Article Text

Abstract
BACKGROUND/AIM The pathogenesis of visual field loss associated with macular hole surgery is uncertain but a number of explanations have been proposed, the most convincing of which is the effect of peeling of the posterior hyaloid, causing either direct damage to the nerve fibre layer or to its blood supply at the optic nerve head. The purpose of this preliminary prospective study was to determine the incidence of visual field defects following macular hole surgery in cases in which peeling of the posterior hyaloid was confined only to the area of the macula.
METHODS 102 consecutive eyes that had macular hole surgery had preoperative and postoperative visual field examination using a Humphrey's perimeter. A comparison was made between two groups: I, those treated with vitrectomy with complete posterior cortical vitreous peeling; and II, those treated with a vitrectomy with peeling of the posterior hyaloid in the area of the macula but without attempting a complete posterior vitreous detachment. Specifically, no attempt was made to separate the posterior hyaloid from the optic nerve head. Eyes with stage II or III macular holes were operated. Autologous platelet concentrate and non-expansile gas tamponade was used. Patients were postured prone for 1 week.
RESULTS In group I, 22% of patients were found to have visual field defects. In group II, it was possible to separate the posterior hyaloid from the macula without stripping it from the optic nerve head and in these eyes no pattern of postoperative visual field loss emerged. There were no significant vision threatening complications in this group. The difference in the incidence of visual field loss between group I and group II was significant (p=0.02). The anatomical and visual success rates were comparable between both groups.
CONCLUSION The results from this preliminary study suggest that the complication of visual field loss after macular surgery may be reduced if peeling of the posterior hyaloid is confined to the area of the macula so that the hyaloid remains attached at the optic nerve head. The postoperative clinical course does not appear to differ from eyes in which a complete posterior vitreous detachment has been effected during surgery.
- macular hole
- visual field loss
- optic nerve
Statistics from Altmetric.com
Visual field defects are a recognised complication of macular hole surgery.1-4 It is suggested that macular holes are the result of tangential vitreomacular traction.5 6 This has led to the use of vitrectomy, posterior cortical vitreous peeling, and gas tamponade, as first described by Kelly and Wendel,7 to promote flattening of the neurosensory rim and closure of the hole. Stripping of the posterior hyaloid, which is considered a requisite part of the procedure, is however purported to be a likely aetiological factor in the development of visual field defects in these patients.8 9
We report a consecutive series of 102 eyes in 100 patients who underwent macular hole surgery, and document postoperative visual field changes. We describe two groups—those treated with vitrectomy, posterior cortical vitreous peeling, autologous platelet concentrate, and gas tamponade; and those treated with vitrectomy, posterior cortical vitreous peeling confined to the area of the macula but not at the optic disc, autologous platelet concentrate, and gas tamponade.
Patients and methods
We report on a prospective non-randomised study of 102 consecutive procedures in 100 patients. Two patients had both eyes operated. Patients were included in the study if they had either a stage II or III macular hole, no other significant ocular disease, and had symptoms for less than 1 year. The study reports on two groups: group I comprised 82 eyes in which complete posterior cortical vitreous peeling was performed, while group II comprised 20 eyes in which the peeling of the posterior cortical vitreous was restricted to the area of the macula.
Preoperatively, a complete ocular examination was performed, including best corrected Snellen visual acuity, intraocular pressure measurement, assessment of lens clarity, slit lamp biomicroscopy, contact lens examination of the fundus, and fundus fluorescein angiography. All patients had preoperative Humphrey Esterman monocular suprathreshold visual field testing.
Seventy six patients were female and 24 were male. They ranged in age from 21 to 85 years, mean 65 years. Macular holes were staged according to the criteria outlined by Gass,5 6 and this staging was confirmed at the time of surgery. There were 25 (24.5%) stage II and 77 (75.5%) stage III holes. There was no significant difference in stage distribution between group I and group II cases (p=0.38). Preoperative visual acuity was 6/18 or less in all patients.
All patients were operated on by the same surgeon. Three port pars plana vitrectomy was performed in all eyes. In group I, the posterior cortical vitreous was detached either by aspiration with the vitreous cutter or silicone tipped cannula and the vitreous peeled as far out peripherally as possible. Cortical vitreous detachment was then confirmed using aspiration with a silicone tipped cannula.
