Article Text

Abstract
AIMS To evaluate the efficacy of amniotic membrane transplantation (AMT) for ocular surface reconstruction.
METHODS 10 consecutive patients who underwent AMT were included. The indications were: group A, cases with persistent epithelial defect after corneal abscess (n=1), radiation (n=1), or chemical burn (n=3); group B, cases with epithelial defect and severe stromal thinning and impending or recent perforation, due to chemical burn (two patients, three eyes) or corneal abscess (n=2); group C, to promote corneal epithelium healing and prevent scarring after symblepharon surgery with extensive corneo-conjunctival adhesion (n=1). Under sterile conditions amniotic membrane was prepared from a fresh placenta of a seronegative pregnant woman and stored at −70°C. This technique involved the use of amniotic membrane to cover the entire cornea and perilimbal area in groups A and B, and the epithelial defect only in group C.
RESULTS The cornea healed satisfactorily in four of five patients in group A, but the epithelial defect recurred in one of these patients. After AMT three patients underwent limbal transplantation and one penetrating keratoplasty and cataract extraction. In group B amniotic membrane transplantation was not helpful, and all cases underwent an urgent tectonic corneal graft. Surgery successfully released the symblepharon, promoted epithelialisation and prevented adhesions in the case of group C.
CONCLUSION AMT was effective to promote corneal healing in patients with persistent epithelial defect, and appeared to be helpful after surgery to release corneo-conjunctival adhesion. Most cases required further surgery for visual and ocular surface rehabilitation. Amniotic membrane used as a patch was not effective to prevent tectonic corneal graft in cases with severe stromal thinning and impending or recent perforation.
- amniotic membrane
- cornea
- ocular surface
- epithelial defect
Statistics from Altmetric.com
Amniotic membrane is the innermost layer of the fetal membranes. It has a stromal matrix, a thick collagen layer, and an overlying basement membrane with a single layer of epithelium.1 Amniotic membrane has unique properties including antiadhesive effects, bacteriostatic properties, wound protection, pain reduction, and epithelialisation effects. Another characteristic of amniotic membrane is the lack of imunogenicity.2 Amniotic membrane has been used as a surgical material for several decades. Amniotic membranes have been used as a dressing to promote healing of chronic ulcers of the leg and as a biological dressing for burned skin and skin wounds.3-5 It has also been used in surgical reconstruction of artificial vagina, for repairing omphaloceles, and to prevent tissue adhesion in surgeries of the abdomen, head, or pelvis.6-10
The use of amniotic membrane transplantation (AMT) to treat ocular surface abnormalities was first reported five decades ago.11-13 The role of AMT in ocular disorders has been recently re-evaluated. Amniotic membrane has been successfully used in patients with persistent epithelial defects,14pterygium,15 symblepharon,16 and for ocular surface reconstruction.17-21 In this report we describe our experience with AMT to treat ocular surface abnormalities.
Materials and methods
All patients who underwent AMT at Queen’s Medical Centre from January 1996 to December 1997 were included in this study. The patients had diverse ocular surface abnormalities and were divided in three categories: group A (n = 5), patients with persistent epithelial defects; group B (n = 4), patients in whom the integrity of the eye was threatened by perforation or impending perforation and conservative measures such as the use of a soft contact lens and cyanoacrylate glue had failed to stabilise the situation; and group C (n = 1), cases with symblepharon (Table 1).
Demographics and clinical data
In group A patients developed persistent epithelial defects after chemical burn (n = 3), corneal abscess (n = 1), and radiation keratopathy (n = 1) (Table 1). All cases were initially treated with lubricants (hypromellose 0.3% without preservatives, hourly or every 2 hours, and liquid paraffin at bedtime). Surgery was indicated after lubricants failed to promote epithelial healing. In group B the cause of corneal ulcer was chemical burn (two patients, three eyes) and corneal abscess (n=2). In group C the patient (Table 1, patient No 10) had an extensive corneo-conjunctival adhesion and symblepharon after trauma.
