Article Text

Abstract
AIM The goal was to compare the biological response of the corneal stroma with three porous materials: a melt blown microfibre web of polybutylene:polypropylene (80:20); a polyester spun laced fabric (polyethylene terephthalate), and an expanded polytetrafluoroethylene. Fifty per cent of each of the materials were modified using argon radio frequency.
METHODS Discs (6 mm in diameter) were inserted into interlamellar stromal pockets and followed for a period of 12 weeks. Clinical evaluations were performed weekly. At 6 and 12 weeks, fibroplasia and the distribution of matrix proteins and growth factors (bFGF and TGF-β) were evaluated immunohistochemically. The characterisation of glycosaminoglycans was determined after selective extraction and digestion.
RESULTS The response to the disc resembled that of a wound with a decrease in keratan sulphate and an increase in dermatan sulphate. Pretreatment of the discs reduced corneal oedema and neovascularisation. Heparan sulphate, not normally detected in the corneal stroma, was detected in the region immediately surrounding the disc and in the discs of some materials. The presence of glycosaminoglycans and collagens in the disc indicated that cells had migrated into the disc and deposited a complex matrix in all three materials. The collagen response was not surface specific. bFGF and TGF-β were detected in the region between the disc and the stroma in the polybutylene material and became diffuse with time.
CONCLUSION Fibroplasia occurred most rapidly into the polyester discs but was accompanied by a large number of inflammatory cells. While the distribution of collagens was not altered by the material, the expression and distribution of growth factors was material dependent. bFGF was expressed transiently and occurred before that of TGF-β. It is predicted that the transient expression of growth factors mediates the regulation of matrix proteins.
- synthetic cornea
- basic fibroblast growth factor
- glycosaminoglycans
- wound healing
- cornea
Statistics from Altmetric.com
A normal biological response to synthetic materials is critical to the successful retention of a keratoprosthesis. Many of the complications that occur from the lack of tissue ingrowth at the device–tissue interface result in tissue necrosis and ultimately in the extrusion of the device.1 While the earlier designs had a flange attached to the optical core, there was no attempt to induce fibroplasia.2 By the 1980s, investigators demonstrated that retention depended on the ability of stromal keratocytes to migrate into the device.3 4 More recently, there has been an extensive effort by several groups to develop porous materials that possess the following criteria: the device must permit the migration of stromal keratocytes and the subsequent deposition of collagens and proteoglycans; the interface of the cells and material must have sufficient tensile strength; the diffusion of nutrients must occur, and the peripheral component must not become encapsulated. One major difference in the development of a synthetic cornea from that of devices intended for skin or other vascular tissues is the inability to use biodegradable polymers.5
Many different materials are currently being evaluated and incorporated into keratoprosthetic devices. Early studies demonstrated that both fibre diameter and pore size were critical in optimising tissue ingrowth and diffusivity. This resulted in fibre diameters that ranged from 2 to 12 μm with a void volume of 88%.4-6Currently the materials incorporated into devices and evaluated in vivo range from the polybutylene:polypropylene (80:20) web,7 a porous PTFE (impra),8 and polyhema9 where both components are cross linked polymers of polyhema. Additional materials used in devices include bone,10 Dacron, and siliconised hema.
Our goal was to compare the biological response with several materials that are employed in other devices over a period of 12 weeks in vivo. The three materials that we chose to evaluate were a polyester similar to Dacron used in vascular grafts; a polybutylene:polypropylene web, and an expanded polytetrafluoroethylene (impra). Recently, we demonstrated that the application of radio frequency argon plasma yielded the anterior optical surface optimal for epithelialisation in vitro and in organ culture.11 Therefore the porous materials were treated with argon plasma. Our analysis consisted of clinical and histological assessment of oedema, inflammation, and ingrowth. In addition, we compared the ability of stromal fibroblasts that had entered the three materials to deposit glycosaminoglycans. We examined the localisation and expression of transforming growth factor beta (TGF-β) and basic fibroblast growth factor (bFGF). Our results indicate that there are distinct biological responses for each material. Most interesting may be the specific localisation of TGF-β and bFGF, to the tissue–device interface when specific materials are inserted. These are detected at 6 weeks concurrent with the appearance of heparan sulphate.
