Article Text

Abstract
AIMS To determine the relation between the stages of diabetic retinopathy (DR) and the levels of hepatocyte growth factor (HGF) and vascular endothelial growth factor (VEGF) in aqueous fluid and serum.
METHODS Levels of HGF and VEGF in serum and aqueous humour obtained during ocular surgery were measured by enzyme linked immunosorbent assay in 58 diabetic patients with 32 non-diabetic patients (NDM) as controls. The patients with diabetes were classified into three groups according to the stage of DR: no DR (NDR; 15 cases), non-proliferative DR (NPDR; six cases), and proliferative DR (PDR; 37 cases).
RESULTS No significant differences were found between any of the groups in serum concentrations of HGF or VEGF. The aqueous HGF levels increased with the stage of DR: NDM, median 397 pg/ml, range 133–930 pg/ml; NDR, 371 pg/ml, 142–1536 pg/ml; NPDR, 455 pg/ml, 162–1007 pg/ml; and PDR, 638 pg/ml, 187–2222 pg/ml. The aqueous VEGF levels in PDR (median 212 pg/ml, range 14–1216 pg/ml) were significantly higher than in NDM (105 pg/ml, 9–203 pg/ml), but aqueous HGF concentrations were unrelated to those of VEGF.
CONCLUSION The results of the present study suggest that both HGF and VEGF present in the ocular tissues may play important roles in the progression of DR.
- aqueous humour
- diabetic retinopathy
- hepatocyte growth factor
- neovascularisation
- vascular endothelial growth factor
Statistics from Altmetric.com
- aqueous humour
- diabetic retinopathy
- hepatocyte growth factor
- neovascularisation
- vascular endothelial growth factor
Proliferative diabetic retinopathy (PDR) is a major cause of adult blindness.1 Retinal capillary closure, a hallmark of this devastating disease, leads to tissue hypoxia and ischaemia, and neovascularisation of the retina develops adjacent to these areas of non-perfusion.2 3
Retinal ischaemia was postulated to induce the elaboration of angiogenic factors, resulting in retinal and iris neovascularisation,4 and a plethora of candidate angiogenic factors including acidic and basic fibroblast growth factors (a-FGF and b-FGF),5-7 transforming growth factor β,8 9 platelet derived growth factor,8insulin-like growth factor 1,10 tumour necrosis factor α,8 11 hepatocyte growth factor (HGF),7 9 12 13 and vascular endothelial growth factor (VEGF)11 12 14-16 have been identified as playing a role in PDR. The question of which of these factors, if any, functions to link retinal ischaemia with the pathological angiogenic response in PDR patients, however, has remained unanswered. Because blood vessel formation is a complex, multistep, process there may be several angiogenic factors, each of which operates under different circumstances, or the various factors may work together synergistically.
HGF, which is identical to scatter factor,17 is a disulphide linked heterodimeric molecule of 69 kDa containing an α chain and 34 kDa β chain.18 Its receptor is the c-met proto-oncogene product, a transmembrane tyrosine kinase.19Although HGF has been well characterised as a hepatotropic20 and a renotropic factor21 in liver and kidney regeneration, the presence of the local HGF system (HGF and its receptor, c-met) in endothelial cells and vascular smooth muscle cells has been demonstrated in vitro and in vivo.22Furthermore, recent studies have demonstrated that HGF is one of the endothelium specific growth factors, whose mitogenic activity is more potent than that of b-FGF, VEGF, interleukin 6 (IL-6), and IL-1.7 23 In addition, HGF levels in the vitreous fluid of PDR patients have been reported to be significantly higher than in non-diabetic patients.12
These findings prompted us to examine whether HGF plays a role in the progression of diabetic retinopathy (DR) in cooperation with VEGF, which is considered to be the most potent factor for retinal neovascularisation. Therefore, in the present study, we investigated the relation between the HGF and VEGF levels in the aqueous humour of diabetic patients and correlations between the levels of these factors and the stages of diabetic retinopathy.
Patients and methods
PATIENTS
Undiluted aqueous fluid samples were collected from patients who underwent eye surgery, including vitrectomy, cataract surgery, or both. All patients gave their informed consent. Specimens were obtained from 58 patients with diabetes mellitus (33–83 years old; mean age, 61.9 (SD 12.5)) and 32 patients without diabetes mellitus (34–86 years old; mean age, 72.4 (10.9)), who served as controls (NDM). None of the patients had neovascularisation of the iris or angle, and patients were excluded if they had undergone previous intraocular surgery or had a history of intraocular ischaemia due to causes other than DR, such as retinal vein occlusion. Exclusion criteria concerning systemic disease included: (1) ischaemic cardiovascular disorders; (2) ischaemic cerebrovascular disorders; (3) renal dysfunction (serum creatinine concentration over 2.0 mg/dl); (4) hepatic disorder (serum alanine aminotransferase over 32 IU/l, serum aspartate aminotransferase over 41 IU/l, or serum β guanosine 5′-triphosphate over 78 IU/l in males and over 42 IU/l in females, respectively); (5) history of malignancy; (6) hyperlipidaemia. These criteria were applied to all control subjects, whereas only (3), (4), and (5) were applied to the diabetics.
