Article Text

Abstract
AIMS The effect of transpupillary thermotherapy (TTT) on human choroidal melanomas was investigated by means of histopathology.
METHODS Before enucleation TTT was performed in 11 eyes with a xenon arc photocoagulator with a red filter or a diode laser at 810 nm. The exposure time was 1 minute; the estimated temperature at the top of the tumour was about 65°C.
RESULTS Seven of 11 tumours developed necrosis to a maximum depth of 3.9 mm with a sharp demarcation between the necrotic and the viable part of the tumour. The depth correlated with penetration of heat into the tumour. Scattered small haemorrhages in the transitional zone between the necrotic and the viable part of the tumour were observed in three eyes but large haemorrhages were absent. Ocular media were not affected owing to the low rate of absorption of radiation at 810 nm. TTT did not cause significant scleral damage. Intrascleral tumour cells with a viable appearance were observed in one eye, where the tumour was almost totally necrotic.
CONCLUSION Results show that TTT has potential as a conservative therapeutic treatment for choroidal melanomas.
- hyperthermia
- choroidal melanoma
- histopathology.
Statistics from Altmetric.com
Enucleation as treatment of choroidal melanomas is partly replaced by radiotherapy with charged particles or brachytherapy with ruthenium-106 or iodine-125. Irradiation is associated with failures and complications since approximately 50% of eyes develop late complications after brachytherapy.1 2
Hyperthermia is used to treat malignant tumours, including melanomas, because of its synergistic action with radiation.3-5 It is generally performed at tumour temperatures below 43°C and exposure times of 30 minutes or more; under these conditions it has limited potential as sole means of destroying tumour cells but it does enhance the effect of radiotherapy. For treatment of choroidal melanomas hyperthermia is applied by means of microwave,6-9 localised current field,10 11ultrasound,12-14 and ferromagnetic thermoseeds.15 With these trans-scleral techniques hyperthermia does not cause permanent damage to normal tissue.16 17
Hyperthermia at a tumour temperature of 45°C or more can be designated as thermotherapy since after application for 1 minute it exerts an irreversible destructive effect on cells for which it does not require additional radiotherapy or cytostatic drug therapy.18-20 The application of thermotherapy at more than 45°C in clinical oncology is restricted since it affects both malignant and normal cells. In ophthalmology, however, thermotherapy by means of transpupillary infrared radiation can be used to treat choroidal melanomas19 because the rate of absorption at 810 nm is low for clear ocular media.21
This paper deals with the histopathological findings in human choroidal melanomas enucleated after transpupillary thermotherapy.
Material and methods
Eleven patients with large choroidal melanomas underwent transpupillary thermotherapy (TTT) by infrared irradiation before enucleation. We did not aim for total destruction of the tumour. Permission for the investigation was given by the medical ethics committee of Leiden University Medical Centre and informed consent was obtained from each patient after full explanation of the procedure. Before treatment the pupil was dilated with phenylephrine hydrochloride 5% and tropicamide 0.25% eyedrops. Immobilisation of the eye and anaesthesia to make the treatment painless were achieved with a retrobulbar injection of 2 ml prilocaine hydrochloride 2% (Citanest).
TTT was performed in four patients with a modified xenon photocoagulator (Zeiss, Oberkochen, Germany) with a red filter permitting 85% transmission between 780 and 880 nm.22 In seven patients we used a continuous wave diode laser (Nidek, Tokyo, Japan) which produced radiation at 810 nm via a handheld fibre in front of the eye. Both methods yield a beam diameter on the surface of the tumour of 2–4.5 mm. For the laser lens we used the panfunduscope (Rodenstock, Munich, Germany) or the Mainster lens (Mainster, Ocular Instruments, Bellevue, WA, USA). Because of variations in beam diameter the energy output was calculated in W/cm2 on the target area. We started the irradiation at the relatively low level of 3 W/cm2 and an exposure time of 1 minute. In the absence of an ophthalmoscopic effect we increased the energy level stepwise until the tumour exhibited a greyish discoloration as a result of tissue oedema developing during the 1 minute exposure. The maximum irradiance was 19 W/cm2 for the xenon photocoagulator and 12 W/cm2 for the diode laser. The interval between TTT and enucleation was 1 day in three patients, 2 days in five patients, and 3, 4, and 10 days, respectively, in the other three patients. After enucleation the eyes were fixed in buffered formaldehyde (10%), dehydrated in a series of alcohols and embedded in celloidin. Serial sections 17 μm thick were cut in a plane parallel to the light beam (Jung microtome, Heidelberg, Germany). Haematoxylin and eosin stained and some depigmented (KMnO4) sections were examined by light microscopy. Depth of tumour necrosis was measured with the aid of a grid.