Materials and methods
Three porous materials intended for use as the peripheral skirt part of a synthetic cornea were evaluated. These were: (1) a melt blown microfibre web of polybutylene:polypropylene (80:20), whose fibre diameter ranged from 2 to 12 μm and had a void volume of 88% (The 3M Company) (polybutylene); (2) a Sontara (DuPont) polyester spun laced fabric (polyethylelene terephthalate) (polyester). The polyester fabric was coarser than the polybutylene, with a fibre diameter of 10 μm and a void volume of 92%; and (3) an expanded polytetrafluoroethylene from International Polymer Engineering (Tempe, AZ) (ePTFE). ePTFE is a polymer with a high melting temperature, a fibre diameter of 3–4 μm, and a void volume of 91%. All materials were cut into discs, 6 mm in diameter, and subjected to an extensive washing protocol. The thickness of the discs varied with each material (see Table 2 column 1). After the discs were cleaned, half of the specimens were treated with argon rf plasma (AST Billerica, MA, USA). Nine discs were used at each time point for each type of material or treatment.
Changes of corneal and disc thickness after implantation (mm)
PLACEMENT OF THE DISCS WITH SURGICAL PROCEDURE
All research using animals conformed to the Declaration of Helsinki and the Guiding Principles in the Care and Use of Animals (NIH publication no 85–23 Rev 1985). The New Zealand rabbits were anaesthetised with Ketaset (ketamine) at a dose of 35 mg/kg and Rompun (xylazine) at a dose of 5 mg/kg administered together intramuscularly. A 4 mm incision was made along the corneal limbus and 3 mm inside it. The incision was made half to two thirds the depth of the cornea and the lamellae were separated with a cyclodialysis spatula creating a 7 mm diameter pocket in the centre of the cornea. The 6 mm disc was inserted into the interlamellar stromal pocket. The opening was closed using an 10–0 nylon suture.
CLINICAL EVALUATION
Clinical evaluations were performed a minimum of two times a week using slit lamp biomicroscopy and photography. Corneal oedema (graded on a scale from 0 to 3) and corneal infiltration (graded on a scale from 0 to 2) were noted twice weekly.
Neovascularisation was graded on the following scale:
- 0,
having no neovascularisation;
- 1,
initial neovascularisation detected from the limbus;
- 2,
neovascularisation localised between the limbus and margin of the disc;
- 3,
neovascularisation approaching the disc margin; and
- 4,
neovascularisation present in the central disc or covering the entire disc.
The depth (shallow or normal) and inflammation in the anterior chamber were also observed.
HISTOLOGY
Rabbits were sacrificed at 6 and 12 weeks. At each time point the corneas were excised and fixed in 3.7% formaldehyde. Frozen sections were cut from one half of the cornea for immunohistochemical experiments. The other half was processed for JB-4 methacrylate (Polysciences Inc, Warrington, PA, USA), Two μm sections were cut and stained with haematoxylin and eosin. All tissue samples were evaluated and photographed using a Nikon UFX-IIA microscope.
IMMUNOHISTOCHEMISTRY
To determine the distribution of antigens, 50% of the corneas were frozen, embedded in OCT, and 5 μm sections cut. The localisation of collagen types I, III, and VI (mouse monoclonal antibodies (MAb), from Chemicon), keratan sulphate (KS), dermatan sulphate (DS), (gift from Dr Charles Cintron Schepens Eye Institute), bFGF, and TGF-β (mouse MAb from Genzyme Cambridge, MA, USA) were examined. Briefly, sections were rehydrated in phosphate buffered saline (PBS) (pH 7.2), blocked with 3% bovine serum albumin (BSA) in PBS and incubated in 1% BSA/PBS with the appropriate primary MAb for 2 hours at room temperature. Monoclonal antibodies against collagen types I, III, VI, bFGF, and TGF-β were used at a concentration of 1 μg/50 μl. The antibody to KS was used at 1 μg/20 μl. Additional sections were preincubated with chondroitinase ABC (1 U/ml) for 2 hours at 37°C, washed, and then incubated in primary antibody against DS (1:10). Sections were washed with PBS, and incubated in 1% BSA/PBS containing the appropriated secondary antibody, conjugated to FITC (1:50), for 1 hour at room temperature. Sections were washed extensively, mounted with anti-fade media, and photographed using a Nikon UFX-IIA microscope. Lack of primary antibody was used as a control.