Amniotic membrane was obtained under sterile conditions after elective caesarean delivery. The woman’s serum was negative for human immunodeficiency virus, syphilis, hepatitis B virus, or hepatitis C virus. Under a lamellar flow hood, the placenta was first washed free of blood clots with sterile saline. The inner amniotic membrane was separated from the rest of the chorion by blunt dissection (through the potential spaces between these two tissues), and rinsed in sterile saline (2 litres) and later in 4%, 8%, and 10% dimethylsulphoxide (DMSO) phosphate buffered saline (PBS) for 5 minutes each, successively. The membrane was then flattened onto a nitrocellulose paper, with the epithelium/basement membrane surface up. The amniotic membrane was then cut into 5 × 5 cm pieces. Each of them was placed in a sterile vial containing 10% DMSO medium. The vials were frozen at −70°C. The membrane was defrosted immediately before use by warming the container to room temperature for 10 minutes, and rinsed three times in saline.
After retrobulbar or general anaesthesia, in groups A and B debris from the base of the ulcer was removed. The epithelium adjacent to the edge of the ulcer was removed if loose. A 360° perilimbal conjunctival incision was done and the amniotic membrane was secured with interrupted 8-0 Vicryl sutures with episcleral bites around the limbus. Thus, the whole corneal surface was covered by the amniotic membrane. The basement membrane was on the outside (that is, epithelial side up), and the mesenchymal surface in contact with the cornea. After surgery a bandage contact lens was put in place, and discontinued after epithelialisation.