In group II, the inner cortical vitreous was removed over the post-equatorial retina using a vitreous cutter but without attempting any traction on the vitreous to peel the posterior hyaloid. Careful vitrectomy on the surface of the retina was then performed over the macula and this was usually sufficient to remove the posterior hyaloid from the area of the macula. Aspiration with a silicone tipped cannula was subsequently used to test for the presence of vitreous attachment at the macula and the optic disc. In cases where the vitreous was still attached at the macula, it was carefully peeled with the silicone tipped needle from the macula out to the arcades but not from the optic disc, and it was then excised with the vitreous cutter. The posterior vitreous was not removed over the optic disc, and its presence at this site was confirmed using aspiration with a silicone tipped cannula.
Peeling of epiretinal or internal limiting membranes was not performed and fluid was not drained through the hole in any case. In all patients, before air/fluid exchange, careful examination of the peripheral fundus was performed to discover any induced retinal tears. Following air/fluid exchange, 10 minutes were allowed for peripheral fluid to drain posteriorly, this was then aspirated. Autologous platelet concentrate (0.1 ml) was then placed on the macula and an air-gas exchange was performed. In group I 23% SF6 gas was used in 35 eyes and 14% C3F8 was used in 47 eyes. In group II the intraocular gas used was 23% SF6. Patients lay supine for 4 hours, then prone for 7 days.
Platelets were prepared in the manner described by Gaudricet al.10 Immediately before the procedure, 40 ml of venous blood was taken from the patient. This was mixed gently with 6 ml of acid citrate dextrose (ACD). The mixture was then centrifuged at 280 g for 15 minutes and the platelet rich plasma decanted. The plasma was mixed with 1/8 volume ACD and further centrifuged at 1000 g for 10 minutes. The packed platelets were then mixed with 0.6 ml of sodium chloride to achieve a platelet suspension. The preparation of platelets was performed entirely in the operating theatre.
All patients have a minimum follow up of 6 months. Postoperative assessment was carried out at 1, 3, 6, and 12 months postoperatively, and included best corrected Snellen visual acuity, intraocular pressure measurement, assessment of lens clarity, slit lamp biomicroscopy, contact lens examination of the fundus. All patients had preoperative and postoperative fundus fluorescein angiography. Humphrey Esterman monocular suprathreshold visual field testing was performed in all eyes preoperatively and at 1 and 3 months postoperatively. Visual field testing was repeated at 6 and 12 months in those eyes which developed any form of scotoma in order to examine for any resolution or progression.
Results were analysed statistically using Fisher exact (two tailed p values), Student's t testing, and χ2 analysis. Visual acuity measurements were converted to logMAR to compare means.
Results
Preoperative visual acuity ranged from 6/18 to 3/60. Postoperatively, there was the appearance of a white “coagulum” over the posterior pole, and covering the hole. This material slowly disappeared over the subsequent 1–2 weeks. Cases were considered an anatomical success if the subretinal fluid surrounding the hole resolved and the retina flattened.
In group I the macular hole was closed in 91% (75) of cases. Postoperative visual acuity ranged from 6/6 to 3/60 (median 6/18). Overall 63% of patients had a final visual acuity of 6/18 or better, 38% had 6/12 or better, and 18% had 6/9 or better. Snellen visual acuity improved by two lines or more in 56 (68%) patients. Five eyes (6%) developed retinal tears which were treated intraoperatively. Three eyes (4%) developed retinal detachments and these were treated successfully.
In group II there was separation of the posterior hyaloid from the macula in all eyes. Spontaneous detachment of the hyaloid from the optic disc occurred during vitrectomy in two eyes. Retinal tears were not identified during surgery in group II. Two eyes were complicated by retinal detachment postoperatively. One of these had an area of lattice degeneration surrounding a retinal tear which was treated with argon laser preoperatively, and a superior retinal detachment developed from a hole within the lattice postoperatively. In the other patient retinal detachment arose as a result of a small round hole in the periphery: spontaneous separation of the posterior hyaloid had occurred in this eye during vitrectomy. In both eyes the macula was not detached and the hole was closed at the time of retinal detachment surgery. These cases were treated successfully and had postoperative visual acuities of 6/12 and 6/18 respectively. Closure of the macular hole was obtained in all 20 eyes in group II. Postoperative visual acuity ranged from 6/9 to 6/60 (median 6/18). Overall 60% of patients had a final visual acuity of 6/18 or better, 35% had 6/12 or better, and 25% had 6/9 or better. Snellen visual acuity improved by two lines or more in 14 (70%) of patients. Anatomical and visual success were comparable between the group I and group II and a significant difference was not found (p=0.44).