EXTRACTION AND PURIFICATION OF PROTEOGLYCANS
Corneas containing discs were examined after 6 and 12 weeks. A 6 mm trephine was used to remove the control cornea and disc. The corneal tissue anterior and posterior to the disc were teased free and treated as surrounding tissue. The disc and surrounding tissue were analysed separately. Samples were pooled, extracted, and proteoglycans purified following the procedure of Brown et al 12 13 and Midura et al.14
ENZYMATIC DIGESTION AND DIMETHYLMETHYLENE BLUE COLORIMETRIC ASSAY
Purified GAGs were identified and quantified using selective polysaccharide lyases. Each data point represents pooled samples for each time point and region (see above). Total sulphated GAGs were quantitated colorimetrically using the dimethyl methylene blue (DMB) assay.15 Absorbance was read at 525 nm. Concentrations were determined from standard curves of purified GAGs.
Results
CLINICAL EVALUATION
Corneal oedema was observed postoperatively for a period of 12 weeks. Oedema was greatest at 2 weeks and became negligible after 12 weeks (Fig 1A, B). When surface treated implants were examined, oedema decreased after 4 weeks and was not detected after 8 weeks. These observations indicated that corneal oedema was lessened when the materials were surface treated with argon rf plasma (Fig 1A). The difference in response between treated and untreated was most marked with the polyester discs, while the treated polybutylene discs elicited the least corneal oedema (Fig 1B). The data represent nine corneas per condition.
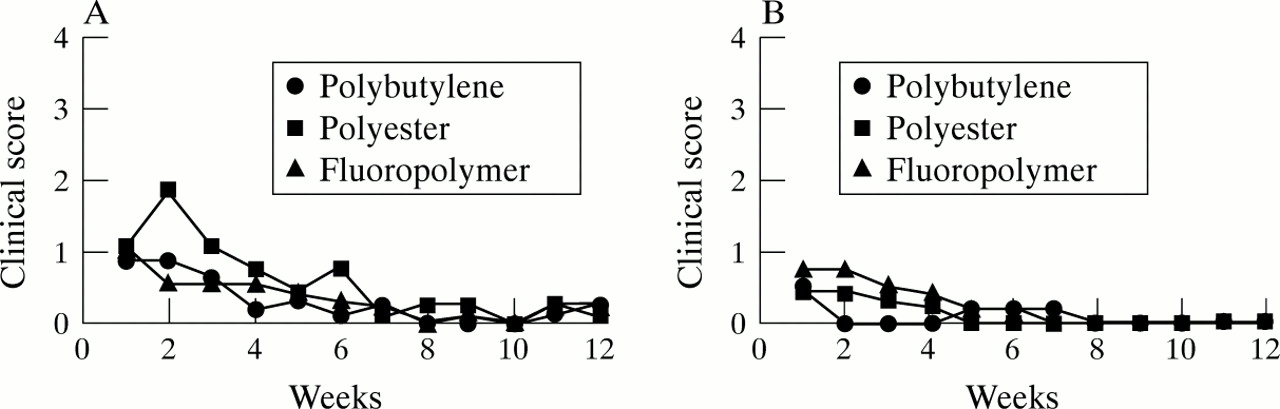
Oedema. (A) Non-treated. Corneal oedema gradually decreased over 6 weeks after surgery. Oedema was minimal after 12 weeks. Individual analysis at 6 weeks —polybutylene: 3/9 animals had a score of 1; polyester: 2/9 animals had a score of 2; and ePTFE: 3/9 animals had a score of 1. (B) Treated. Corneal oedema was minimal 8 weeks after treated discs were inserted. These discs were surface modified with an argon rf plasma. The oedema in response to the polyester disc decreased markedly after surface treatment. Individual analysis at 6 weeks—polybutylene: 1/9 animals had a score of 2 at 6 weeks; polyester: no animals had oedema; and ePTFE: 1/9 animals had a score of 2. Each data point represents the average of nine corneas.
