Article Text

Abstract
AIM To examine the outcome of care for patients with glaucoma followed up by the hospital eye service compared with those followed up by community optometrists.
METHODS A randomised study with patients allocated to follow up by the hospital eye service or community optometrists was carried out in the former county of Avon in south west England. 403 patients with established or suspected primary open angle glaucoma attending Bristol Eye Hospital and meeting defined inclusion and exclusion criteria were studied. The mean number of missed points on visual field testing in the better eye (using a “better/worse” eye analysis) in each group were measured. The visual field was measured using the Henson semiautomated central field analyser (CFA 3000). Measurements were made by the research team on all patients at baseline before randomisation and again 2 years after randomisation. The mean number of missed points on visual field testing in the worse eye, mean intraocular pressure (mm Hg), and cup disc ratio using a “better/worse” eye analysis in each group at 2 years were also measured. Measurements were made by the research team on all patients at baseline before randomisation and again 2 years after randomisation. An analysis of covariance comparing method of follow up taking into account baseline measurements of outcome variables was carried out. Additional control was considered for age, sex, diagnostic group (glaucoma suspect/established primary open angle glaucoma), and treatment (any/none).
RESULTS From examination of patient notes, 2780 patients with established or suspected glaucoma were identified. Of these, 752 (27.1%) fulfilled the entry criteria. For hospital and community follow up group respectively, mean number of missed points on visual field testing at 2 year follow up for better eye was 7.9 points and 6.8 points; for the worse eye 20.2 points and 18.4 points. Similarly, intraocular pressure was 19.3 mm Hg and 19.3 mm Hg (better eye), and 19.1 mm Hg and 19.0 mm Hg (worse eye); cup disc ratio at 2 year follow up was 0.72 and 0.72 (better eye), and 0.74 and 0.74 for hospital and community follow up group respectively. No significant differences in any of the key visual variables were found between the two groups before or after adjusting for baseline values and age, sex, treatment, and type of glaucoma.
CONCLUSIONS It is feasible to set and run shared care schemes for a proportion of patients with suspected and established glaucoma using community optometrists. After 2 years (a relatively short time in the life of a patient with glaucoma), there were no marked or statistically significant differences in outcome between patients followed up in the hospital eye service or by community optometrists. Decisions to implement such schemes need to be based on careful consideration of the costs of such schemes and local circumstances, including geographical access and the current organisation of glaucoma care within the hospital eye service.
- glaucoma
- hospital eye service
- community based optometrists
- Bristol
Statistics from Altmetric.com
Primary open angle glaucoma (POAG) is a slowly progressive chronic eye condition which, once diagnosed, requires lifelong observation and management. Even with careful monitoring and good control of intraocular pressure (IOP) up to 25% of patients continue to lose visual field.1 The prevalence of glaucoma is 0.4% to 3.3% in those over 40 years old but rises with age to 5% in people aged 80 and over2 3 resulting in a considerable workload for ophthalmic departments. Almost a quarter of outpatients attending Bristol Eye Hospital do so for follow up of glaucoma (Professor John Colley, personal communication), and this pattern is likely to be similar elsewhere.4
The Bristol shared care glaucoma study was set up to examine whether community based optometrists might have a role in the management of patients with primary open angle glaucoma. A randomised controlled study design was used with patients allocated either to follow up by community optometrists or to usual care by the hospital eye service. Data on the reliability and validity of measurements made by optometrists, patient satisfaction, and the costs of the two approaches to surveillance have already been reported.5-7 This paper reports on patient outcomes at the 2 year follow up.