The levels of DR were determined by pre- or intraoperative fundus findings according to the early treatment of diabetic retinopathy study (ETDRS).24 Diabetic patients were classified as having no DR (NDR, n=15, 56–83 years old; mean age 68.9 (SD 9.0)), non-proliferative DR (NPDR, n=6, 64–82 years old, 71.7 (6.5)), or PDR (PDR, n=37, 33–81 years old; 57.5 (12.4)). Six patients with non-proliferative DR had mild or moderate non-proliferative DR and no severe non-proliferative DR. All 37 patients with PDR had high risk proliferative retinopathy.
SAMPLE COLLECTION
At the start of eye surgery, the sample of undiluted aqueous humour (100–200 μl) was manually aspirated into a disposable tuberculin syringe, transferred immediately to a sterile tube, and frozen immediately at −20°C in the operating room, and then transferred to a deep freezer at −70°C until assay.
HGF and VEGF levels in serum were also determined in all patients. For this purpose, blood samples were collected simultaneously with the eye surgery and centrifuged at 3000 g for 10 minutes to obtain serum, then aliquoted and stored at −70°C until assay.
HGF AND VEGF ANALYSIS
Concentrations of HGF in undiluted aqueous fluid and serum samples were measured by an enzyme linked immunosorbent assay (ELISA) for human HGF (Immunis, Institute of Immunology Co, Tokyo, Japan) according to the manufacturer’s standard protocol. In the assay, 100 μl of solution containing 50 μl of aqueous fluid or serum diluted with the phosphate buffer in the kit was used as a sample solution. Intra-assay coefficient of variation (CV) was 3.7%–5.0%, and interassay CV was 3.2%–5.7%. The limit of the assay was 100 pg/ml.
Concentrations of VEGF in undiluted aqueous fluid and serum samples were measured by an ELISA for human VEGF (Quantikine, R&D systems, Minneapolis, MN, USA) according to the manufacturer’s standard protocol. In the assay, 150 μl of solution containing 50 μl of aqueous fluid or serum diluted with the phosphate buffer in the kit was used as a sample solution. Intra-assay CV was 4.5%–6.7%, and interassay CV was 6.2%–8.8%. Samples with undetectable levels of VEGF were assigned a value of 9 pg/ml, the minimum level of detection.
STATISTICAL ANALYSIS
In view of the skewed distribution, all values are displayed as the median value and range, unless otherwise indicated. The significance of differences between groups was evaluated by the Kruskal–Walls test followed by Scheffe’s F test. Correlations between serum and aqueous concentrations of HGF or VEGF were studied by linear regression analysis. Linear regression analysis was used to assess the relation between concentrations of HGF and VEGF in aqueous fluid. The criterion for statistical significance was set at p<0.05.
Results
No significant differences were observed between any of groups in the serum HGF concentrations (p=0.37): NDM, median 217 pg/ml, range 108–367 pg/ml; NDR, 247 pg/ml, 119–441 pg/ml; NPDR, 282 pg/ml, 107–439 pg/ml; and PDR, 226 pg/ml, 122–432 pg/ml (Table 1). Nor were there any significant differences between any of the groups in the serum VEGF concentrations (p=0.25): NDM, median 210 pg/ml, range 87–830 pg/ml; NDR, 173 pg/ml, 64–367 pg/ml; NPDR, 141 pg/ml, 37–686 pg/ml; and PDR, 224 pg/ml, 65–670 pg/ml (Table2).
