Article Text

Statistics from Altmetric.com
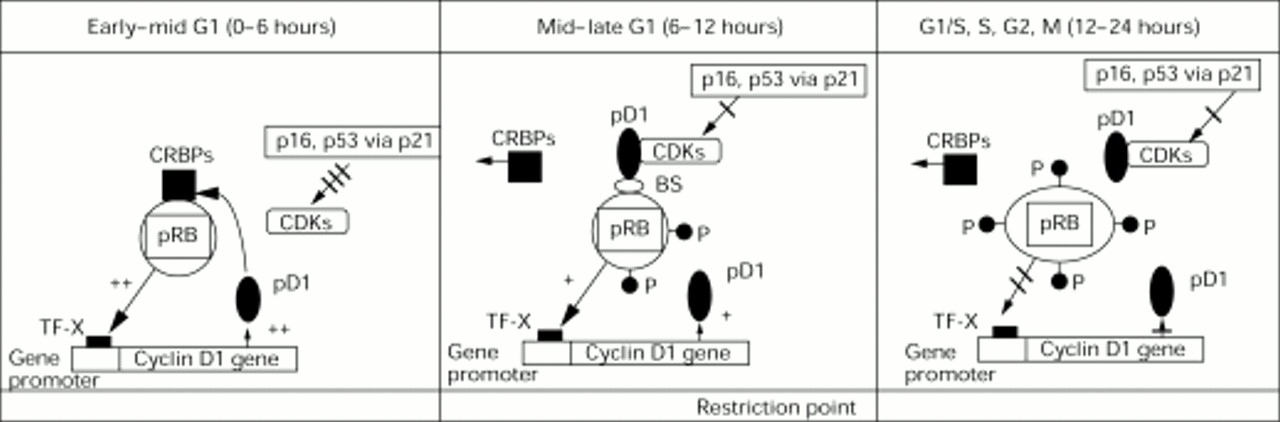
Cyclins are cell cycle regulatory molecules which complex with and activate cyclin dependent kinases (CDKs) to govern cell cycle progression (Fig 1) (Table 1).1 They include cyclin D1 protein which binds with CDK4, leading to phosphorylation of the retinoblastoma protein (pRB), a product of the tumour suppressor gene located on chromosome 13q14 which can inhibit cell proliferation (Fig 1). Phosphorylation of pRB results in a change in pRB molecule configuration, the release of transcription factors bound to pRB, such as E2F, and ultimate cell cycle progression from G1 to the S phase (Fig 1).23 Interest in a possible role of cyclin D1 in tumorigenesis has grown since experiments demonstrated that induction of cyclin D1 in cells arrested in the early G1 phase by transfection with pRB was sufficient for cell cycle completion.4 Further, cyclin D1 overexpression has been reported in several tumours including parathyroid adenomas,5 mantle cell lymphoma,67malignant melanoma of the skin,8 as well as carcinomas of the breast, lung, liver, oesophagus, urinary bladder, head and neck, vulva, and uterine cervix.8-14

Interactions between cyclin D1 gene and protein (pD1) and retinoblastoma protein (pRB) as well as between the cyclin dependent kinases (CDKs) and their inhibitors (p16 and p21 via p53) during the cell cycle (modified from Lukas et al55). During early to mid G1, the concentrations of pD1 are low. pRB is hypophosphorylated and has a stimulatory activity on the transcription of the cyclin D1 gene. At this time, the retinoblastoma “pockets” are occupied by “cellular retinoblastoma binding proteins” (CRBPs), which are potent cell cycle stimulators when released later from the pRB pockets. The CDKs are inhibited by the CDKIs, including p16 and p21, the latter being stimulated by p53. The combination of hypophosphorylated pRB, the pRB bound CRBPs, and the inhibitory effects of the CDKIs contribute to cell cycle arrest at the restriction point (R point) in the mid to late G1 phase. The concentrations of pD1 increase and eventually are sufficient to combine with the CDKs, overriding the inhibitory activity of the CDKIs and resulting in (a) the displacement of the CRBPs from the RB pockets, (b) phosphorylation of the pRB, causing a change in the configuration of the pRB molecule. These alterations stimulate cell progression into the S phase, as well as a decrease in the transcriptional stimulus of the cyclin D1 gene. The concentration of pD1, consequentially, decreases during the S, G2, and M phases. TF-X represents a proposed transcription factor55 and BS, a possible binding site or molecule through which cyclin D1 indirectly interacts with pRB.