Methods
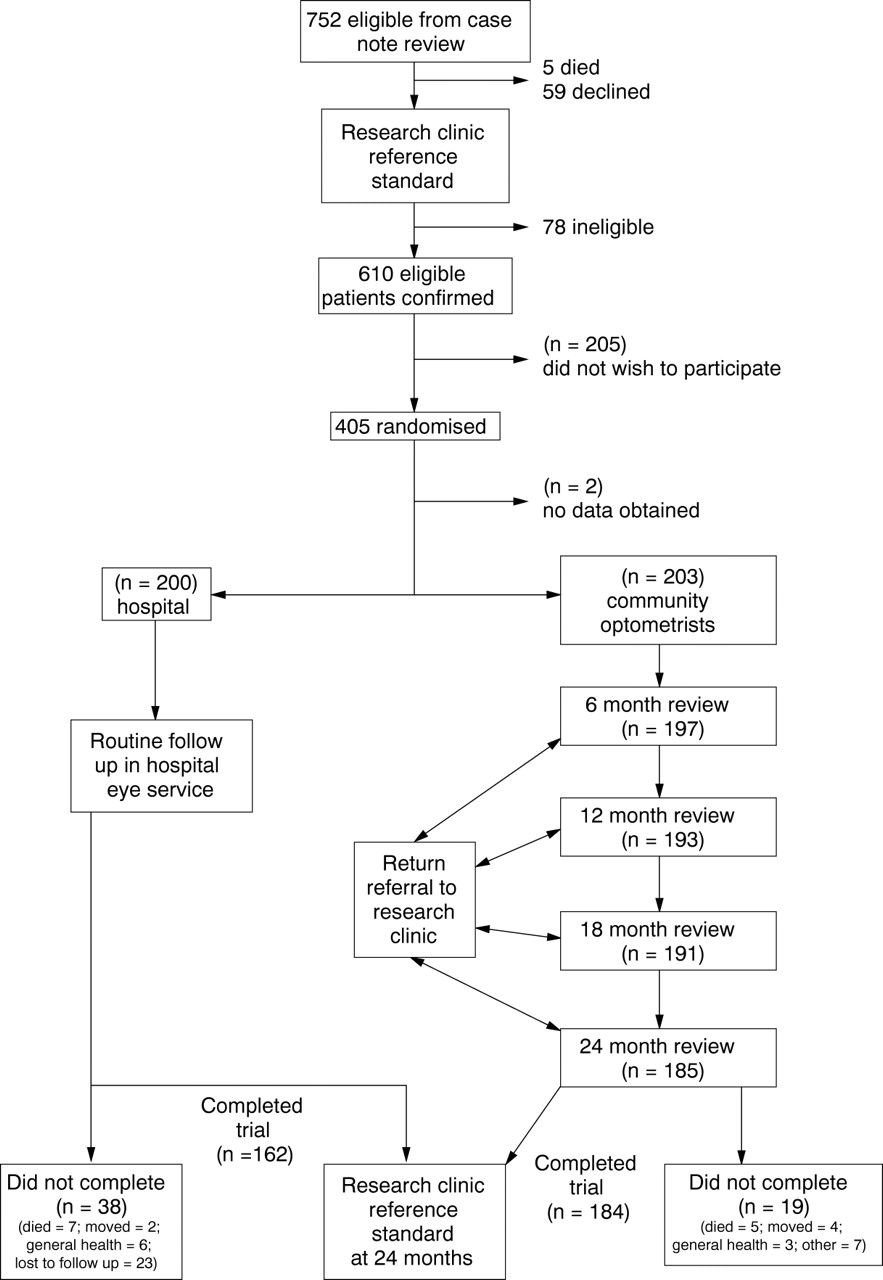
Full details of the methods used to set up the study have previously been described.8 The trial profile is shown in Figure 1. All optometrists in Avon (approximately 100) were sent a questionnaire to determine whether they would be interested in participating in the study and also if they had appropriate instrumentation; 45 expressed an interest of whom 13 had an appropriate visual field analyser (the Henson CFA 3000) for the study. Twelve were recruited so as to achieve a geographical spread of participating practices. Permission was sought from non-participating optometrists for their patients to be seen by study optometrists if allocated to that arm of the study. Study optometrists received training consisting of 15 hours of lectures and 10 hours of practical “hands on” examination experience on volunteer glaucoma patients at Bristol Eye Hospital. Optometrists were remunerated at a rate agreed as reasonable for the purpose of conducting the study and confirmed that they were insured professionally to cover the measurements and referrals required by the study. The United Bristol Healthcare Trust local research ethics committee gave approval for the study.
{kind=link}
Trial profile.