Postoperative intraocular pressure spiking occurred in six patients from the cohort, five from group I and one from group II. In all six eyes the intraocular pressure spikes were below 33 mm Hg and had a maximum duration of 36 hours. Visual field loss did not occur in any of these patients.
VISUAL FIELD DEFECTS
None of the group II cases produced any pattern of visual field loss. Occasional points were missed postoperatively in a few patients, as shown in Figure 1; however these were single non-contiguous points located in the far periphery and were absent on repeat testing.

An example of a postoperative monocular Humphrey Esterman visual field perimetry from a patient in group II, where the posterior hyaloid remains attached at the optic nerve head.
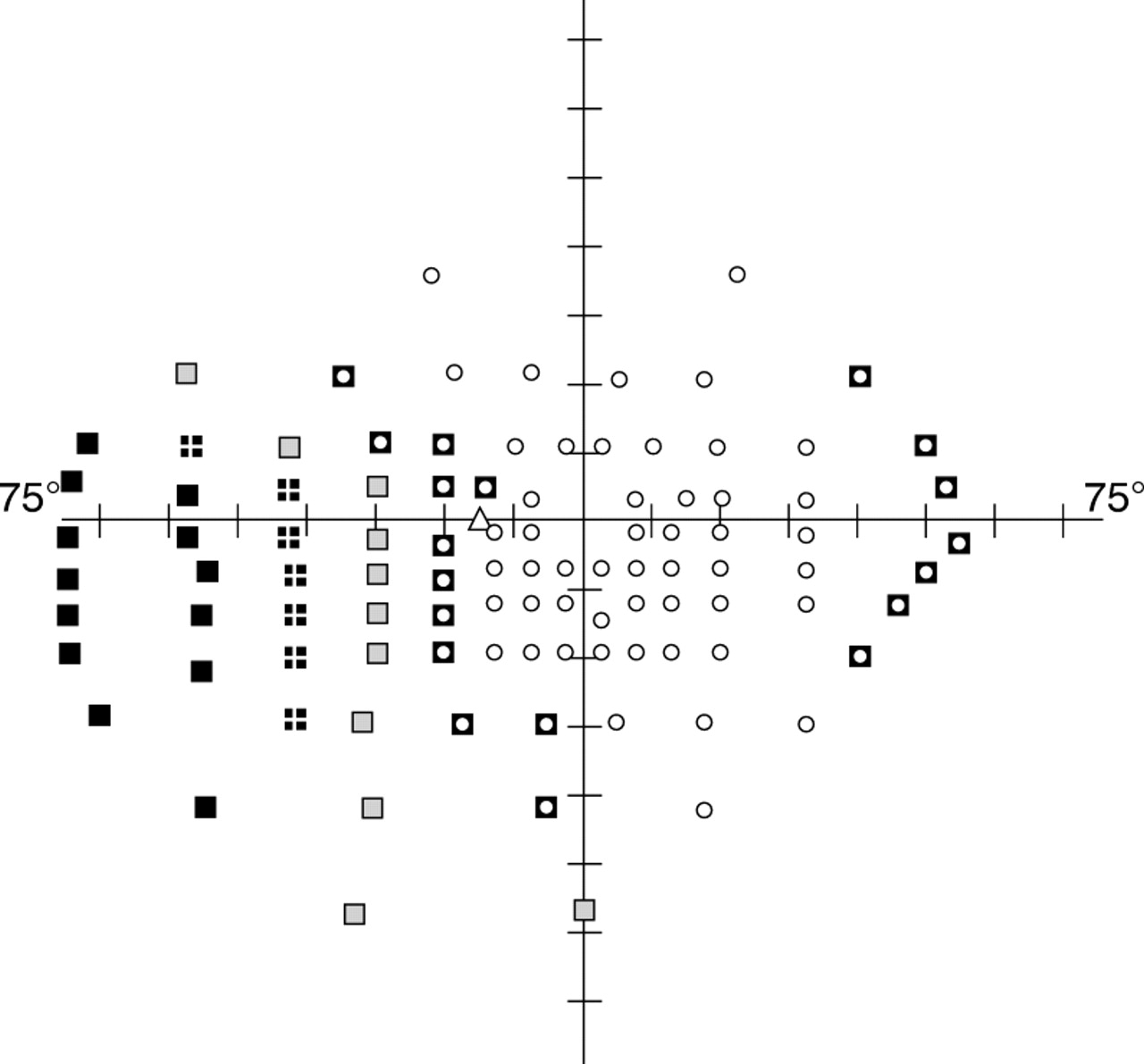
In group I, 22% of patients (18 eyes) were found to have visual field defects, a typical example of which is shown in Figure 2. Thirteen of the 18 patients with visual field loss were symptomatic and many of these were aware of the scotoma as soon as the gas bubble absorbed. Figure 3 illustrates the pattern of visual field loss showing a composite of points not seen on Esterman visual field analysis from all 18 patients with field defects. We found that the mean number of points not seen was 27 (±2 SEM) in these eyes. The pattern of field loss exhibits an absolute, dense, peripheral, temporal, and inferotemporal scotoma which extends above and below the horizontal, in all eyes. Overall, the difference in the incidence of visual field loss between group I and group II attained statistical significance (p=0.02). In group I visual field loss occurred in seven of the 35 eyes where SF6 was used and in 11 of the 47 eyes where C3F8 was used. Again, the difference between these individual subgroups and group II was statistically significant (p=0.026: C3F8 subgroupv group II; p=0.04: SF6 subgroupv group II). The incidence of visual field loss between the SF6 subgroup (20%) and the C3F8 subgroup (23%) were comparable and failed to reach a statistically significant difference.

Monocular Humphrey Esterman visual field from a patient in group I, following macular hole surgery where the posterior hyaloid was stripped from the optic nerve head. This illustrates the typical inferotemporal quadrant defect found in this group.