Molecules involved in executing cell cycle arrest at the restriction point (R point) between G1-S phase (A) and those involved in recommencement of cell cycling after the R point (B)
In addition to cyclin D1, other cell cycle regulatory molecules may participate in the development and progression of human tumours. In particular, a group of cyclin dependent kinase inhibitors (CDKIs) have been proposed in tumorigenesis as possible tumour suppressor genes15-17 (Fig 1) (Table 1). These proteins act as negative regulatory elements of cell proliferation by inhibiting the kinase activity of the cyclin/CDK complexes and are, thereby, implicated in the mechanisms of cell arrest that allow the cell time for DNA repair. Of these molecules, p16 and p21 are strong candidates to participate in tumour progression. p16 gene (CDKN2/MTS1/INK4a) is located on chromosome 9p21 and has been found to be deleted, mutated, or downregulated by hypermethylation at high frequency in different types of tumours, including cutaneous and uveal melanomas.1517-20 Experimental evidence has confirmed p16 as an anti-oncogene and the incidence of its mutations appears to be inversely correlated with frequencies of other oncogenic mutations, such as the loss of pRB, along the cyclin D1/CDK/p16/pRB pathway.21
p21 gene (WAF1/Cip1/SDI1), located on chromosome 6, results in G1 arrest via the inhibition of the CDKs and via an interaction with the proliferating cell nuclear antigen protein.22 Although it can be activated via p53 independent mechanisms,23 p21 is induced by “wild type” but not mutant tumour suppressor gene p53. It is, therefore, considered to be a critical downstream effector of p53 in cell cycle arrest.222425 In normal tissues, p21 has been associated with maintaining growth arrest in terminally differentiated tissues.26 Somatic mutations in p21 gene are rare in human tumours27; however, some have been demonstrated in human prostate cancer.28
Apart from inducing cell arrest, the tumour suppressor gene p53, located on chromosome 17q, has a second distinctive function depending on the cell type. This second function is the induction of apoptosis, also known as programmed cell death (PCD).29 Wild type p53 has been associated with a downregulation in the anti-apoptotic genebcl-2 and an upregulation in thebcl-2 associated genebax, this combination resulting in apoptosis induction. Disruption of this balance can occur owing to a loss of normal p53 gene function or to a dysregulation of BCL-2 protein expression—for example, following the characteristic t(14;18) translocation observed in follicular lymphoma.30 Thereby, the balance is tipped towards the prevention of PCD, a characteristic of bcl-2 which distinguishes it from other oncogenes, which promote cell proliferation as their mechanism of tumorigenesis. An inverse relation between BCL-2 protein expression and mutant p53 expression has been shown in malignant lymphoma,31 breast3233 and thyroid carcinoma.34
Retinoblastoma is the most common intraocular tumour in childhood occurring in one of 17 000 to 24 000 live births,35-38and it may occur either as a hereditary or a sporadic tumour. The chromosome locus of the retinoblastoma gene is in the region 13q14 and according to the “two hit hypothesis” proposed by Knudson,39 two mutational events leading to the inactivation or deletion of both alleles of the retinoblastoma locus must occur before the development of retinoblastoma. Uveal melanoma, on the other hand, is the most frequent primary intraocular tumour in white adults with an incidence of 0.7 per 100 000.40 The pathogenesis of uveal melanoma is unclear and probably represents a multistep process involving the progressive and clonal accumulation of multiple genetic lesions affecting proto-oncogenes and tumour suppressor genes. Recent studies have demonstrated certain genetic changes associated with these tumours, in particular, monosomy 3, multiplication of chromosome 8q, as well as loss of 9p.41-47
Although the role of RB gene has been clarified in retinoblastoma,39 little is known about the cell cycle markers of G1-S phase transition and their relation to each other in this tumour. Further, only occasional reports have addressed these issues in uveal melanoma.19 In the present study, we investigated the expression of cyclin D1 in one type of intraocular tumour where mutations of the pRB are present (retinoblastoma) and compared it with another with an apparently functional pRB (uveal melanoma). In particular, we investigated the relation between cyclin D1 protein expression and that of pRB, p53, p21, and p16 in these two tumours. We also analysed whether there was a possible correlation between expression of these cell cycle markers of G1-S phase transition and the growth fraction of the tumour, as determined by the Ki-67 antigen, or with BCL-2 expression.