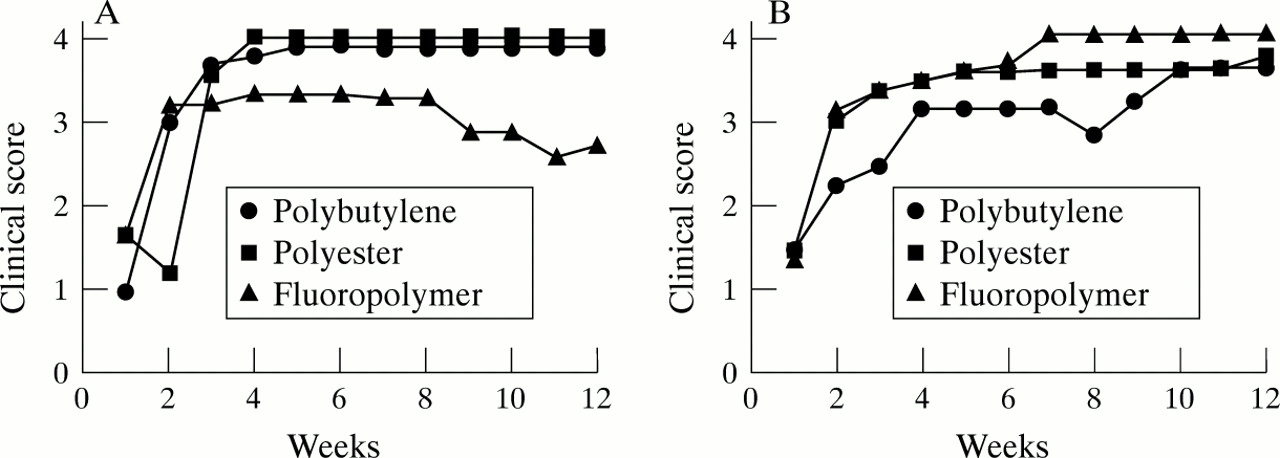
The onset and extent of corneal vascularisation was examined over a period of 12 weeks. Neovascularisation was detected at the superior limbus 1 week after implantation of all materials. By 4 weeks, vessels were present over the entire cornea and disc for both the untreated polybutylene and polyester materials (Fig 2A). In response to the untreated ePTFE, neovascularisation was less severe and some blood vessels had occluded by 8 weeks (Fig 2A). When discs were treated with argon rf plasma, the onset of corneal neovascularisation was delayed and less extensive in the polyester and polybutylene discs (Fig 2B). For the latter materials, neovascularisation was only present in the disc margin and an area between the edge of the disc and central cornea and never covered the entire cornea (see Materials and methods). When treated ePTFE discs were evaluated after 7 weeks, neovascularisation was extensive (score of 4/4) indicating that the treatment may have altered the material (Fig 2B). Inflammation in the anterior chamber was not detected.