Composite pattern of overlapping visual field loss from all 18 patients in whom visual field defects occurred in group I. Black boxes indicate the common points missed by all 18 patients (100%) with field loss. Crossed boxes show points missed in >75% (14–17) of these eyes. Hatched boxes correspond to points missed in >50% (9–13), and centre circle boxes represent the points not seen in < 50% of eyes (<9).
It is possible with the Esterman visual field programme to score the number of points seen at each examination, thus enabling numerical quantification of visual field loss. Using this analysis we examined the difference in visual field loss by comparing Esterman efficiency scores between the two groups. The overall mean incidence of points missed in group I was 5.97 (SEM 1.33), whereas in group II this was 0.6 (0.41). The difference between the number of points not seen between these two groups was highly statistically significant (p<0.001,t=3.86), using unpaired Student'st test.
Discussion
Visual field defects are a recognised complication of macular surgery for the treatment of macular holes and subfoveal choroidal neovascular membranes, and it is suggested that visual field defects are caused by the additional manoeuvre of stripping the cortical vitreous from the optic nerve head.2 8 9 While it is generally accepted that posterior hyaloid removal is necessary over the macula in the repair of macular holes, whether it is necessary to remove the cortical vitreous from the surface of the optic disc is unknown.
In order to examine if the stripping of the posterior hyaloid is an aetiological factor in the development of visual field loss we developed a technique of repairing macular holes by vitrectomy and posterior hyaloid removal at the macula, but without separation of the post-cortical vitreous at the optic nerve head.
We have shown that there is a significant reduction in the incidence of visual field loss in eyes that did not undergo posterior hyaloid separation at the optic disc. While it was possible to leave the posterior hyaloid attached to the optic nerve head in the majority of cases, in two eyes spontaneous detachment of the posterior hyaloid occurred without traction during the vitrectomy. In these eyes the posterior hyaloid was only tenuously adherent at the optic nerve head and such cases may perhaps be less likely to develop visual field loss. The anatomical success in group II (100%, 20 eyes) was comparable with group I (91%, 75 eyes). Overall visual success was also similar, with a two Snellen line improvement in visual acuity in 70% (14 eyes) in group II, and 68% (56 eyes) in group I.