Results
Data on tumour height and pigmentation, equipment used for TTT, diameter of the radiation beam, irradiance, radiant exposure, time interval between TTT and enucleation, and depth of tumour necrosis are summarised in Table 1.
Heat induced tumour necrosis in patients with choroidal melanomas treated with transpupillary thermotherapy (TTT) before enucleation
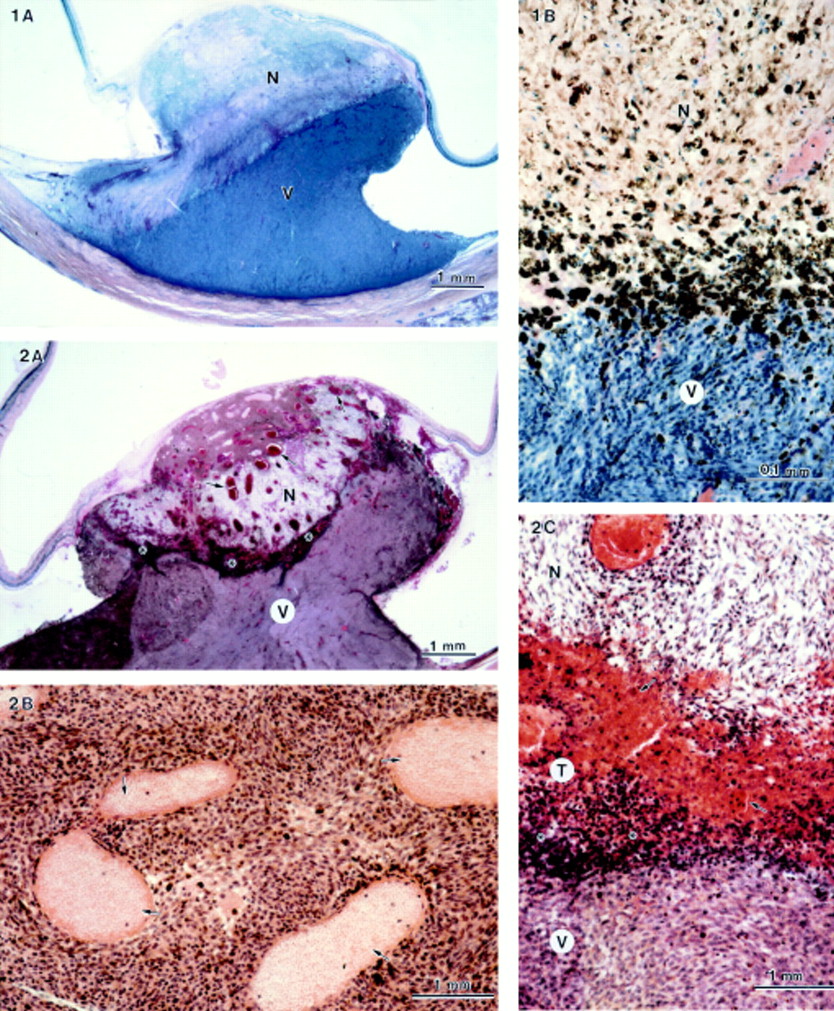
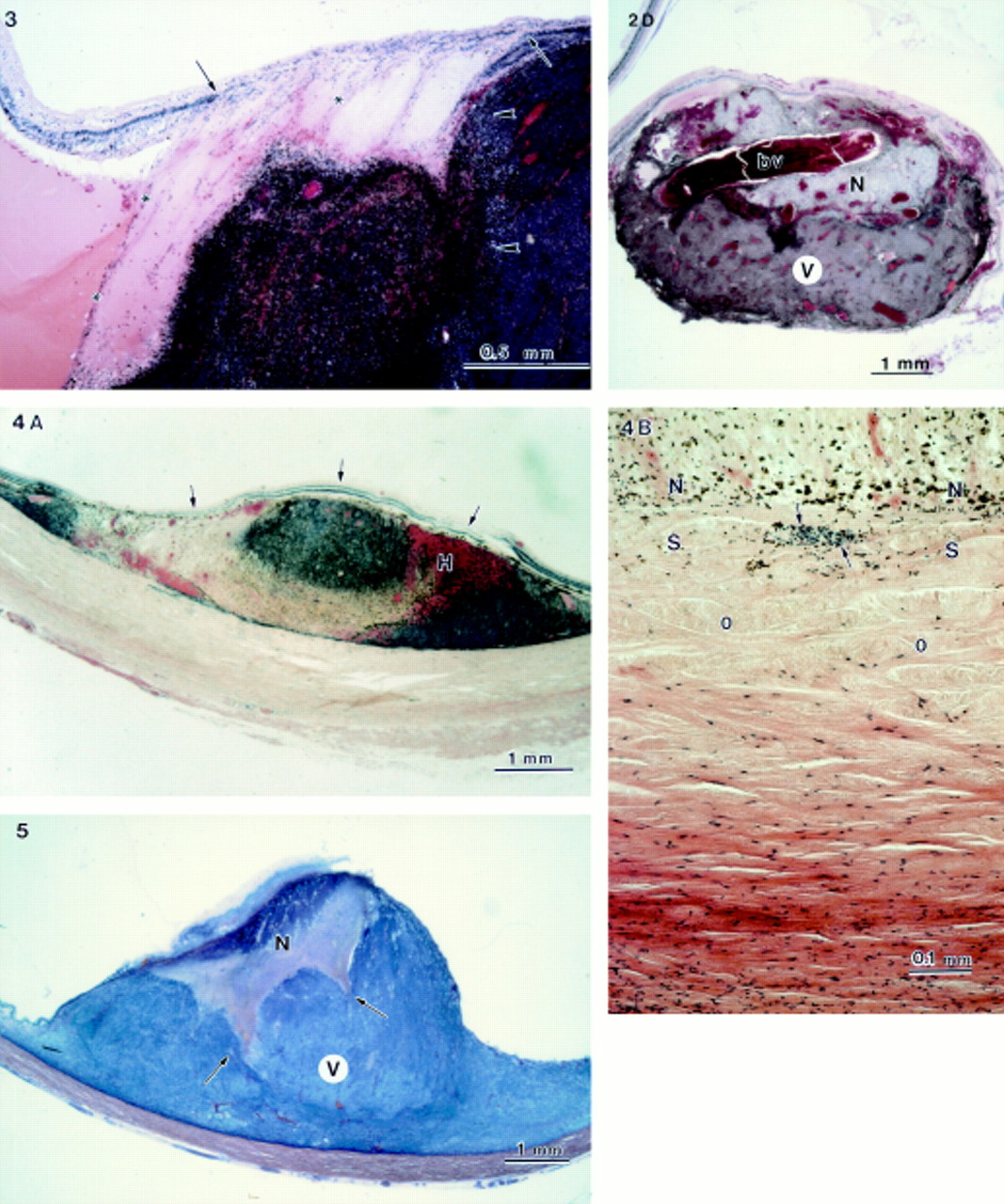
Tumour necrosis varying in depth between 1.3 and 3.9 mm was observed in seven of 11 melanomas. One eye was treated by xenon irradiation and enucleated 48 hours after TTT, the other six were treated with a diode laser and enucleated 48 hours to 10 days after TTT. The demarcation between the necrotic and viable parts of the tumour was sharply defined both in depth and in lateral direction (Figs 1–5). In two eyes (Nos 6 and 10) cones of necrotic tissue in between segments of viable tumour tissue were observed (Fig 5).
Four tumours (Nos 5, 8, 10, 11) contained two layers of necrosis, each with a different appearance of cell death (Figs 2A, 4A, 5). A superficial layer 0.7–2.2 mm contained tumour cells with shrunken nuclei, most of them without nucleoli, and loss of cytoplasm. All tumour vessels in this area were dilated and occluded by thrombi; some contained red blood cell ghosts (Fig 2B). Haemorrhages were absent.