Methods
CONVENTIONAL HISTOLOGY AND IMMUNOHISTOLOGY
Ninety eyes were enucleated for either uveal melanoma (n=66) or retinoblastoma (n=24). Eight eyes donated for corneal transplantation with an average postmortem time of 12 hours served as controls. All enucleated eyes were fixed in 10% buffered formalin and embedded in paraffin wax. Conventional histological stains of the uveal melanomas were assessed for cell type using the modified Callender system48—that is, spindle A, spindle B, epithelioid, and mixed cell type. Retinoblastomas were graded as to the degree of differentiation according to a system proposed by Nork and coworkers.49 Briefly, the grades of differentiated were: (1) poorly differentiated—cells with high nuclear to cytoplasmic ratios with a high mitotic index. Pseudorosettes and Homer–Wright rosettes were found in such areas; (2)moderately differentiated—cells with moderate nuclear to cytoplasmic ratios, a moderate mitotic index, and possible pseudorosettes and Flexner–Winterstein rosettes; (3)well differentiated—cells with a low nuclear to cytoplasmic ratio, a low mitotic index, and the formation of florets. The recently described “zones 1, 2, and 3” around pseudorosettes49 were used for the evaluation of tumour cell staining. Briefly, these were as follows “zone 1” (central region near blood vessel), “zone 2” (adjacent to edge of the pseudorosette), and “zone 3” (edge of pseudorosette).49
Additional slides were stained for immunohistochemical studies using several monoclonal and polyclonal antibodies that are reactive in paraffin embedded tissues. An antigen retrieval method using a pressure cooker was performed before immunohistochemical staining.50 The staining consisted of a first stage incubation with the following primary monoclonal antibodies: cyclin D1 (clone P2D11F11; Novocastra; Germany); retinoblastoma protein (pRB) (clone G3-245 which binds to an epitope between amino acids 300–380 of human RB; Pharmingen; Germany); p53 (clone DO7 which recognises both wild type and mutant p53 proteins; Dako; Denmark); p21 (clone DCS-60.2; Neomarkers; Germany); p16 (clone DCS-50.1/A7; Neomarkers; Germany); BCL-2 (clone 124; Dako; Denmark); MIB-1 (antigen Ki-67 which reacts with a DNA associated antigen in the nuclei at all phases of the cell cycle except the resting phase51; the antibody was kindly provided by Dr J Gerdes, Borstel, Germany); and glial fibrillary acid protein (clone 6F2; GFAP; Dako; Denmark). The antibodies were made visible with an indirect immunoperoxidase method for p53, whereas the alkaline phosphatase anti-alkaline phosphatase (APAAP) method was used to demonstrate the binding of the remaining antibodies.52In heavily pigmented tumours, the sections were placed in hydrogen peroxide for 18 hours to remove melanin pigmentation from the tumour cells before cover slipping the slides, as previously described.53