PATIENT ELIGIBILITY AND RANDOMISATION
Eligible patients were identified by reviewing case notes of all attenders aged 50 years and over attending specialist glaucoma clinics at the Bristol Eye Hospital. Patients were included if they were classified as glaucoma suspects or had primary open angle glaucoma, were able to cooperate, and had a Snellen visual acuity of >6/18 or better in both eyes. A visual acuity of 6/18 or better ensured clear ocular media sufficient to enable reliable measurement of optic disc variables. Glaucoma suspects were defined as having intraocular pressure of above 24 mm Hg on at least two occasions, and/or suspicious optic disc appearances, but no demonstrable visual field defect in either eye on threshold related suprathreshold visual field assessment on at least two occasions. Patients were considered “stable” if their consultant felt that intraocular control was satisfactory on treatment and that visual field deterioration had not been identified on at least two repeatable threshold related suprathreshold field tests over the past year. Patients were excluded if they had unstable glaucoma, normal tension or other complex glaucomas, extensive visual field loss (>66/132 points with Henson suprathreshold strategy), or serious coexisting pathology. Unstable POAG patients were defined according to clinical judgment of the supervising ophthalmologist, as was poor IOP control necessitating a change in treatment or poor compliance in taking medical treatment.
Those who appeared eligible following case note review were invited for a detailed assessment by the research team (described hereafter as the research clinic reference standard). The research team consisted of an ophthalmological registrar (IS), a registered optometrist (PS), and an ophthalmologically trained nurse with special skills in visual field testing. If eligibility was confirmed, informed consent was sought and patients were randomised using sealed opaque envelopes containing the allocation to either the hospital eye service or to community based optometrists. Allocation codes were generated using block random numbers.
MEASUREMENTS OF VISUAL VARIABLES
The research clinic reference standard examination was conducted on all patients at baseline before randomisation and at 2 years after randomisation. This consisted of the following: a Humphrey field analyser 24-2 central visual field examination; 132 point Henson CFA3000 threshold related suprathreshold visual field examination (two tests for baseline examination); IOP measured by Goldmann applanation tonometry (mean of three consecutive tests); Snellen and logMAR visual acuity; full binocular indirect ophthalmoscopic optic disc examination (with pupil dilatation) and optic disc stereophotography after pupil dilatation. For visual field testing with the Henson CFA 3000, points were defined as defective if they were unseen at any suprathreshold increment (5, 8, or 12 dB). To avoid false positive errors in the semiautomated strategy, points unseen on first presentation were re-presented with a verbal cue to the patient to maintain central fixation and were only marked as unseen if missed on both presentations. For IOP, the Goldmann tonometer xprobe was reset to 10 for the initial measurement, and the scale was not read until the end point was reached. The end point selected for each measurement was inner edge opposition of the tear film fluorescein rings at the maxima of the IOP cycle (systolic).
The same examination was undertaken at 2 years post-randomisation by the same team using an identical standardised assessment protocol, the only difference being that a single suprathreshold field was done on this occasion. The researchers conducting the 2 year examination were blind to the randomisation of the group of patients, and previous measurements, although it is possible that they could have been aware of which group some patients were in.
FOLLOW UP
Patients randomised to the hospital eye service were followed up according to usual practice; those randomised to care by community based optometrists were seen at 6 monthly intervals. A clear protocol indicated when patients should be referred back to the hospital eye service. Details of the process have been described previously.8 Data were entered and stored on a database by the research team. Data collection was on a similar form for patients in the hospital eye service arm but data were obtained by the research team from the medical notes.
OTHER INFORMATION
Self reported data on medication and other treatment for glaucoma and co-existing disease were collected at baseline and at 2 year follow up. During the course of the study data were collected about patient satisfaction and costs; details have already been reported.5 6
SAMPLE SIZE
Careful consideration was given to attempting to perform a sample size calculation based upon expected field loss in both groups. However, owing to a paucity of long term data on the rate of visual field loss on a cohort of patients using the Henson CFA 3000 over a 2 year period, this was not feasible.
As previously reported,5 a sample size calculation was therefore performed using patient satisfaction as the key outcome. Baseline data suggested that satisfaction among hospital patients was of the order of 90% satisfied and 50% very satisfied. A total of 200 patients in each arm of the study was considered adequate on follow up to detect a difference of the order of 10–15% in the proportion of patients who expressed varying degrees of satisfaction in the two groups. Specifically, with a 5% two sided significance level, this study had 80% power to detect a difference of 90% satisfied versus 80% satisfied, and 85% power to detect a difference of 50% versus 35% very satisfied. Generally speaking, the sensitivity of the study to detect differences in terms of continuous measurements, such as visual field loss, would be expected to be considerably greater than this. For instance, a sample size of 200 in each group provides 85–90% power to detect differences of just under one third of a standard deviation (again using a 5% significance level).