HGF concentrations
VEGF concentrations
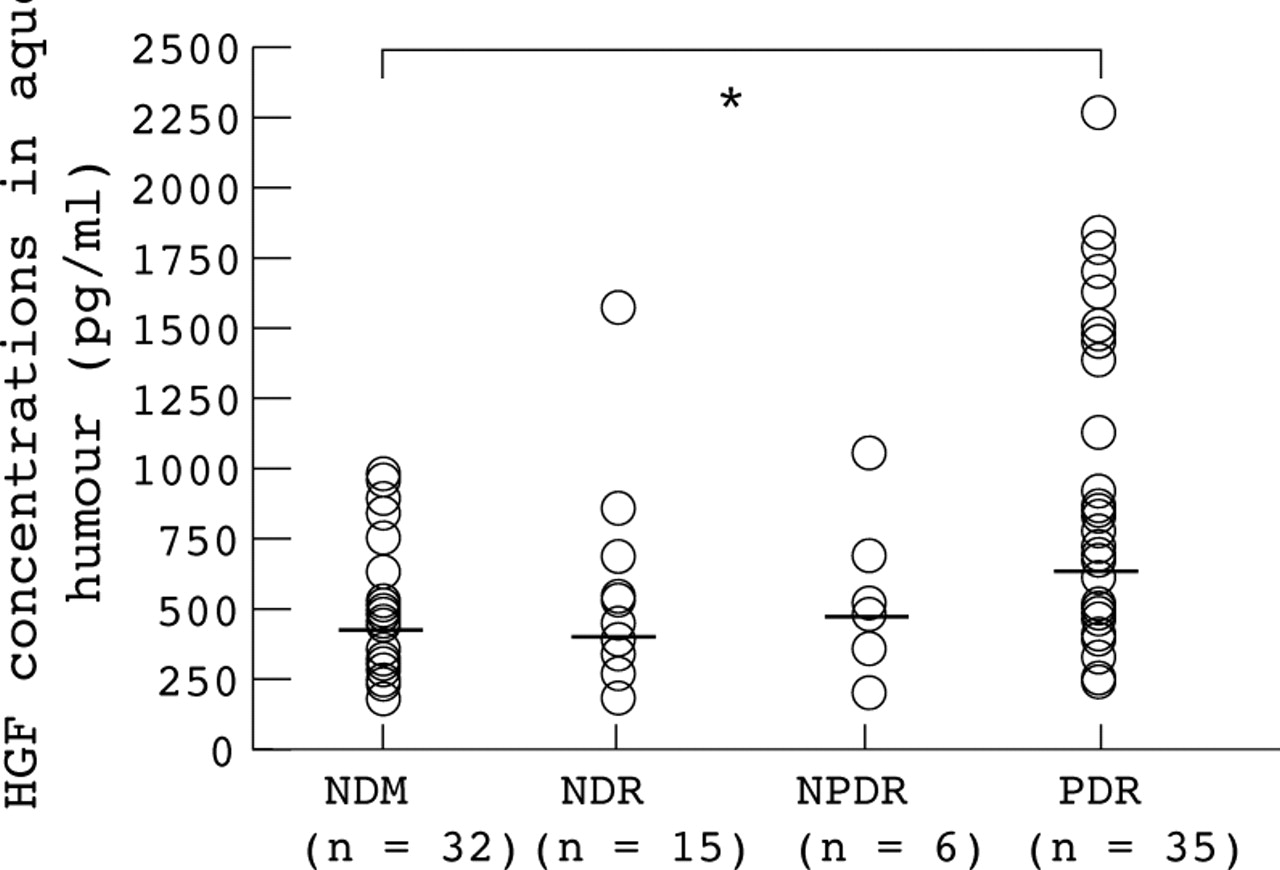
In contrast, the aqueous HGF level increased with the stage of DR (p=0.004): NDM, median 397 pg/ml, range 133–930 pg/ml; NDR, 371 pg/ml, 142–1536 pg/ml; NPDR, 455 pg/ml, 162–1007 pg/ml; and PDR, 638 pg/ml, 187–2222 pg/ml (Fig 1). The aqueous VEGF level in PDR (median 212 pg/ml, range 14–1216 pg/ml) was significantly higher (p<0.001) than in NDM (105 pg/ml, 9–203 pg/ml, p=0.02) and NDR (99 pg/ml, 13–189 pg/ml, p=0.004), and although not statistically significantly (p=0.24), it was also higher than in NPDR (77 pg/ml, 31–325 pg/ml) (Fig2).

The relation between the stages of diabetic retinopathy and the aqueous HGF levels. Aqueous concentrations of HGF in non-diabetic control subjects (NDM) and in diabetic patients without retinopathy (NDR), with non-proliferative diabetic retinopathy (NPDR), and with proliferative diabetic retinopathy (PDR). *p<0.05. The aqueous VEGF level in PDR was significantly higher (p<0.05) than in NDM.

{kind=link}
{kind=link}
The relation between the stages of diabetic retinopathy and the aqueous VEGF levels. Aqueous concentrations of VEGF in non-diabetic control subjects (NDM) and in diabetic patients without retinopathy (NDR), with non-proliferative diabetic retinopathy (NPDR), and with proliferative diabetic retinopathy (PDR). **p<0.01. The aqueous VEGF level in PDR was significantly higher than in NDM (p<0.001) and NDR (p=0.004).
However, there was no significant correlation between the aqueous humour concentrations of HGF and VEGF in samples from the patients with diabetes mellitus in each group: NDR (r=0.04), NPDR (r=0.33), PDR (r=0.29). No was there any significant correlation between the serum concentrations of HGF and VEGF in the samples from patients with diabetes mellitus in each group: NDR (r=0.54), NPDR (r=0.10), PDR (r=0.14).