The superficial layer was surrounded by a 0.7–1.9 mm zone of nuclear debris without cytoplasm and widened intercellular spaces. Also in this area vessels were occluded and even large vessels had not leaked erythrocytes (Fig 2D). In two patients (Nos 6, 11) some haemorrhages were observed in the peripheral part of the heat damaged area (Fig 4A).
A small transitional area of 0.15–0.7 mm could be seen between the necrotic and the viable part of the tumour with or without scattered small haemorrhages (Fig 2C).
Scleral damage was insignificant when the tumour necrosis bordered on the sclera. Heat penetration had caused some oedema but the scleral collagen retained its lamellar structure; sclerocytes had disappeared in this area but intrascleral tumour cells were present (Fig 4B).
In eight eyes retinal necrosis and atrophy in the TTT treated area were clearly separated from the surrounding normal retina (Fig 1A, 2A, 3, 4A).

(A) Patient 7. Depigmented haematoxylin and eosin stained section showing transpupillary thermotherapy induced necrosis (N) in a choroidal melanoma with a depth of 3.4 mm, sharply demarcated from the viable part (V) of the tumour without haemorrhages. Retinal necrosis and atrophy correspond with the area of necrosis of the tumour. (B) Haematoxylin and eosin stained section of the same eye as shown in (A) at higher magnification. Sharp demarcation between necrotic (N) and viable (V) parts of the melanoma without haemorrhages.
Figure 2 (A) Patient 5. Transpupillary thermotherapy induced necrosis (N) with a depth of 3.9 mm in a choroidal melanoma sharply demarcated from the viable part (V) of the tumour. Different histological features of cell damage in the superficial and deeper layers of the necrotic zone. All tumour vessels in this area are dilated and occluded by thrombi. Scattered small haemorrhages are present in the transitional zone between the necrotic and the viable part of the tumour (asterisks). Retinal necrosis is seen in the target area. (B) Detail of (A). Blood vessels in the most superficial layer contain red blood cell ghosts (arrow). (C) Detail of (A). The transition area (T) between necrotic (N) and viable (V) parts of the tumour contains scattered haemorrhages (arrows) and tumour cells with dense pyknotic nuclei (asterisks). (D) Histological section of a different part of the tumour as shown in (A). Large dilated blood vessel crossing the area of necrosis became thrombotic but did not bleed. (V) viable part, (N) necrotic part of the tumour, (bv) blood vessel.

Patient 4. Sharp lateral demarcation of transpupillary thermotherapy induced effect in a melanoma (arrowhead), and in retinal (arrows) and subretinal exudate (asterisks).
Figure 4 (A) Patient 11. Transpupillary thermotherapy induced tumour necrosis with a depth of 2 mm. Different histological features of cell damage in the superficial layers of the tumour. Haemorrhages (H) developed along the periphery of the necrotic part of the tumour. Retinal necrosis is present in the target area (arrows). (B) Same patient as in (A). Necrotic tumour borders on the sclera . The inner scleral layers are oedematous (O); the lamellar structure of the collagen remained intact. Intrascleral tumour cells (arrows) have a viable appearance but sclerocytes in this area have disappeared.
Figure 5 Patient 10. Depigmented haematoxylin and eosin stained section of the tumour. Different histological features of transpupillary thermotherapy induced cell damage in the superficial and deeper layers of the tumour. Irregular but sharp demarcation of the area of necrosis as cones of necrotic tissue (arrows) are located in between segments of viable tumour tissue. (V) viable part, (N) necrotic part of the tumour.
There were no signs of inflammation either in the tumour or in the pathway of the radiation beam through the eye. Ocular structures in the pathway of the radiation beam remained normal except for a local anterior subcapsular cataract in three patients (Nos 5, 7, 8); it had developed where the laser beam from the handheld fibre had accidentally touched the iris.
Among the three patients treated with the xenon equipment a thermotherapy effect was not observed in the first two eyes enucleated 24 hours after TTT. The tumour in the third patient showed only some pyknotic tumour cells and dilated blood vessels in the most superficial layers of the tumour.
Histopathological examination of the tumour from patient 9, who was treated with ruthenium-106 brachytherapy 1 year before TTT and enucleated 22 hours after TTT, revealed pyknotic tumour cells throughout the tumour, some dilated blood vessels with thrombi and areas with viable tumour cells. Differentiation between the effect caused by irradiation and that caused by heat was not possible.