The recognised complications of macular hole surgery occurred in both groups. Retinal tears occurred during surgery in 6% of group I, but none was found in group II, although this difference failed to reach statistical significance (p=0.59). The omission of a complete surgical posterior vitreous detachment in group II may exert a protective effect to reduce intraoperative retinal tears. Retinal detachment is the most serious complication that may be encountered as a result of macular hole surgery.11 Retinal detachment in the group II eyes with incomplete separation of the posterior hyaloid may arise from two potential mechanisms. Firstly, the presence of an expansile gas bubble in an incompletely vitrectomised eye may induce upward traction on the inferior retina leading to the formation of peripheral retinal tears.12 Secondly, spontaneous detachment of the remaining cortical vitreous at a later stage, in these eyes where the central posterior vitreous has previously been removed, may result in peripheral retinal breaks and subsequent detachment; however, this has not occurred within the time frame of our follow up.
In this study, retinal detachment occurred in two eyes from group II. One of these had an area of lattice degeneration with retinal holes in the superior retina, treated preoperatively with laser. Two weeks postoperatively, after absorption of the gas bubble, the superior retina containing the area of lattice and retinal hole detached, not involving the macula and probably as a result of vitreous gel traction on the retina anterior to the lattice degeneration. The other eye that developed a retinal detachment was one of the two eyes in the study that had a spontaneous separation of the posterior hyaloid from the retina and optic nerve head during vitrectomy. Both eyes were treated successfully with good visual outcome. It has been recommended that a more complete vitrectomy may reduce the rate of postoperative retinal detachments.13 In this study, although the surgical technique was directed at not separating the posterior hyaloid from the optic nerve head, every effort was made to remove as much vitreous gel as was possible in order to reduce any tractional effects from the gas bubble.
Our results in this small series suggest that with this technique the incidence of retinal detachment occurring after macular hole surgery is not any higher than in the eyes in which the posterior hyaloid was separated from the optic nerve head. Furthermore, in a recent series of submacular surgery, in which the posterior hyaloid was not detached and a non-expansile gas bubble was used for postoperative tamponade of the retinotomy, Berger et al reported an incidence of retinal tears in 1.6% and retinal detachment in only 3% of cases.14
To assess visual field loss we used the Esterman visual field programme because the typical visual field defect occurred outside the central 30° zone, and would thus not be detected by standard Humphrey central visual field examination. In group I, where forced separation of the posterior hyaloid was performed, 22% of patients (18 eyes) were found to have visual field defects, an incidence which is comparable with findings from other groups.15 16 Figure 3 illustrates a composite of points missed on Humphrey Esterman visual field analysis combined from all 18 patients with field defects. The pattern of field loss was consistent and all eyes had permanent, non-progressive, absolute, dense, peripheral inferotemporal scotomata. The scotoma reached the blind spot in only one case. In all cases the scotoma extended above the horizontal in the far periphery. This consistent pattern and location, which has also been reported by others,3 4 9 17 would suggest a common site and aetiology in the pathogenesis of these lesions.
Aetiological mechanisms proposed in the development of visual field loss include glaucomatous damage secondary to postoperative raised intraocular pressure and mechanical compression from an expanding gas bubble. These mechanisms have been examined by us and by others2 3 18 and have not been shown to play a major part in the development of this pattern of visual field loss. Previous studies have also demonstrated normal photoreceptor function in the retina corresponding to the area of visual field loss2 17suggesting nerve fibre layer injury and it has been proposed that these visual field defects must arise from damage to the optic disc or peripapillary nerve fibre layer. In our series of eyes the consistent pattern of peripheral field loss with preservation of the blind spot would also suggest that the optic disc rim rather than the central portion is predominantly affected. The significant reduction in the incidence of visual field defects in eyes in which the posterior hyaloid was not stripped would seem to indicate that vitreopapillary traction, during forced separation of the posterior hyaloid, is responsible for the formation of these visual field defects.
The field defects in our series were always temporal in location which indicates nasal involvement of the optic disc or peripapillary nerve fibre layer. Previous histological studies have also shown the posterior cortical vitreous is most adherent at the superonasal aspect of the optic disc19 and that this is the last area to separate during spontaneous posterior vitreous detachment.20 Furthermore, histopathological studies have shown that cortical vitreal membranes extend through gaps in the internal limiting membrane of the retina and optic disc and become entwined between glial cell processes and these epipapillary membranes are found in a nasal in location in 90% of cases studied.21 22 This arrangement results in a strong adhesion between the cortical vitreous fibres and the adjacent nerve fibre layer. Forced separation of the posterior cortical vitreous from the optic nerve head could thus conceivably lead to damage to the superficial nerve fibre layer via traction on these processes.