Cells were considered positive for cyclin D1, pRB, p53, p16, p21, and for MIB-1 only when distinct nuclear staining was identified. The percentage of immunoreactive nuclei in the uveal melanoma and retinoblastoma was evaluated by counting at least 5 × 100 cells using the 40× objective (Olympus, BH2). Positive controls included cases of mantle cell lymphoma for cyclin D1, colon carcinoma for p21, and gastric and breast carcinoma for p16. Negative controls were obtained by omitting the primary monoclonal antibodies.
STATISTICAL ANALYSIS
Comparison of differences was performed using the Student’st test. p Values at less than 0.05 were interpreted to be statistically significant.
Results
CLINICAL FEATURES
The patients (n= 23) with retinoblastoma consisted of eight females and 15 males with an age range of 4 months to 19 years; mean 3 years. Twelve patients had bilateral tumours and 11 unilateral. Sixteen patients were treated with primary enucleation; five with chemoreduction before planned enucleation; two with combined chemotherapy and radiotherapy before enucleation; and one patient with radiotherapy alone.
The patients (n=66) with uveal melanoma consisted of 39 females and 27 males with an age range of 9–88 years; mean 59 years. Fifty five patients had been treated with primary enucleation or local excision of the tumour; nine with radiotherapy before enucleation.
CONVENTIONAL AND IMMUNOHISTOLOGY
The results of the immunohistochemical investigations are summarised in Table 2.
Summary of the immunohistochemical findings for cyclin D1 and related G1-S phase proteins in the normal retina, untreated retinoblastoma, and untreated choroidal melanoma
Normal choroid and retina
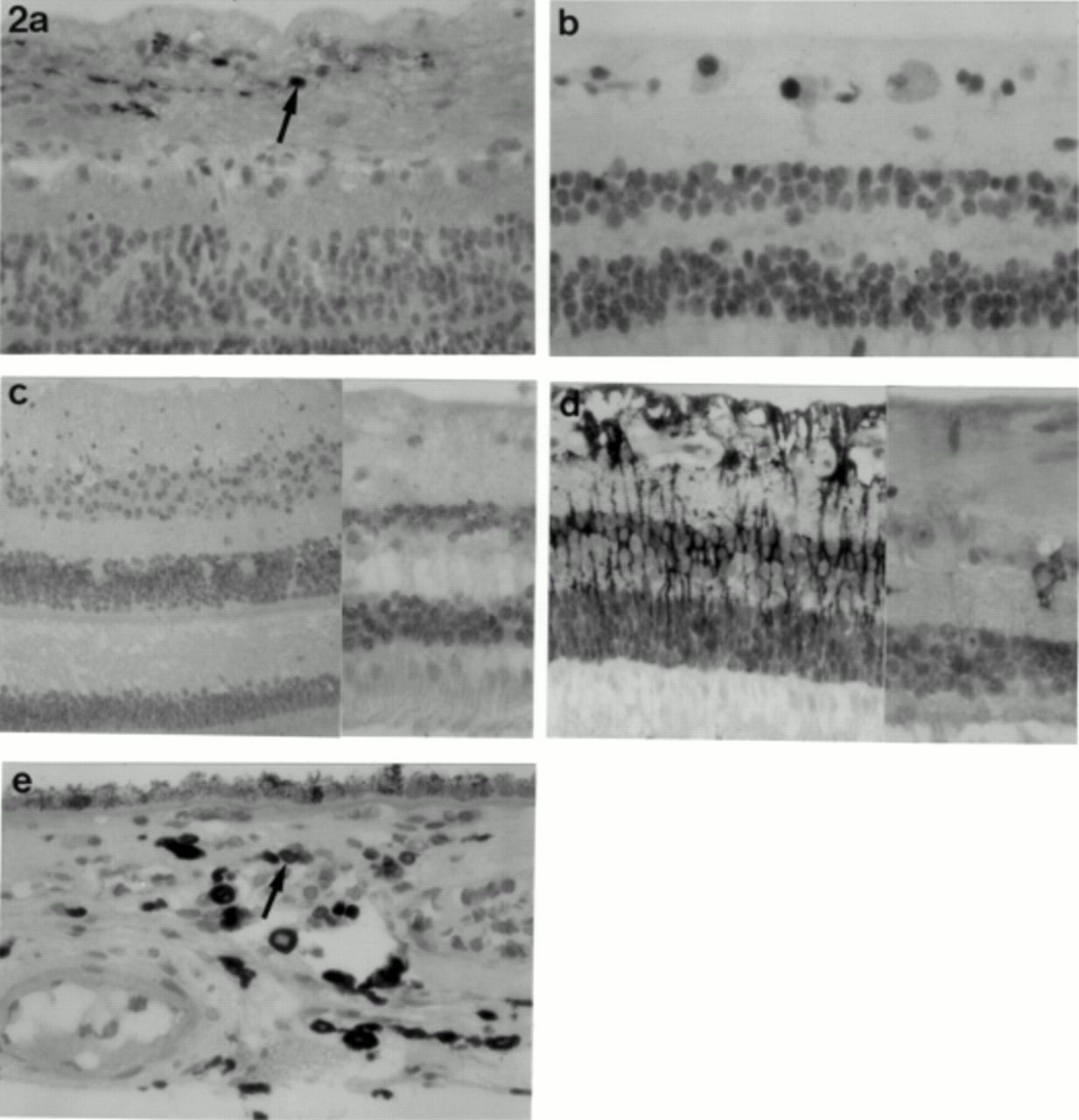
Cyclin D1 was observed in occasional ganglion cells of the normal retina (Fig 2a); a similar staining pattern was observed for p53 (Fig2b) and p16. Positive staining for pRB and p21 (Fig 2c) was observed in all cell layers of the normal retina. BCL-2 positivity was observed in scattered ganglion cells, the bipolar cells, and in perivascular astrocytes (Table 2) (Fig 2d).

Normal retina with (a) cyclin D1 staining in occasional ganglion cells (arrow) (×20 objective); (b) p53 positivity in scattered ganglion cells (×40 objective); (c) granular p21 staining in all cell layers of the retina (×20 and ×40 objective); (d) BCL-2 positivity in glial cells and, at the higher magnification, in occasional ganglion cells (×20 and ×40 objective). (e) Normal choroid with scattered BCL-2 positive reactive lymphocytes (arrow) (×40 objective); occasional melanocytes demonstrated weak BCL-2 positivity following bleaching (not shown).
The choroidal melanocytes were negative for cyclin D1, pRB, p53, and p16. Occasional melanocytes, as well as scattered reactive T and B lymphocytes, were positive for p21 and BCL-2 (Fig 2e) (Table 2).