STATISTICAL ANALYSIS
Data were entered into an Access 2.0 database and then exported for analysis in stata (Statistics Data Analysis, Stata Corporation, TX, USA). The analysis used baseline and 2 year follow up measures taken from the research clinic reference standard examinations. For analysis of the visual field the number of points missed during examination with the Henson CFA 3000 was used. (Where more than one measurement of fields or IOP had been made mean values were used.) This measure provides a summary of visual field loss, although it is recognised that it gives no differential weighting for missed points. However, given that a randomised study design is used, there is no reason to suppose that the spatial patterns of field loss would be different in each group. For each patient a “better” eye and a “worse” eye was identified using the visual field measurements at follow up. If the number of missed points on visual field testing was the same in both eyes at follow up, then the worse eye at baseline was taken to be the worse eye. If both baseline fields were identical (seven patients) a pragmatic decision was taken to record the right eye as the better eye. Visual field variables for the better and worse eyes were then identified for each patient—for example, intraocular pressure in better eye at baseline, cup disc ratio in worse eye at follow up, and so forth. The outcome measure of prime importance to patients is visual function, and it was considered that this most closely relates to function of the better eye. Thus, field loss in the better eye was considered to be the primary outcome measure, and the others secondary outcome measures.
An analysis of covariance was performed for each of the outcome variables comparing the two follow up groups adjusting for the corresponding baseline measurements. Additionally, control was considered for age, sex, time from recruitment to follow up, treatment at baseline, treatment at any time (any/none), and diagnosis (glaucoma suspect/established POAG).
Together with the large sample sizes, descriptive statistics indicated that the assumptions for these analyses were reasonable. Throughout the analysis statistical significance was taken at the 5% level and confidence intervals obtained for between group analyses.
Results
RECRUITMENT AND BASELINE COMPARABILITY
Of the 2780 patient notes examined, 2028 patients were not considered further as entry criteria were not met. The major reasons why entry criteria were not met were extensive visual field loss (912), newly diagnosed glaucoma (585), diagnosis other than POAG (357), and poor visual acuity (469). Of the 752 potentially eligible patients identified, five had died and 59 declined to attend the initial clinic assessment. Of those attending the assessment 78 were found to be ineligible on re-examination. Thus, 610 patients were confirmed as eligible. A third (205) of patients were unwilling to participate in the study, mainly due to problems with health (58), general concerns with extra visits (31), and transport, employment, or other time commitments. Two patients were recruited but no baseline data were recorded so they are not considered further. By October 1994, 403 patients had been recruited to the study of whom 200 were randomly allocated to follow up by the hospital eye service and 203 by community optometrists (see Fig 1).
The baseline characteristics of patients in both groups are shown in Table 1. Although broadly comparable, there were slightly more women and patients with suspected glaucoma in the community group. Mean age was similar in each group, although detailed scrutiny revealed some differences in the distribution, with relatively fewer in the age groups 65–74 and 75+ years in the community arm (Table2).
Baseline characteristics of patients in study
Numbers (%) of patients in each age group and numbers (%) of glaucoma suspects in each age group at baseline
As expected the mean field loss at baseline varied according to whether patients were glaucoma suspects or established cases of glaucoma. In the glaucoma suspects the mean (SD) number of points missed was 2.8 (2.10) in the better eye and 3.7 (3.7) in the worse eye. For established glaucoma it was 9.4 (10.8) for the better eye and 19.9 (14.5) for the worse eye. Only one patient had lost no points on field testing before randomisation.
Follow up information at 2 years post-randomisation was obtained for 346 patients (86%), including 162 (81%) hospital and 184 (91%) community patients (see Fig 1). For those attending the 2 year follow up examination, data on IOP were complete for all patients; there was one missing cup disc ratio measurement and three missing field tests.
FOLLOW UP RECEIVED IN EACH GROUP
As defined in the protocol, patients in the community follow up were seen at 6 monthly intervals. The trial profile (Fig 1) shows that 200, 197, 193, 191, and 185 patients attended at these time intervals respectively. Some patients missed one or more of their appointments but remained in the study.