Discussion
Transpupillary thermotherapy (TTT) resulted in tumour necrosis to a maximum depth of 3.9 mm with a sharp demarcation between damaged and viable parts of the tumour; it did not affect the normal ocular structures.
The heat induced lesions are comparable with those found in hamster Greene melanomas implanted in the eyes of rabbits and subcutaneously in hamsters.18-23 The heat induced necrosis is caused mainly by a direct cytotoxic effect, not by ischaemia as is evident from our light and electron microscopic findings after thermotherapy.24
Thrombosis of tumour vessels may explain the low tendency to bleed, which was also observed clinically and in animal experiments.18-23
The transition between the necrotic and the viable part of the tumour was about perpendicular to the direction of the radiation beam. The rather sharp demarcation may be attributed to a steep decrease in temperature in the tumour. During TTT the maximum temperature at the apex of the tumour will be about 65°C, at or just below the threshold for an ophthalmoscopically visible coagulation effect.25 26 The temperature in the demarcation zone is estimated to be about 45°C, the lowest temperature which causes irreversible tissue damage.14 27Thus the decrease in temperature in a tumour with necrosis measuring 3 mm in depth will be about 5°C per mm tumour tissue, as was also calculated by Svaasand (personal communication).
Bleaching of erythrocytes in the most superficial tumour vessels is caused by heat damage during stasis of the circulation caused by thrombosis developing during TTT (Fig 2B). The temperature in these vessels was increased above 57°C, the critical clotting temperature where fibrinogen is converted into fibrin.28
Signs of tumour cell damage were absent in one patient (No 1) despite a rather high irradiance of 4–10 W/cm2 and radiant exposure of 7300 J/cm2; in another patient (No 3) an even higher irradiance resulted in only slight cell damage in the superficial tumour layers. The xenon photocoagulator converted for thermotherapy was difficult to handle and manual focusing was not totally stable during the 1 minute exposure time. The rather short time interval between thermotherapy and enucleation, about 24 hours, in two eyes may have influenced the results since visualisation of heat induced lesions may depend on the time interval between thermotherapy and enucleation.
Eight tumours had TTT induced retinal lesions in the target area with a sharp demarcation between the damaged retina in and the normal retina outside the target area (Figs 1A, 2A, 3, 4A). The presence of subretinal exudate did not interfere with a thermotherapy effect in the tumour (Fig 3).
Ocular structures in and outside the radiation area remained unchanged owing to the low rate of absorption of radiation at 810 nm by clear ocular media of about 5%.21 In three eyes the radiation beam from the handheld fibre had touched the iris at the pupillary margin and caused a localised subcapsular cataract; for clinical use the beam is stabilised by fixation of the fibre to a slit-lamp.
Scleral alterations induced by heat11 are not an impediment to clinical thermotherapy; the inner layers of the sclera became oedematous and sclerocytes disappeared but the lamellar structure of the scleral collagen remained intact. The sclera is fairly heat resistant since temperatures of 52.2°C for 45 minutes and 65°C for 1 minute did not cause significant damage.29-31
In one eye intrascleral tumour cells with a viable appearance were located only 36 μm from a totally necrotic tumour (Fig 4B). The distance is too short to explain this viability by a decrease in temperature. Moreover, the heat was sufficient to destroy the sclerocytes in the inner scleral layers. If we assume that the tumour cells were located intravascularly, then their viability could be explained by a cooling effect of the blood circulation, as also observed in animal experiments.24
Since viable intrascleral tumour cells may be the source of tumour recurrences we usually combine TTT with ruthenium-106 brachytherapy. The two treatments, together coined as ‘sandwich therapy’, are complementary since the impact of the transpupillary infrared laser is maximal at the top of the tumour and that of the trans-scleral brachytherapy is maximal at its base (Fig 6).

{kind=link}
{kind=link}
{kind=link}
Schematic drawing of ‘sandwich therapy’, transpupillary thermotherapy being most effective at the top of the tumour, and brachytherapy at the base of the tumour.
Acknowledgments
This investigation was supported by grants of the ‘Haags Oogheelkundig Fonds’ and ‘Stichting Blindenhulp’; Ed Barten assisted in the histological examination.