Retinoblastoma
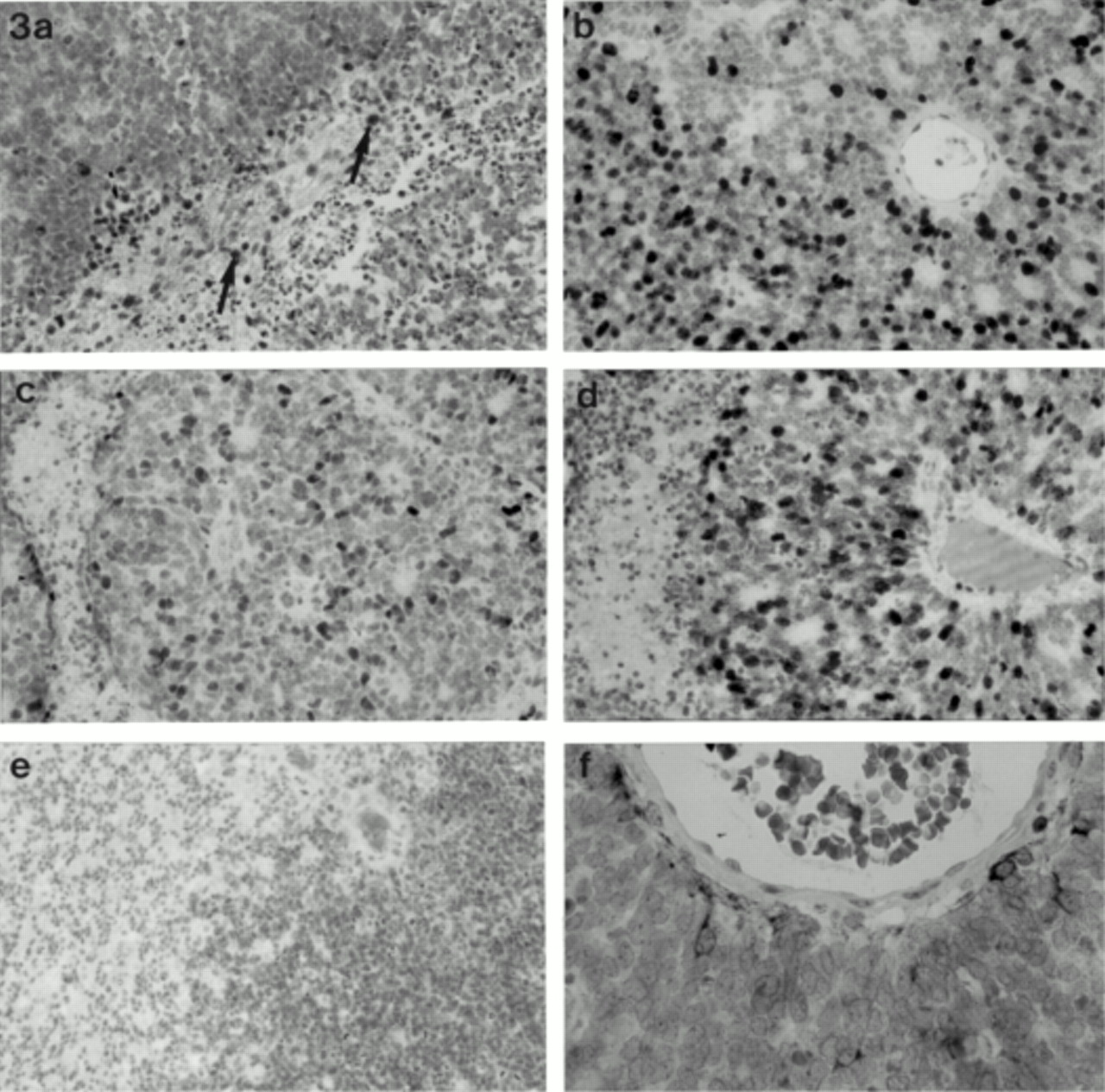
Cyclin D1 positive cells were rarely seen in retinoblastoma and when present corresponded to glial cells (Fig 3a), also positive for GFAP. Similarly, retinoblastoma cells were negative for pRB using the applied antibody, staining for pRB being observed only in vascular endothelial cells and some perivascular GFAP positive glial cells (Table 2). Excluding those retinoblastomas which had been treated with chemotherapy, radiation, or with a combination of the two before enucleation, most retinoblastomas demonstrated all three grades of cell differentiation. These were reflected to some extent by the growth fraction of the tumour cells as well as by the percentages of cells positive for the p53, p21, and p16. The highest proliferating cell populations were observed in the poorly differentiated areas with growth fractions of 60–90% (mean 80%). In the moderately and well differentiated areas, the growth fractions were significantly lower, averaging 30% and 5%, respectively (Fig 3b). Highest percentages of p53 positive cells (mean 60%) were observed in the poorly differentiated areas; lower percentages (mean 25%) in the moderately differentiated areas within the Flexner–Winterstein rosettes; and only scattered p53 positive cells were observed in the well differentiated areas. p21 positive tumour cells were observed in the poorly and moderately differentiated areas; occasional cells were positive for p21 in the well differentiated tumour areas (Table 2). The recently described zonal differentiation of p53 and p21 staining cells in pseudorosettes—p21 adjacent to the central blood vessel (zone 1) and p53 adjacent to the pseudorosette edge (zone 2)49—was observed in many retinoblastomas. A large proportion of pseudorosettes, however, demonstrated p53 and p21 positive cells in both zones (Fig 3c and d, respectively). p16 stained positively in high percentages in areas of poor and moderate differentiation (Fig 3e). Cells in zones 1 and 2 of the pseudorosettes were positive for p16. Only rare p16 positive cells were observed in well differentiated tumour areas.