Of the 200 patients in the hospital follow up arm, 166 attended the hospital eye service for a follow up visit before the 2 year follow up examination. The time to first follow up appointment varied from 3 months to over 24 months (mean 10.7 (SD 5.4) months). The median number of visits within the 2 year time period was 2.8 (range 0–8). A small number of patients had multiple visits as a result of follow up appointments after a surgical procedure.
OUTCOME AT 2 YEARS
Descriptive statistics of visual measurements for better and worse eye at the 2 year follow up and for changes from baseline are shown in Table 3. As anticipated, both groups show a small increase in the mean number of missed points on visual field testing and a slight increase in cup disc ratio over the 2 year period. Both groups also show a small decline in IOP, which may be a treatment effect. As anticipated the deterioration in visual fields was more pronounced in those with established glaucoma with the mean (SD) number of points lost on visual field testing of 3.2 (3.3) for better eye and 8.8 (10.7) for worse eye for glaucoma suspects, and 10.7 (14.1) for better eye and 28.1 (22.4) for worse eye for established glaucoma cases.
Descriptive data: visual variables at 2 year follow up and paired differences from baseline by group using better eye/worse eye analysis (mean (SD))
The results of the analysis of covariance for each of the outcome variables comparing the two follow up groups are shown in Table 4. No significant differences were shown between the two groups using this analysis. Adjusting for the corresponding baseline measurements, age, sex, diagnosis, and treatment had no appreciable effects on these results and so are not presented here. As there were no major differences between the two groups in time to follow up (mean 813 days, median 834, hospital; mean 804, median 814, community) and treatment at baseline (Table 1) these variables were not included in the analysis of covariance.
Results of the analysis of covariance: outcomes at 2 years by group using a best eye/worst eye analysis (n=346)
REFERRAL RATES AND INTERVENTION RATES
The number of patients referred back for assessment by the hospital at each community visit was 38 at 6 months, 45 at 12 months, 35 at 18 months, and 49 at 24 months. A number of patients were referred back to the hospital eye service on more than one occasion, with two (1.0%) being referred back four times, 10 (5%) three times, 30 (15%) twice, 69 (34%) once, and the remaining 92 (45%) not at all during the 2 year period. Considering all referrals together, a quarter were in patients with suspected glaucoma and the remainder in those with established disease. The outcome of the referrals is shown in Table 5. Changes in visual field were the most common reason for referral. The proportion of cases where the changes prompting referral were confirmed on re-examination by the research team and changes in management instigated in conjunction with the patient's consultant was very variable. In all but two cases following referral the patient was referred back for continuing care by the optometrists.
Number, reason, and outcome of referrals to hospital from community optometrists by follow up visit
By the end of the 2 year follow up 155 (78%) and 149 (73%) better eyes and 162 (81%) and 157 (77%) worse eyes in the hospital and community arm respectively had received treatment for glaucoma, either at baseline or by the 2 year follow up.
In the hospital and community group respectively, the number of patients who reported having received argon laser treatment by the 2 year follow up in the better eye was 12 (6%) and 14 (7%) and in the worse eye 13 (6.5%) and 21 (10.3%); for trabeculectomy the proportions were 15 (7%) and 18 (9%) for the better eye and 27 (14%) and 37 (18%) for the worse eye respectively.
Discussion
The increasing numbers of elderly patients with chronic eye disease (of which primary open angle glaucoma is a major one) have led to problems of overburdened ophthalmic outpatients in the UK. A report to the General Optical Council from the Optical Services Audit Committee9 in 1990 recommended ways of increasing the contribution of optometrists to the management of chronic eye diseases, and specifically that the clinical expertise of optometrists could be used to relieve the burden of overloaded outpatient departments. Against this background a number of shared care schemes for patients with glaucoma have been or are in the process of being set up, based upon an (as yet unproved) assumption that this will result in more cost effective patient care10-13 although caution has been advised.14 Not all have included specific training, standardised measurements, or agreed referral protocols, which the Royal College of Ophthalmologists in a joint statement with the College of Optometrists and the Royal College of General Practitioners has strongly recommended for all those considering setting up such schemes,15 all of which were a feature of this study. Minimal research about the effectiveness of these schemes has been undertaken.