In patient No 10 (category C), after the removal of the conjunctival extension onto the cornea and subconjunctival scarring up to the episcleral surface, the amniotic membrane was fitted to cover the epithelial defect by trimming off the excess portion. This fashioned membrane was then secured to the corneal edge of the defect by interrupted 10-0 nylon sutures and to the conjunctival edge with interrupted 8-0 Vicryl sutures with episcleral bites.
Postoperative care consisted of preservative-free prednisolone acetate 1% eye drops four times a day and preservative-free chloramphenicol 0.5%, both tapered off in 1 month.
Results
The demographics and clinical data of the patients are summarised in Table 1.
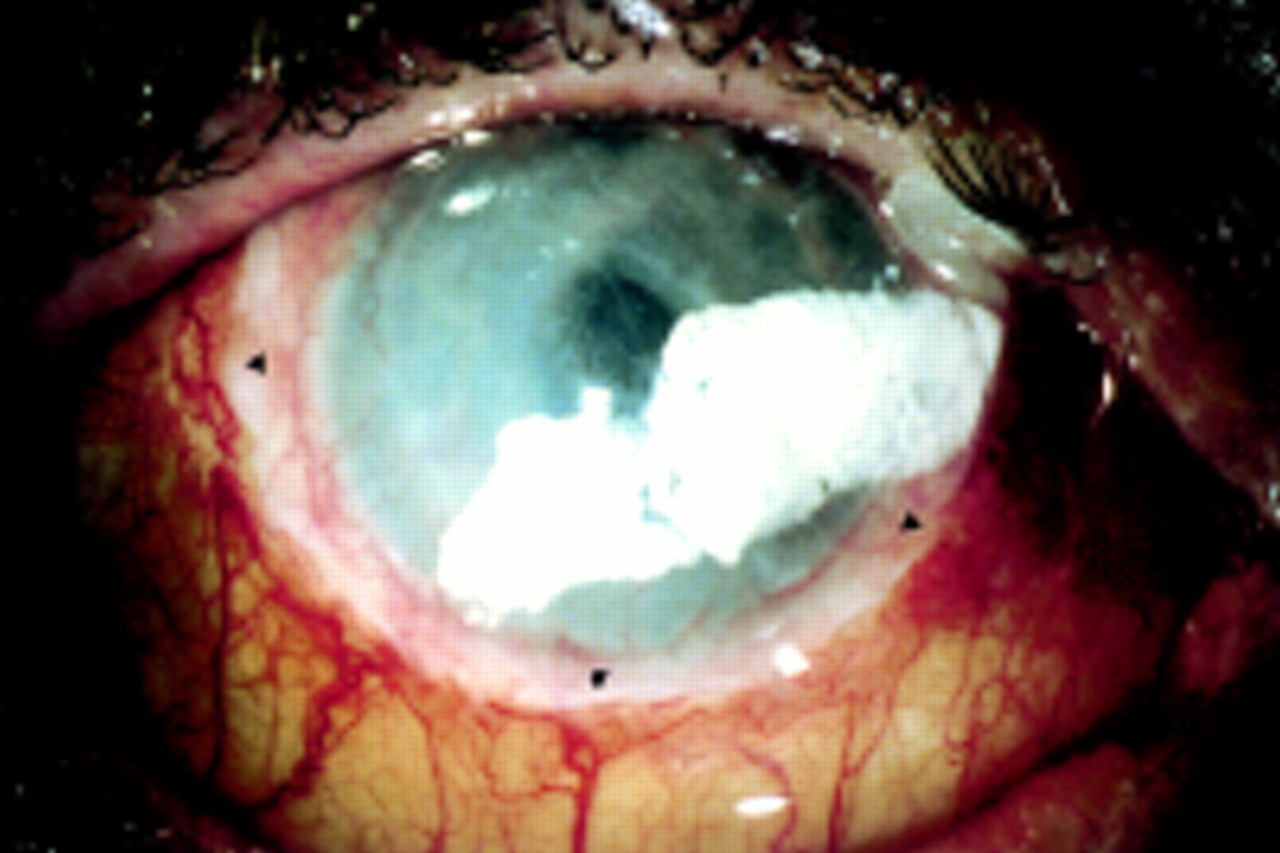
In group A, rapid corneal healing occurred in four of five cases 1–4 weeks after AMT (Figs 1 and 2). However, in patient 5 the epithelial defect recurred. The membrane dissolved within 2 months in all cases. In successful cases, epithelialisation apparently occurred underneath the amniotic membrane. After the membrane dissolved, the corneal epithelium phenotype appeared to be unchanged. Three patients (Nos 3, 4, and 5) underwent limbal transplantation after AMT (Table 1). In group B amniotic