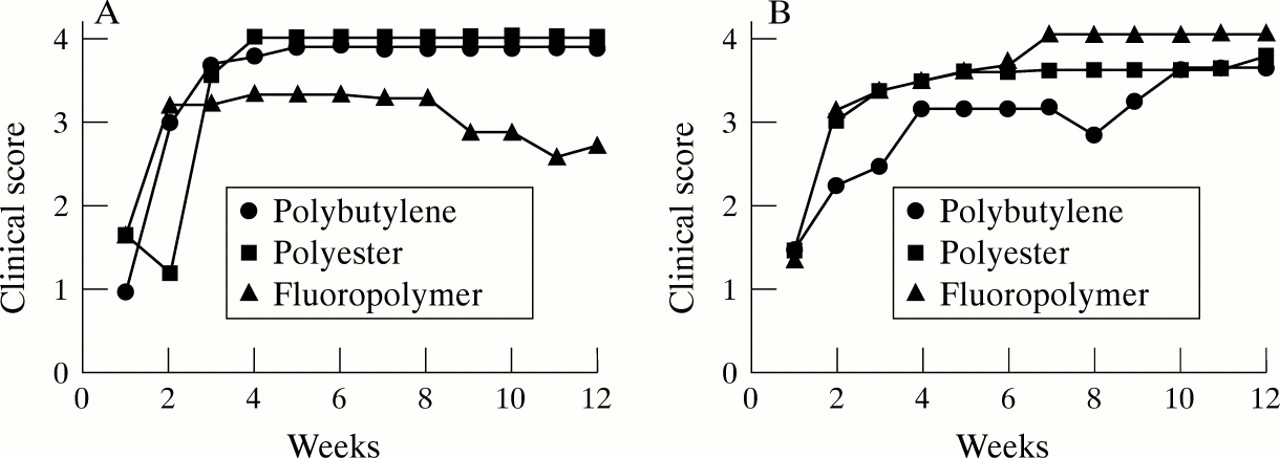
Neovascularisation. (A) Non-treated. When discs were implanted, neovascularisation was detected within 1 week after surgery. After 3 weeks, blood vessels approached the disc margin. Neovascularisation was most extensive when polyester and polybutylene discs were inserted. In response to ePTFE, vessels were never detected in the discs and after 8 weeks some vessels had occluded. Individual analysis at 12 weeks —polybutylene: 5/9 animals had a score of 4; polyester: 9/9 animals had a score of 4; and ePTFE: 4/9 animals had a score of 4. (B) Treated. When ePTFE discs were surface treated neovascularisation increased while the response to the other two materials decreased. Neovascularisation was more gradual in response to the modified polybutylene, not reaching the margin of the disc until 4 weeks. Individual analysis at 12 weeks—polybutylene: 4/9 animals had a score of 4; polyester: 5/9 animals had a score of 4; and ePTFE: 9/9 animals had a score of 4. Each data point represents the average of nine corneas.
HISTOLOGICAL ANALYSIS
To determine whether keratocytes migrated into the porous discs, cross sections were analysed. In the polybutylene discs keratocytes were present within the disc after 6 weeks but there remained open regions in the interstices of the disc. Inflammatory cells decreased over 6 to 12 weeks (Table 1). By 12 weeks keratocytes were present throughout the porous discs and little open space remained (Fig 3A). Treatment with the argon rf plasma did not alter fibroplasia or disc thickness (data not shown). The thickness of the disc at 12 weeks increased by 14% (Table 2).
Presence of inflammatory cells in the disc and surrounding stroma

Histological appearance of discs inserted into stromal interlamellar pockets 12 weeks after surgery. Cross sections were stained with haematoxylin and eosin. (A) Polybutylene disc inserted (100×). (a) Higher magnification of (A) indicated by an asterisk (200×). (B) Polyester disc inserted (100×). (b) Higher magnification of (B) indicated by an asterisk (200×). A large number of inflammatory cells are present within the polyester disc. (C) ePTFE disc inserted (100×). (c) Higher magnification of (C) indicated by an asterisk (200×). In all cases the cells migrated from the anterior and posterior stroma into the disc. The data represent those from nine animals.
When discs of polyester were implanted into interlamellar stromal pockets, keratocytes were detected within the interstices of the disc after 6 weeks. However, a large number of inflammatory cells were detected inside the disc and surrounding stroma (Table 1) (Fig 3B). When the polyester discs were treated with argon rf plasma, fibroplasia was unaltered and the number of inflammatory cells inside the disc and the surrounding corneal stroma decreased (Table 1). After 6 weeks the discs did not change significantly in thickness from the control unimplanted discs. However, after 12 weeks, the disc thickness increased by 58% (Table 2).
