection in this study. Resection has the advantage that good visual acuity can be retained22 but the technique is not free from complications. There is concern over the morbidity associated with profound hypotensive anaesthesia with a reported 4% incidence of strokes following the anaesthetic23 and at least one reported anaesthetic death.24 Approximately one third of patients develop retinal detachments following surgery.22There is also the problem of local recurrence25 with the concern that this may adversely affect survival,26 though no difference in mortality rate was noted in a large study involving matching cases treated by either local resection or enucleation.27 The only study directly comparing tumours treated by local resection and brachytherapy found an increased morbidity in the local resection treated group.28

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A clinical algorithm summarising how we propose uveal melanoma should be treated. The numbers refer to how the cases described in this paper fit into the proposed algorithm.
There is no evidence that survival rate is influenced by the different method chosen for treatment of uveal melanoma. Rational selection criteria for conservative therapy should therefore depend upon the inter-relation between the clinical features of a melanoma and the morbidity associated with the available treatment modalities. This study has shown that rubeosis following proton beam radiotherapy depends on the tumour characteristics and that the outcome in terms of morbidity and possibly also of mortality can be predicted by a simple clinical scoring system based on the clinical features at presentation.
Acknowledgments
This study was funded in part by the Imperial Cancer Research Fund and the Medical Research Council. Additional financial support was provided by Mrs Helen Agrawal.