The Bristol shared care glaucoma study was set up as a rigorous objective evaluation of a shared care scheme whereby community optometrists undertook surveillance of selected patients with glaucoma. A relatively high level of input of training was provided. Strict inclusion criteria, standardisation of measurements, and clear protocols for referral and return back to the hospital eye service were agreed at the outset. Within this context the study has demonstrated that patients followed up by community optometrists have comparable outcomes to those followed up by the hospital eye service, although it is recognised that 2 years is a relatively short period of follow up for this condition.
Previously reported data from this study have demonstrated that optometrists are able to make measurements of the key visual variables in patients with established or suspected glaucoma of comparable quality to those currently made within the hospital eye service.5 7 Patients were significantly more satisfied with certain aspects of care in the community compared with their experience in the hospital eye service, although this was predominantly due to improved ratings of issues related to travelling time and timeliness of appointments, rather than perceptions about the quality of care.5 The economic data have previously been reported in detail,6 but depending on the different methods used the annual cost per patient for follow up by community optometrists was £68.98–£108.98 compared with £14.50–£59.95 in the hospital eye service. (The costs for follow up by community optometrists included the costs of patients referral back to the hospital, with cost per hospital visit for returning patients assumed to be identical to the full cost of each hospital visit, and the referral rate used to calculate costs being the proportion of patients who were referred following the first 6 monthly visits.)
If optometrists are able to make measurements of comparable quality to the hospital eye service and outcomes are no different, should shared care for glaucoma now be implemented? There are a number of issues to consider carefully before making a recommendation along these lines. Firstly, this scheme used optometrists who were volunteers and who had also undertaken additional training, both factors which may improve their performance, and may limit the generalisability of the findings of this study. Secondly, it is unlikely that providing surveillance through community based optometrists will generate appreciable savings. However, depending on local circumstances, providing follow up in this way might provide a higher quality service for patients living at some distance from a hospital eye service, particularly perhaps in rural areas or where there are difficulties with public transport. It might also free up time within the hospital eye service, that could perhaps be used to deal with other work more speedily—for example, new referrals of glaucoma. The potential for doing this will be limited; although the inclusion and exclusion criteria used in this study were relatively strict, only 25% of the total patients with glaucoma attending the hospital eye service were eligible to participate; this still amounted to over 600 patients. Of those eligible, only 60% were willing to participate, but this might be higher outside the study, which required quite a number of additional visits. The inclusion criteria used in the study were in our view appropriately cautious. However, modest changes in the inclusion criteria could allow a much higher proportion of patients to be included in a shared care scheme. There is no a priori reason to suppose that the disease process is intrinsically different in patients excluded from the study. The measurements that are required to assess disease progression remain the same regardless of state of disease. Given that optometrists are seeing patients at predetermined intervals, undertaking a standardised assessment, and referring all those who demonstrate appreciable change according to a defined protocol back to the hospital eye service for review and change in management if required, there seems no particular reason to suppose that these results should not be broadly applicable to a wider patient group. However, it is possible that the rate of referrals to hospital might be higher in a different group. Increasing numbers of community optometrists now have access to field testing equipment and tonometers within their practices; a recent survey found that 42% of optometrists now have the Henson CFA 3000, most of which had been acquired in the past few years.16 These changes mean that a higher proportion of optometrists now routinely have suitable equipment to participate in shared care schemes than was the case when this study was set up.
We were unable to detect any significant change between the two groups over a 2 year period. As indicated earlier, it was not possible to conduct a sample size calculation on expected visual field loss owing to a paucity of long term data on the rate of visual field loss on a cohort of patients using the Henson CFA 3000. This study will provide robust data for future studies upon which to base such calculations. However, in considering the power of the study to detect significant change, generally a sample size of 200 in each group provides 85–90% power to detect differences of just under one third of a standard deviation at 5% significance level. Table 3 shows that the standard deviation for points lost for better eye and worse eye was 10.8 and 19.9 respectively, suggesting that the study would have had power to detect an approximate order of difference of three points in the better eye, and six points in the worse eye. Unpublished data on the test retest reliability of the Henson CFA 3000 (Dr David Henson, personal communication) using normal patients indicated that 2 SDs of the mean difference in readings was four points; hence, differences above this are likely to be due to real change. There is no clear consensus as to what is a clinically significant change in visual field. However, as part of the background preparatory work in for the study we undertook a survey of ophthalmologists seeking views as to what change in visual field (and other variables) they would consider should prompt a change in management. Of the 49 respondents, 73% considered that a new cluster of four points, and 23% that four new scattered points using the Henson CFA3000 should be considered significant in starting or changing management.4 Thus, it seems reasonable to conclude that change of the order of four points of magnitude can be considered to be of likely clinical significance. Given these two factors, it is reasonable to believe the study would have had sufficient power to detect clinically significant change.