When ePTFE discs were examined after 6 weeks, keratocytes were present but open spaces remained. After 12 weeks, little increase in disc thickness was detected and keratocytes had filled most of the remaining open spaces (Table 2) (Fig 3C). A small number of inflammatory cells were detected in the disc and stroma (Table 1). The endothelium remained intact after insertion of discs.
LOCALISATION AND DEPOSITION OF GLYCOSAMINOGLYCANS
The glycosaminoglycans (GAGs), keratan sulphate (KS), and dermatan sulphate (DS) were localised after specific enzyme digestion.13 In addition, the concentration of KS, DS, and HS deposited in each disc was quantitated. Here, the data represent a pooling of the tissue. Keratan sulphate and DS were localised in the corneal stroma and interstices of discs in all three materials at 6 and 12 weeks, in both treated and untreated discs. Intense staining was detected within the discs (Fig 4). Staining was not detected in undigested sections. Fluorescence was negligible when the primary antibody was omitted. The data represent micrographs from a total of nine animals.

Distribution and composition of glycosaminoglycans. Keratan and dermatan sulphate were localised on cross sections of corneas 42 days after treated discs were inserted. (A), (D) Polybutylene disc inserted; (B), (E) polyester disc inserted; and (C), (F) ePTFE disc inserted. (A), (B), (C) Corneas stained with anti-dermatan sulphate shows dermatan sulphate within the disc. (D), (E), (F) Corneas stained with anti-keratan sulphate shows keratan sulphate within the disc (100×). Composition of glycosaminoglycans present 12 weeks after implantation of the porous materials. Aliquots from purified extracts were assayed for dermatan sulphate (DS), keratan sulphate (KS), and heparan sulphate (HS). Dermatan sulphate was defined as GAG susceptible to chondroitinase ABC. Keratan sulphate was defined as GAG susceptible to heparanase III. Data are presented as specific GAG/total GAG.
The GAGs present in the disc and surrounding stroma were calculated following selective digestion and compared with the control contralateral stroma. Dermatan sulphate was defined as GAG susceptible to chondroitinase ABC and AC digestion, heparan sulphate (HS) as GAG susceptible to digestion with heparanase III, and KS as GAG susceptible to digestion with keratanase. Seventy per cent of the GAG in the contralateral stroma was keratan sulphate. Heparan sulphate was not detected. A decrease in KS accompanied by an increase in DS was seen in the surrounding tissue of all experimental stromas. Heparan sulphate was detected in the surrounding stroma (Fig 5A). The appearance of HS was coincident with a decrease in the ratio of DS:KS. The presence of GAG in the disc indicates that cells in the disc have laid down a matrix. Both DS and KS were detected in the discs. The polybutylene material had the smallest percentage of KS indicating a slower rate of wound repair than other materials (Fig 5B).

(A) Glycosaminoglycans present in tissue adjacent to the disc. (B) Glycosaminoglycans present in the disc. Heparan sulphate is detected after insertion of the disc in both the surrounding tissue and in the disc. Keratan sulphate is reduced in response to injury. Each data point represents data from nine pooled samples.
LOCALISATION OF TGF-β AND bFGF
As heparan sulphate was detected in the surrounding stroma and discs, the expression and distribution of the growth factors, bFGF and TGF-β, were examined. bFGF was detected intensely along the edge of the stroma and disc at 6 weeks in the untreated polybutylene and ePTFE discs (arrows, Fig 6B, C). By 12 weeks it was detected diffusely throughout the polybutylene disc (Fig 7B). bFGF was detected along the disc margin in ePTFE discs at 12 weeks (arrow, Fig 7C). In polyester discs, bFGF was detected diffusely in the discs at 6 and 12 weeks (Fig6A, 7A). bFGF was not detected in the unwounded stroma.