membrane did not help to stabilise the ulcer and after 1–3 weeks all cases underwent tectonic transplantation (Table 1). Patient No 10 (category C) had a successful ocular surface reconstruction, with the return of satisfactory mucosal appearance and release of adhesions (Table 1). Epithelialisation was rapid, and the resulting conjunctival surface remained stable 18 months after surgery, without inflammation or erosion.
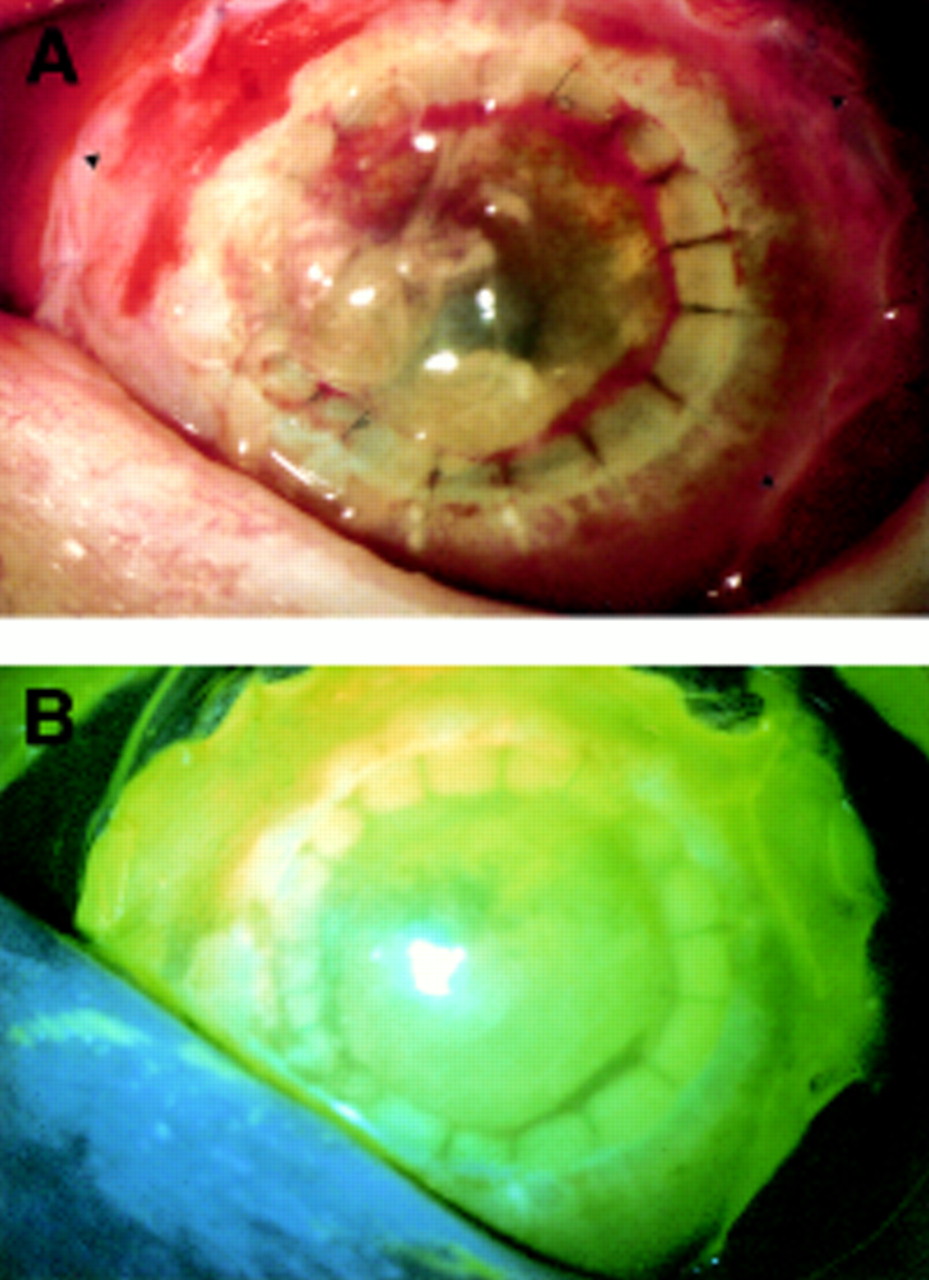
External photograph of case 2 in the early postoperative period after amniotic membrane transplantation. Arrowheads indicate the edge of the amniotic membrane posterior to the limbus (A). The amniotic membrane was stained with fluorescein (B).

{kind=link}
{kind=link}
External photograph of case 3, 3 weeks after amniotic membrane transplantation. Arrowheads indicate the edge of the amniotic membrane posterior to the limbus. There is a dense white opacity on the membrane, which was related to ciprofloxacine treatment.
Discussion
Persistent corneal epithelial defect may progress to persistent sterile corneal ulcer and, occasionally, to perforation. Common factors leading to the breakdown of the epithelial surface include infections, xerosis, trauma, and chemical injuries. Treatment of persistent epithelial defects consists of correction of the underlying cause and tissue lubrication. In cases refractory to medical treatment several options can be considered, including AMT.