It is very difficult to assess “safety” in a shared care scheme. The relatively high proportion of patients referred back at each 6 month interval suggests that optometrists were being relatively cautious, and a proportion of false positives were referred back on each occasion. However, the issue of safety would require an assessment of the number of false negatives in both the hospital and community arm. We have not attempted to undertake this analysis from the data. The ultimate issue is whether the outcome is different after 2 years in each group, and we found no evidence to suggest that it was. This is a relatively short duration of follow up for patients with glaucoma, and longer follow up would of course be welcome.
The specific financial issues relating to payment of optometrists for provision of these services would also need to be agreed. Informal feedback from the participating optometrists was that they had enjoyed participating in the study, and that they would be prepared to continue participating in such a scheme if remuneration could be agreed at a similar level. They commented that while they had not undertaken sight testing during the glaucoma surveillance visits they had experienced some indirect benefit—for example, relatives purchasing spectacles. While annual cost per patient for follow up by community optometrists was £68.98–£108.98 compared with £14.50–£59.95 in the hospital eye service, sensitivity analysis demonstrated that if the follow up interval by community optometrists was allowed to be similar to that of the hospital services, the full costs per annual patient visit for community optometric services would fall to £46.31 and the lowest marginal cost could be £41.38.6 The economic analysis examined the real costs associated with care in each setting. Given the way in which optometrists are currently remunerated, the price, as opposed to the cost of the service would of course be dependent on the fee which was agreed for follow up of patients with glaucoma.
Other approaches to service development for this group of patients have been recommended.17 One approach to is to structure the review process and critically examine the skill mix required within the hospital eye service so that a multidisciplinary approach is taken with optometrists and nurses undertaking appropriate tests.14Given the high degree of interobserver variation inherent in the measurements required to assess disease progression in glaucoma,7 consideration should be given to maximising continuity of care within the hospital eye service. Other issues that could be addressed include identification of which (if any) patients with suspected glaucoma with minimal field loss require follow up by the hospital eye service. Preliminary work undertaken as part of the background preparation for the study showed that there is currently great variation in the frequency with which patients are followed up and the tests that are undertaken at each visit.4Standardising the frequency with which individuals are seen, and the tests undertaken on each occasion has the potential to streamline clinics. Finally, given that the amount of change believed to reflect clinical deterioration is not dissimilar to the random variation in these measurements, consideration should be given to the need for an internal quality assurance programme for measurement of key visual variables which determine treatment changes.
Perhaps most importantly, the demonstration of deterioration in both visual field and cup disc ratio in this relatively stable group of patients with apparently well controlled IOP over a 2 year period emphasises the need to continue to develop reliable and sensitive methods for monitoring outcomes other than IOP in glaucoma, and the need to examine the efficacy of therapy in terms of outcome not intermediate risk factors.
In conclusion, this study has shown that it is possible to set and run shared care schemes for glaucoma using community optometrists. When appropriately trained optometrists are able to make measurements of comparable quality there does not appear to be any significant difference in patient outcomes over a 2 year period. However, shared care schemes are unlikely to be more cost effective than the hospital eye service care, and decisions to implement such schemes need to be based on careful consideration of local circumstances, including geographical access and the current organisation of glaucoma care within the hospital eye service.
References
Footnotes
-
↵Current address: Discoveries in Sight, Devers Eye Institute, Portland, Oregon, USA
-
Funding: The Bristol shared care glaucoma study was funded by the MRC (small project grant), the International Glaucoma Association, R&D Directorate NHS Executive South and West, and Avon Health Authority.
We thank Mrs Judy Furber for unstinting support with conducting field tests; all members of the Avon Chronic Eye Disease Group; the participation of the community optometrists without whose enthusiastic help and support the study would not have been possible; Mr John Foster for assistance with data collection; and Ms Joanna Coast for undertaking the economic analysis and providing invaluable support throughout the study.