(a) Cyclin D1 positivity in reactive glial cells (arrow) within retinoblastoma; the tumour cells are negative (×20 objective). (b) The degree of differentiation within the retinoblastomas is reflected by the corresponding MIB-1 growth fractions (×20 objective); (c) p53; and (d) p21 positivity surrounding a pseudorosette where staining of these markers is present in all “zones” (×40 objective); (e) p16 staining in poorly and moderately differentiated tumours areas within a retinoblastoma (×20 objective). (f) Perivascular glial cells positive for BCL-2 in a retinoblastoma; the tumour cells are negative (×40 objective).
Perivascular glial cells in areas of all grades of cellular differentiation were positive for BCL-2 (Fig 3f). Further, scattered or occasional groups of glial cells positive for BCL-2 were present between the tumour cells.
The nine retinoblastomas from patients treated with chemotherapy, chemoreduction, or radiation before enucleation demonstrated extensive calcification of the devitalised neoplastic cells, cystic degeneration, as well as reactive gliosis. Changes to retinoblastoma following treatment as well as those observed in adjacent ocular tissue have been described in more detail elsewhere.54 Three tumours demonstrated vital tumour with growth fractions of 10% in one case and 90% in the other two. Occasional vital retinoblastoma cells were positive for p53, p21, and p16; there was no alteration in the expression of these markers compared with the “untreated” tumours in the vital areas of the tumour. All post-treatment retinoblastomas were negative for cyclin D1, pRB, and BCL-2.
A correlation between the above G1-S cell cycle markers and the laterality of the tumours was not demonstrated.
Uveal melanomas
Forty five of the uveal melanomas arose from the choroid; 18 from the ciliary body; and one in the iris. Of the choroidal melanomas, 37 were posterior to, or close to the equator; eight tumours were anterior to this with no infiltration of the pars plana of the ciliary body. The uveal melanomas consisted of 21 spindle B, 29 mixed tumours with spindle B predominance, seven pure epithelioid tumours, and seven mixed tumours with epithelioid predominance. Extraocular extension of tumour was observed in nine cases.
Excluding those uveal melanoma which had been treated with radiotherapy before enucleation, nuclear positivity of cyclin D1 was observed in 85% of cases with the percentage of positive cells ranging between 2% and 75% (Table 2). The cyclin D1 percentage expression correlated positively with the growth fraction of the tumours which varied between 5% and 55% (p<0.05, Student’s t test). The percentage of cells positive for MIB-1 and cyclin D1 significantly correlated with cell type: pure or mixed epithelioid tumours demonstrated a greater percentage of MIB-1 and cyclin D1 positive cells than spindle cell tumours (p<0.05, respectively) (Fig 4a and b). Further, the percentage of cyclin D1 positive cells was greater in the anteriorly located tumours or those which showed extraocular tumour extension (p<0.05).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cyclin D1 positivity in a spindle (a) and epithelioid (b) choroidal melanoma (×20 objective). pRB positivity in a spindle (c) and epithelioid (d) choroidal melanoma (×20 objective). (e) Clear p53 positivity in choroidal melanoma (arrow) (×20 objective). (f) p21 staining in occasional tumour cells of a mixed cell choroidal melanoma (×20 objective). (g) p16 positivity in scattered tumour cells of a mixed cell choroidal melanoma (×40 objective). (h) BCL-2 staining in a spindle choroidal melanoma (×20 objective).
pRB tumour cell positivity varied between 5% and 65% (Table 2) and a significant correlation was observed between the percentage of cells expressing pRB and the MIB-1 growth fraction of the tumour (p<0.05). Further, a positive correlation existed between pRB and the cyclin D1 expression, the cell type (less in spindle cell tumours) (Fig 4c and d) and anatomical location of the tumour (higher percentage in the anteriorly located tumours) (p<0.05, respectively).
p53 expression was found in 60% of cases, with the percentage of positive cells varying between 2% and 30% (Fig 4e) (Table 2). Higher percentages of p53 positivity tended to occur in epithelioid cells; however, this was not statistically significant (p=0.09). Further, statistically significant correlations between p53 expression and the MIB-1 growth fraction, cyclin D1 and pRB positivity, and the tumour location were not observed.
Occasional tumour cells were positive for p21 in most cases (65%), range 5–30% (mean 8%) (Fig 4f). A statistically significant inverse relation between p53 and p21 was observed with a decreased p21 expression in tumours with high percentage p53 expression (p<0.05). Double staining demonstrated that p53 and p21 positive cells were distinct from one another (not shown). A significant correlation between p21 positive cells and the MIB-1 growth fraction, cyclin D1 and pRB positivity, tumour cell type or tumour location was not observed.
Immunohistochemical detection with p16 showed both nuclear and cytoplasmic staining in uveal melanoma; p16 cells were the scattered cells seen in 45% of cases and this positivity varied between 5% and 25% (mean 12%) of tumour cells (Table 2) (Fig 4g). There was no correlation with cell type, tumour location, or the percentage of cells positive for pRB. Double staining demonstrated exclusive staining for p16 and pRB in uveal melanoma.