Distribution of bFGF and TGF-β 6 weeks after untreated discs were implanted in the cornea. (A), (D) Polyester discs inserted; (B), (E) polybutylene discs inserted; (C), (F) ePTFE discs inserted. (A), (B), (C) Corneas stained with a MAb to bFGF. bFGF is localised along the interface between the disc and stroma in (B) and (C) (arrow). (D), (E), (F). Corneas stained with a MAb to TGF-β. TGF-β is present along the margin of the disc and stroma in (E) (arrow) and is diffuse in (D) and (F) (100×).

Distribution of bFGF and TGF-β 12 weeks after untreated discs were inserted into the stroma. (A), (D) Polyester disc inserted; (B), (E) polybutylene disc inserted; and (C), (F) ePTFE disc inserted. (A), (B), (C) Localisation of bFGF. bFGF was present along the interface between the disc and stroma of (C) and was diffuse in (A) and (B). (D), (E), (F) Localisation of TGF-β. TGF-β was diffuse throughout the disc (100×).
TGF-β was detected intensely along the interface of the stroma and disc at 6 weeks in the untreated polybutylene discs (arrow, Fig 6E). By 12 weeks it was detected diffusely throughout the polybutylene disc (Fig 7E). TGF-β was detected throughout the polyester and ePTFE discs at both 6 and 12 weeks (Figs 6D, 7D, 6F, 7F). The background staining was greater for the ePTFE than for other materials. TGF-β was not detected in the control unwounded cornea (data not shown). The results indicated that the maximal expression of bFGF occurs more rapidly than TGF-β after a wound.
LOCALISATION OF COLLAGEN TYPES I, III, AND VI
Previously we found that type I collagen was synthesised and deposited in the disc over time.4 16 Type I collagen was detected within the discs after 6 weeks and the localisation did not change after 12 weeks (Fig 8A, D). The polybutylene disc was shown as there was no difference in the localisation of the collagens in response to the three materials. Surface treatment did not alter the localisation and deposition of type I collagen.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Localisation of collagen types I, III, and VI in the cornea after polybutylene discs were inserted. Immunohistochemistry of corneal cross sections after 6 weeks (A, B, C) and 12 weeks (D, E, F). (A), (D) Localisation of type I collagen; (B), (E) type III collagen; and (C), (F) type VI collagen (100×).
Type III collagen was found in both the disc and along the disc and surrounding stroma with intense staining localised to the disc. After 12 weeks type III collagen was localised to the disc. No difference in the localisation of type III collagen was detected in either treated or untreated materials (data not shown). Type III collagen was most intense in the interstices of polyester and polybutylene discs (Fig 8B, E). The results indicate that while the neighbouring stroma has been repaired successfully after 12 weeks, the collagen deposited within the disc remained characteristic of an injured cornea.
Type VI collagen, localised between collagen fibrils of corneal stroma, was detected in the discs and corneal stroma. Intense fluorescence was detected throughout the discs (Fig 8C, F). Staining intensity was similar in both treated and untreated materials after 12 weeks (data not shown). While the response to the treated discs is not shown in the figures, there were no detectable changes in the localisation or intensity of staining.
Discussion
The interface of the peripheral haptic and surrounding stroma is critical in stabilising the device and maintaining a watertight junction between the keratoprosthesis and adjacent corneal stroma. The material must be flexible and possess elasticity to avoid stress at points of attachment that might contribute to stromal necrosis and melting. Additionally, the peripheral material must act as a barrier against epithelial downgrowth and be sufficiently porous to allow for keratocyte ingrowth. All of the materials that were chosen for investigation are similar to those used in other implant prototypes. This is the first attempt to compare the biological response under identical conditions to three porous materials placed into lamellar stromal pockets. Furthermore, we have made novel observations on the expression of growth factors in response to the deposition of matrix molecules after insertion of a disc.