No correlation was found between the concentrations of HGF in the aqueous humour and serum in either the diabetic patients (r=0.03) or the control subjects (r=0.30). The concentrations of HGF in the aqueous fluid were higher than in the serum in all of the diabetic patients (Table 1). No correlation was found between the concentrations of VEGF in the aqueous humour and the serum in either the diabetic patients (r=0.11) or the control subjects (r=0.10).
Discussion
The levels of both HGF and VEGF in the present study were lower than the vitreous levels reported by other investigators.12 15 This may be due to anterior/posterior gradients in the eye and/or the rapid clearance of these growth factors from anterior chamber.25
In the present study, we found no significant difference between any of the groups in the concentrations of serum VEGF, and there were no significant correlations between the concentrations of VEGF in the aqueous humour and serum of the patients with diabetes mellitus, which is in good agreement with an earlier report.14 In addition, Katsura et al 12reported finding no correlation between vitreous VEGF levels in the right and left eye in the same patient upon examining 12 patients who underwent vitreous surgeries for PDR in both eyes. These findings suggest that the vitreous concentrations of VEGF are not determined by serum concentrations in the presence of diabetic retinopathies and that intraocular synthesis of VEGF is the main contributing factor to the high VEGF concentration in ocular fluid observed in patients with PDR.
Although advancing levels of non-proliferative DR have been associated with increased levels of VEGF,26 27 aqueous levels of VEGF in NPDR were not so high in our study. This may be due to the mild to moderate severity of non-proliferative DR in our patients. Some investigators12 25 have reported higher intravitreous VEGF concentrations in active PDR than in quiescent PDR, suggesting that VEGF plays a major role in mediating active intraocular neovascularisation. In addition, VEGF not only stimulates development of new retinal vessels but has also been shown to play an important role in an early stage of DR as a stimulator of microaneurysm formation and capillary occlusion with ischaemia,28 as well as a promoter of increased vascular permeability.27 29 The finding that the aqueous VEGF levels in PDR were higher than in NDM, NDR, and NPDR in the present study is consistent with the observations of several other investigators.16 This may have been affected in part by blood-ocular barrier breakdown or increased vascular permeability. This result suggests that VEGF plays a very important role in a later stage of DR. In contrast with the results reported by Nishimura et al,13no significant differences between any of the four groups in serum HGF concentrations were found in the present study. Recent studies have shown that serum HGF levels are associated with various factors such as systolic pressure,30 serum uric acid concentrations,13 31 serine protease,32TGF-β, and angiotensin II.33 Moreover, sparse high values were obtained in our own data as well as that of others,13 reflecting great interindividual variability. Therefore, our results may differ from those of others13owing to differences in case selection and/or interindividual variability.
There was no significant correlation between the concentrations of HGF in the aqueous humour and serum of the diabetic patients. It is unknown whether the increased concentrations of HGF in the aqueous humour were due to enhanced production in extraocular organs, such as the liver, kidney, or spleen, promoting neovascularisation in the retina and/or in the eye itself. After 70% partial hepatectomy in rats, HGF messenger ribonucleic acid (mRNA) levels in the kidney and spleen increase threefold to fivefold,34 and HGF mRNA in the spleen is increased after the onset of renal injury caused by unilateral nephrectomy.35 HGF produced in uninjured organs may be involved in the regeneration of liver or kidney through an endocrine mechanism.36 These recent studies suggest that the increased concentrations of HGF may have been mainly attributable to production in extraocular organs. Our results, however, suggest another possibility—that increased concentrations of HGF were caused by its production in the eyes. Although VEGF37 and HGF38 are reported to be produced by some cells of ocular tissues, the sites of HGF production and/or receptors in the diabetic eye are not fully understood. Further investigations are required to clarify this.
In the present study, aqueous HGF levels were found to increase with the stage of DR, and no relation was found between the concentrations of VEGF and HGF in the aqueous humour and the serum of the diabetic patients. Katsura et al 12reported findings that the vitreous fluid HGF levels of PDR patients were higher than in non-diabetic patients and became elevated in the active PDR stage. Their study also showed that vitreous concentrations of HGF were unrelated to those of VEGF. In addition, Nakamuraet al 7 reported that HGF is more efficacious in stimulating the growth of vascular endothelial cells than other growth factors such as VEGF, bFGF, and IL-6. They9 also reported that HGF acts in an additive manner with bFGF, but not with VEGF. Therefore, our results support the description of Katsura et al 12 that HGF also plays an important part in neovascularisation in PDR and that the roles and induction mechanism may differ from those of VEGF. However, further investigations are necessary to specify the mechanism.