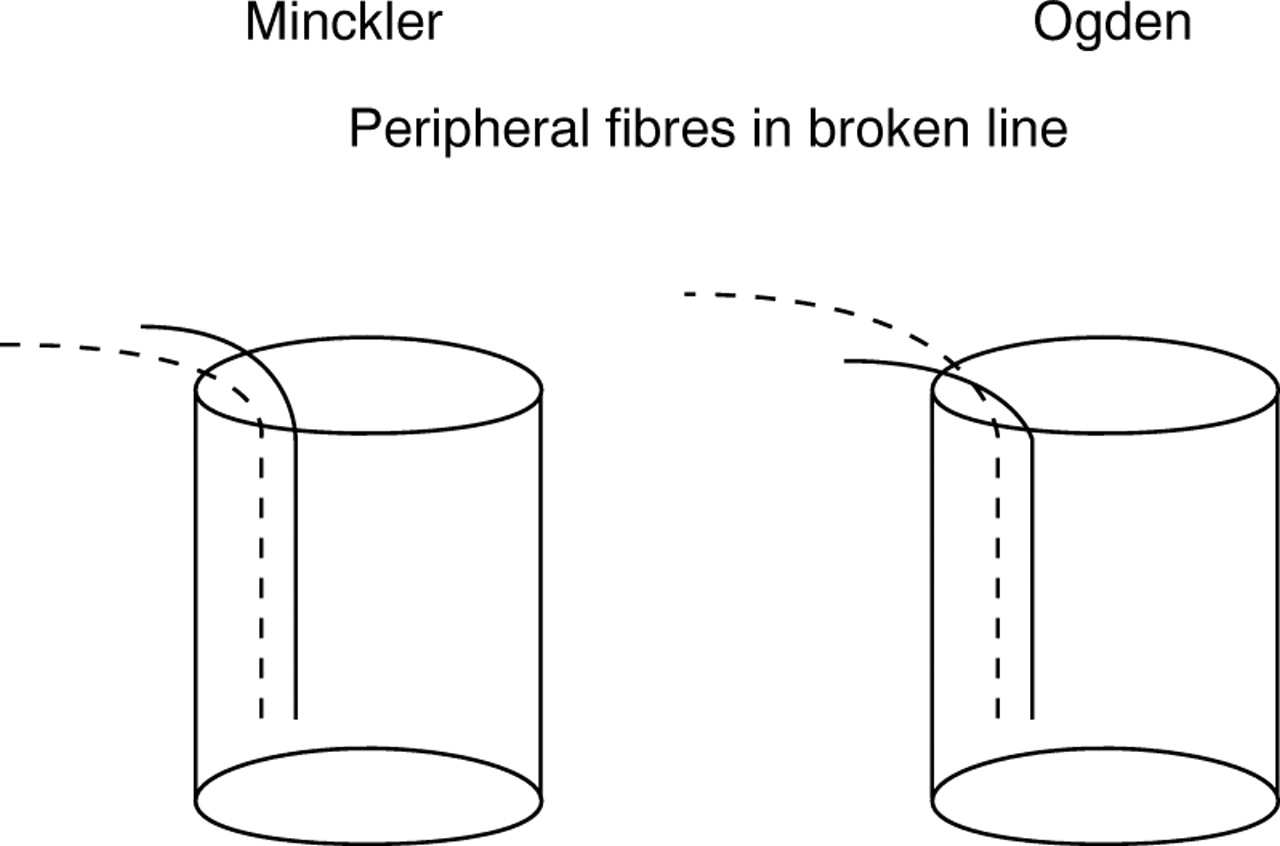
However, the topographical orientation of the peripapillary nerve fibre layer is uncertain, as illustrated in Figure 4. Ogden23proposes that the nerve fibre layer subserving the peripheral retina lies vitreal or superficial to the fibres originating from the central retina as they enter the optic nerve head. If this is the case, shearing forces during posterior hyaloid separation may cause direct damage to the nasal superficial nerve fibre layer and would result in the pattern of visual field loss found in our series of patients. Minckler,24 however, suggests the opposite, that the peripheral nerve fibre layer lies scleral or deeper within the peripapillary optic nerve head and that the superficial nerve fibres subserve the central retina. This arrangement would be anticipated to cause central field loss adjacent to the optic disc and sparing the periphery. Postoperatively, nerve fibre layer defects or sectorial disc pallor corresponding to these dense peripheral scotomas would be expected. In our series of eyes with visual field defects this was not the case.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
A schematic diagram illustrating the proposed theories of vertical topographical organisation of the peripheral retinal nerve fibres at the optic nerve head.