Several characteristics explain why the amniotic membrane can be useful to promote epithelial healing. For example, the epithelium produces various growth factors, and the basement membrane facilitates migration of epithelial cells, reinforces adhesion of basal epithelial cells, and may promote epithelial differentiation.4 Lee and Tseng used amniotic membrane to treat persistent epithelial defects.14 Epithelialisation occurred in 10 of 11 consecutive patients. Recently, Tseng et alreported that the use of AMT was beneficial to restore the ocular surface in patients with partial limbal stem cell deficiency, but in severe deficiency associated limbal and amnion transplantation was required.18
In this study the amniotic membrane promoted rapid corneal healing in four of five patients with persistent epithelial defects. However, one of these cases could be considered as a relative failure because the epithelial defect recurred. It is likely that limbal stem cell deficiency, present in both non-successful cases, contributed to the lack of success. After AMT three patients underwent limbal transplantation to regenerate the ocular surface, and one case required surgery for visual rehabilitation. These results suggest that in patients with associated ocular surface abnormalities (such as diffuse limbal stem cell deficiency) AMT may be only useful as a temporary measure before other reconstructive surgical procedures. It is important to emphasise that AMT may be considered as an option only after intensive topical lubrication has failed to promote epithelial healing. Other alternatives such as tarsorrhaphy, punctal occlusion, botulinum toxin injection, punctal occlusion, tissue adhesive, or conjunctival flaps should be considered with an individualised criterion. A controlled clinical trial will be necessary to evaluate whether AMT has a better or worse outcome than conventional surgical options to treat persistent epithelial defects.
Non-infective corneal ulcers or infected ulcers rendered sterile with antibiotics can fail to epithelialise and lead to progressive stromal melting. In such situations commonly used surgical techniques are penetrating keratoplasty, lamellar keratoplasty, tarsorrhaphy, tissue adhesive, conjunctival flaps (in cases with poor visual potential), or a combination of these procedures. Other surgical procedures are aimed to correct mechanical insults to the ocular surface caused by eyelids abnormalities, enhance the ocular surface defence, replace the damaged corneal stroma, and promote healing with re-epithelialisation. Lamellar keratoplasty and penetrating keratoplasty are indicated when there is a risk of perforation. In this study, AMT was used to treat four patients (five eyes) with severe ulceration and impending or recent perforation. In all cases AMT failed to stabilise the cornea, an additional urgent tectonic procedure was undertaken. The amniotic membrane was sutured to episclera to cover the entire corneal surface. This tissue “patch” graft allows epithelial proliferation growth underneath the membrane; after a few weeks the amniotic membrane dissolves. Alternatively, the amniotic membrane can be sutured to the cornea to cover only the epithelial defect, acting as a substrate graft. In the latter option, proposed by Lee and Tseng, epithelialisation occurs over the membrane, which is incorporated into the corneal tissue.14 This alternative might be more helpful to build up the corneal thickness and to provide a healthy substrate in cases of severe ulceration and impending or recent perforation.
The antiadhesive properties of the amniotic membrane were also explored in one case. The surgery achieved its goal (that is, release of symblepharon, closure of corneal epithelial defect, and reconstruction of mucosal conjunctival mucosal surface with prevention of adhesions). Similarly, Shimazaki et al recently reported the successful use of AMT associated with limbal transplantation to treat four patients with recurrent pterygium associated with symblepharon.16 Several factors are involved in the antifibrotic effect of the amniotic membrane. Most importantly, there is inhibition and arrest in fibroblast proliferation following contact with normal substrates (that is, amniotic membrane). It has been shown that amniotic membrane induces a downregulation of transforming growth factor β signalling responsible for fibroblastic activation in wound healing (Tseng et al, unpublished data). Additionally, the amniotic membrane may also function as an anatomical barrier, keeping the potentially adhesive surfaces apart. Amniotic membrane has been also used by Tseng et alto reconstruct conjunctival defects created during surgical removal of a large lesion or during symblepharon lysis.17
In summary, AMT was useful in patients with persistent epithelial defects, although most cases required further surgery for visual and ocular surface rehabilitation. AMT when used as a patch graft was not effective to promote corneal stability in patients with severe stromal thinning. Its antiadhesive effects were helpful in reconstructing the conjunctival surface in one patient.
Acknowledgments
A Azuara-Blanco is the current Vision Express fellow in cornea and contact lenses.