All uveal melanomas stained for BCL-2, with no variation being observed between tumour location, tumour cell type (Fig 4h), MIB-1 growth fraction, cyclin D1, pRB, p53, p21, or p16 positivity. Despite bleaching procedures, slight variations in the intensity of the BCL-2 staining occurred in heavily pigmented tumours owing to the cytoplasmic location of the BCL-2 protein.
The nine uveal melanomas which had been treated with radiotherapy before enucleation demonstrated necrosis as well as a massive infiltration of melanomacrophages. The growth fraction of these tumours was significantly lower in comparison with untreated tumours, varying between 1% and 5%, mean 3% (p<0.05). Vital melanoma cells were positive for BCL-2 and, occasionally, for cyclin D1, pRB, p53, p21, and p16. There was no change in expression of these markers in the vital tumour areas compared with the “untreated” tumours.
Discussion
The present study represents the first immunohistochemical investigation and description of cyclin D1 protein expression in retinoblastoma and uveal melanoma. The two tumours were chosen for their differing retinoblastoma gene status in order to investigate the expression of cyclin D1 and related G1-S transition proteins dependent on pRB status. Recent studies on cell lines and data from in vitro systems have provided evidence for an autoregulatory loop between cyclin D1 and pRB in normal cells and tumour cells with a functional pRB (Fig 1).55 According to this model, transcription of cyclin D1 gene is stimulated by hypophosphorylated pRB in the early stages of G1 and is later repressed by its hyperphosphorylated form (Fig 1). Disruption of this loop has been proposed to occur in three ways. The first is the binding of DNA viruses to the pRB binding “pockets”55 and will not be further addressed here. The second is the mutation of the pRB molecule, which predominantly involves the pRB binding pockets.55 In human tumours with mutations in both alleles of the RB gene, functional pRB is absent and can no longer regulate transcriptional factors such as E2F. E2F is, thereby, freed from the pRB binding pockets and from the inhibitory regulation of pRB at inappropriate times and, consequently, cell proliferation is stimulated. Further, there is a decrease in the transcriptional stimulus of cyclin D1 by the mutated pRB.55 The third mechanism, by which the autoregulatory loop between pRB and cyclin D1 can be disrupted, is the overexpression of cyclin D1 by gene amplification, resulting in accelerated phosphorylation of pRB and the inactivation of its inhibitory effect on cell cycle progression.55 The exact mechanism by which cyclin D1 overexpression has its oncogenic effect is unclear. Two mechanisms have been proposed—by directly binding to pRB or by reducing the levels pRB in the cell.24 Both mechanisms have been recently questioned in studies on low grade B cell lymphomas.7
In the current study, retinoblastoma tumour cells were negative for cyclin D1 and pRB using the antibodies applied. Uveal melanoma cells, in contrast, demonstrated positivity for both cyclin D1 and pRB in varying percentages, with a positive correlation existing between these two markers (p<0.05), as well as with the growth fraction of the choroidal melanoma (p<0.05). Our data are in agreement with those of previous studies investigating tissue sections for pRB5657 and cell lines for cyclin D1.55 The absence of pRB and cyclin D1 protein staining in retinoblastoma cells may be explained by the above mentioned second mechanism leading to disruption of the autoregulatory loop between cyclin D1 and pRB. The cause of cyclin D1 overexpression in the uveal melanomas—for example, via a heterogeneous cyclin D1 gene promoter or via gene translocation, as in the case of mantle cell lymphoma, must be investigated further. The positive relation between cyclin D1 and pRB observed in choroidal melanoma, however, would tend to support the suggestion of Zukerberg and colleagues that cyclin D1 does not exerts its tumorigenic effect by pRB level reduction.7
Strong expression of p16, a protein which acts as a kinase inhibitor of the cyclin/CDK complexes, was observed in retinoblastoma in areas of moderate and poor differentiation. It was also demonstrated in pRB negative cells in 45% of uveal melanomas. The variable expression of p16 observed in uveal melanomas in the current study parallels to some extent the findings of Ohta et al who reported chromosomal abnormalities involving the p16 gene in 32% of cases examined.19 In general, the results of p16 expression in both tumour types are consistent with studies which have demonstrated high levels of p16 expression in cell lines with lack of pRB function58 and would support the proposal of a negative feedback system between the two proteins.5960Further, they are in agreement with the results of immunohistochemical investigations of other tumours where a reciprocal expression of p16 and pRB was demonstrated.6162 These current models do not explain, however, the absence of p16 expression in well differentiated areas of retinoblastomas (also negative for pRB). Together with biochemical analysis further investigations are presently being conducted with newer p16 antibodies, in order to underline the significance of the present findings.