Apart from direct damage to the nerve fibre layer, visual field loss may result from disruption of the microcirculation at the optic nerve head occurring during forced mechanical separation of the posterior hyaloid. The blood supply to the prelaminar and laminar anterior optic nerve in humans is derived from the posterior ciliary arteries and pial blood vessels. There are also minor contributions from the central retinal artery to this area and to the superficial vessels of the nerve fibre layer. Studies by Hayreh25 indicate the existence of vertically orientated watershed zones lying between the end arterial supply of the medial and lateral posterior ciliary arteries. These studies have demonstrated that in 26% of patients a watershed zone involves the medial aspect of the optic nerve head.
Based on anatomical studies in primates26 it has also been proposed that, owing to the centripetal blood flow of the optic nerve head, and the fact that the peripapillary region is likely to be a low pressure system compared with the remaining choroid,27 the area between the optic nerve and the peripapillary choroid may act as another watershed zone. This hypothesis is in keeping with a study on the distribution of optic nerve head Po2 which found that tissue Po 2 values were lowest deep within the margin of the optic nerve head, rather than superficially in the central nerve fibre layer.28 The presence of a “peripapillary” watershed zone combined with a “vertical” watershed zone would make this area a likely potential site for ischaemic insult. Furthermore, it is agreed that in the deeper prelaminar optic nerve it is a consistent finding that nerve fibres from peripheral retinal elements are located peripherally at this site. A localised vascular event involving ganglion cell axons at the optic nerve rim would thus result in a corresponding peripheral visual field loss. Such a lesion occurring deeper in the peripapillary retina at the level of the laminar or deep prelaminar nerve fibre layer may not be visible on postoperative clinical examination and would account for the lack of visible superficial nerve fibre layer dropout despite such profound field loss.
During surgical peeling of the posterior hyaloid considerable traction may be exerted on the peripapillary nasal retina with a marked ripple effect visible on the nasal peripapillary retina and even elevation of the retina occurring in some cases. In our study the surgical peeling of the cortical vitreous from the underlying nerve fibre layer was more often performed in a nasal to temporal direction. Lateral mobilisation of the optic nerve head in relation to its surrounding vascular supply may take place during this separation of the posterior hyaloid. A tangential force, temporally directed, would predominantly disrupt the vascular supply on the medial aspect of the optic nerve head. Combining this surgical technique with cases where the watershed zone was located medially would render the optic nerve head rim susceptible to localised infarction. Subtle defects in “juxtapapillary” perfusion resulting in visual field defects would not necessarily be visible clinically and signs of choroidal ischaemia would not be seen as the surrounding peripapillary choroidal circulation would still be intact.
Other mechanisms have been postulated to account for this pattern of field loss in these eyes. A dehydration mechanism of retinal injury from a potential drying effect during air infusion has also been a proposed aetiology in the development of visual field loss.29 30 In our study the remaining peripheral cortical vitreous in the group II eyes would have a protective effect from this drying action on the underlying retina, although it is our observation that a film of fluid always remains on the retinal surface throughout the procedure. Whether a stream of air traversing the eye is capable of breaking the surface tension to produce a localised area of retinal desiccation is uncertain, given the high intraocular humidity with a pool of fluid remaining at the posterior pole and the effects of turbulence on the airstream.
In conclusion, we present an alternative approach to macular hole repair which involves preservation of the cortical vitreous at the optic nerve head. There is a significant reduction in the incidence of visual field defects associated with the use of this technique when compared with a control group. This method lends support to the theory that manipulation of the posterior hyaloid at the optic disc plays an important part in the pathogenesis of visual field loss. There was no significant increase in the incidence of the other complications of macular hole surgery associated with this technique. In addition, this study indicates that posterior hyaloid separation at the optic disc is not essential in attaining comparable anatomical and visual success from macular hole surgery.