The argon plasma treatment was used to alter the surface chemistry of the hydrogel making it suitable for epithelial migration onto its surface.11 This treatment caused etching and subsequent deposition of etched fragments on the treated surfaces. In general, the surface treatment decreased corneal oedema, the extent of neovascularisation, and the recruitment of inflammatory cells (exception ePTFE). These results indicate that argon rf plasma treatment not only may promote epithelialisation but may enhance the biocompatibility of certain prosthetic devices.
The three materials chosen for comparison had fibres of different sized diameters but similar void volumes allowing us to ask whether these characteristics played a role in cellular ingrowth and matrix deposition. The development of the polybutylene was based on a large number of trials varying fibre diameter, pore size, and resulting diffusivity.6 Recently, other investigators have also examined the role of fibre diameter and pore size in order to optimise the fibroplasia in their device.8 Fibroplasia was most extensive in the polyester discs that had the largest fibre diameter and greatest void volume. The thickness of the polyester and polybutylene discs increased by 58% and 14% respectively after 12 weeks in the stroma. These results indicate that the smaller fibre diameter of the ePTFE may in part be responsible for the decreased fibroplasia and lack of accommodation as matrix is deposited. Corneal wounds are associated with changes in matrix proteins such as collagens and proteoglycans. Trinkaus-Randall et al showed that the deposition of collagen within the disc increased significantly by day 28 and was prominent by day 42.4 More recently, Trinkaus-Randall et al demonstrated that fibroplasia was enhanced by preseeding the discs with cultured fibroblasts and further showed that enhanced fibroplasia promoted the deposition of an extracellular matrix.16 Malley et alperformed anterior keratectomies using excimer laser surgery on primate corneas and demonstrated that after 1 month, type III collagen continued to be detected at the injured region while type VI collagen was present in both normal and repairing corneal stroma.17Melles et al studied the response to partial thickness wounds of the cornea and found fibronectin, type III, VI, and VII collagen, in a lamellar interweaving pattern across the unsutured wound.18 More recently investigators examined porous discs after implantation to determine whether the collagen composition resembled that of a normal cornea. Collagen types I, IV, and VI were detected in the discs and they demonstrated that the deposition of collagen was directly related to an increase in the porosity of the fabric.8 Chirila et al examined fibroplasia into the polyhema sponge and demonstrated that type III collagen was present in the surrounding stroma, consistent with a normal healing response of stromal fibroblasts.9 These studies indicated that collagen can be used as an indicator for corneal repair and compatibility of a material with the tissue. In response to an injury, chondroitin dermatan sulphate PGs are synthesised having GAG chains of higher sulphation. At the same time, the keratan sulphate molecules that are synthesised are increased in size but decreased in sulphation.19 20 The appearance of HS at 6 weeks demonstrated that HSPG increased after injury,21 and that bFGF and TGF-β were detected in corneal cells.22 Brownet al have shown that the active form of TGF-β is present at the wound margins in the stroma while the latent form was detected a distance from the wound.13 In preliminary experiments we have shown that the expression of TGF-β1mRNA increases at the leading edge of the wound. In other cell models HS has been shown to modulate growth factor receptor binding and activity. It has been well established that TGF-β regulates the expression of core proteins by stimulating GAG synthesis and increasing the length of GAG chains.23 bFGF has been shown to mediate the expression of other core proteins (syndecan and perlecan).24 25 Our results, demonstrating the deposition of HS in the surrounding stroma and disc and the expression of bFGF and TGF-β1 at the interface of the material and stroma suggest that their expression is regulated by a feedback mechanism. These results indicate that the rate of stromal ingrowth into the disc and the change in the availability of growth factors may be the controlling factor in the deposition of matrix proteins and the anchoring of the material within the stroma.
Acknowledgments
Supported by NEI EY11004 and departmental grants from Research to Prevent Blindness Inc and the Massachusetts Lions Eye Research Fund, Inc. We thank the New England Corneal Transplant Fund for supporting Dr Xin Yi Wu. We thank Christopher Brown for his help in extracting and analysing the glycosaminoglycan data.