Some variation exists between the previously reported investigations of p53 expression in uveal melanoma6364 and can most likely be accounted for by the differing fixation techniques, the differing p53 antibodies, as well as differing antigen retrieval techniques used. Such problems with p53 immunohistochemical investigations have been recently addressed in other human cancers in detail and the value of the immunohistochemical analysis alone as being indicative of mutations in the p53 gene has been questioned.65 In the current study, the majority (60%) of uveal melanomas demonstrated p53 positivity with cell percentages varying between 2% and 30%. Previous authors have reported 54%63 and 67%64 of cases of uveal melanomas being positive for p53. Details regarding the percentage of tumour cells positive for this marker were not given in the latter study. One group of investigators defined p53 overexpression as being greater than 10% and this was only observed in five patients, all of whom had been treated with preoperative telecobalt or ruthenium irradiation before enucleation.63 Although our results do not support such an association between p53 expression and irradiation, we agree with these authors’ observation that p53 positivity tended to be greater in epithelioid tumours.
The critical downstream effector of p53 specific pathway growth control, p21, was observed in both intraocular tumours in the current investigation. Further, the inverse relation between p53 and p21 protein expression described in normal tissue and in other tumours,26 could be demonstrated in some pseudorosettes within the retinoblastomas and in uveal melanomas. Nork and coworkers have recently proposed a zonal arrangement of p53 and p21 positive cells in tumour areas adjacent to pseudorosettes in retinoblastoma.49 The authors reported that zone 1, 2, and 3 cells surrounding the pseudorosettes have the highest staining of cells for p21, p53, and transferase mediated biotin dUTP nick end labelling, respectively and that an overexpression of p53 in zone 2 leads to the ultimate onset of apoptosis observed at the edge of the pseudorosette.49 Although a similar pattern for p53 and p21 staining was observed in some pseudorosettes in our tumours, such a strictly defined distribution of these two cell markers was not observed in all pseudorosettes and in all tumours. In the choroidal melanomas, p21 positivity decreased in tumours with a high percentage p53 expression. It would be expected from these results that, as a result of a decrease in the “arrest” function of p21, a positive correlation may exist between p53 expression and the MIB-1 growth fraction. Although such a correlation between p53 and proliferation markers has been observed in immunohistochemical investigations of other tumours,66-68 such a relation could not be demonstrated in this study. The only influence observable on the growth fraction of uveal melanomas was that of irradiation which resulted in a significant decrease in the MIB-1 growth fraction, as previously reported by other authors.69-71
Apart from its cell arrest inducing function, p53 is also involved in the induction of PCD; a direct correlation between p53 expression and apoptosis has been demonstrated in some tumours.34Retinoblastoma cells were negative for BCL-2, the antidote to PCD; perivascular glial cells and scattered astrocytes within the tumour islands only were positive for BCL-2. This absence of BCL-2, together with the extensive apoptosis observed in the majority of the retinoblastomas, would tend to support the suggestion of Norket al, that apoptosis in retinoblastoma is most likely p53 induced.49 Our findings, however, contrast with those of Yuge et al, who described weak positivity for BCL-2 in all retinoblastoma cells.57 The reasons for the discrepancy between results are not clear, although they are likely to be explained by the differing preparation of the slides before immunohistochemistry (hydrogen peroxide incubation; microwave antigen retrieval) as well as in the differing immunohistochemical techniques.57
Uveal melanoma cells, in contrast, were consistently positive for BCL-2, in agreement with previous results where BCL-2 positivity has been described in 100%72 and 90%73 of cases. BCL-2 is considered to have a specific role in the survival of melanocytes.74 Although a positive correlation between the oncogene c-myc and BCL-2 has been established in choroidal melanomas,73 there was no significant correlation between BCL-2 and any of the G1-S phase markers investigated in the present study. The interpretation of BCL-2 staining in uveal melanoma most likely requires the additional results of immunohistochemical staining patterns of other members of the BCL-2 family, such as BAX, which have to date been hampered by the unsuitability of available antibodies for formalin fixed paraffin embedded tissue sections.
In conclusion, retinoblastomas and uveal melanomas differ in their immunohistochemical pattern for cell cycle markers of the G1-S phase transition. Cyclin D1 protein expression is present in most uveal melanomas and absent in retinoblastomas, in agreement with the recently proposed autoregulatory feedback loop model proposed by Lukas and coworkers.55 A positive correlation exists between cyclin D1 cell positivity and tumour cell type, location, growth fraction, and pRB positivity in uveal melanoma. The results presented are based on immunohistochemical investigations onlyand require molecular biological studies to underline their significance. The presence of cyclin D1 overexpression in choroidal melanoma suggests that other mechanisms at the molecular level, such as a possible translocation or heterogeneous promoter of the cyclin D1 gene, may be involved in their tumorigenesis. It also remains to be determined whether the expression of these G1-S phase transition proteins, particularly of cyclin D1 protein, has a role in determining tumour behaviour—for example, the onset of tumour metastasis.
Acknowledgments
The authors thank Mrs Helga Zimmerman-Höffken and Mrs Heidrun Protz for their superb technical assistance.