Article Text

Abstract
AIM To report the clinical consequences of contamination of human donor corneas by herpes simplex virus (HSV) in organ culture.
METHODS Two patients without previous history of ocular HSV infection underwent penetrating keratoplasty (PK), one for keratoconus and the other for Fuchs' endothelial dystrophy. One patient suffered primary graft failure while the other developed a persistent epithelial defect, ultimately resulting in graft failure. Viral culture of swabs taken from both corneas during the early postoperative period was undertaken. The failed donor corneas were examined histopathologically by immunohistochemistry (IHC) for HSV-1 antigens, transmission electron microscopy (TEM), and by polymerase chain reaction (PCR) for HSV DNA. Both failed corneas were replaced within 6 weeks of the initial surgery. The records of the fellow donor corneas were also examined for evidence of infection.
RESULTS HSV was cultured from both corneas during the early postoperative period. Histology of both donor corneas demonstrated a thickened corneal stroma with widespread necrosis of keratocytes and loss of endothelial cells. IHC showed keratocytes positive with antibodies to HSV-1 antigens. TEM demonstrated HSV-like viral particles within degenerating keratocytes. PCR performed on the failed corneal grafts was positive for HSV-1 DNA, whereas PCR performed on the excised host corneal buttons was negative in both patients. Records of the fellow donor corneas showed that one cornea was successfully transplanted into another recipient after 18 days in organ culture, whilst the other was discarded because of extensive endothelial cell necrosis noted after 15 days in organ culture.
CONCLUSION HSV within a donor cornea may cause endothelial destruction in organ culture and both primary graft failure and ulcerative keratitis after transplantation. Endothelial necrosis of a donor cornea in culture also raises the possibility of HSV infection within the fellow cornea.
- graft failure
- human donor corneas
- herpes simplex virus
Statistics from Altmetric.com
The advent of eye bank storage has enabled a large number of corneal grafts to be performed on demand. It allows planning of elective procedures and screening of donor serum for evidence of previous exposure to human immunodeficiency virus (HIV) and hepatitis B and C.
The risk of bacterial or fungal contamination is minimised by cleansing of the donor tissue in povidone-iodine and subsequent culture at 34°C in media containing antibiotics and an antifungal agent. Before issue the corneal endothelium is assessed by light microscopy using trypan blue after exposure to 1.8% sucrose which stains healthy endothelial cell borders as well as non-viable cells. The endothelial cell density is measured using a graticule.1
Despite these measures transplanted tissue occasionally suffers primary graft failure (PGF), defined as a diffusely oedematous cornea on the first postoperative day which fails to clear at any time postoperatively in the absence of an identifiable cause of corneal graft failure.2 Rates of PGF are said to vary between 0–10%2 depending on a number of factors including cause of death,3 time in culture,2 eye bank retrieval and storage techniques,4 and surgeon related factors.5
HSV has been incriminated as a cause of profound endothelial necrosis in corneal organ culture6 and has been implicated in some cases of primary graft failure.7-9 Other reports have highlighted the occurrence of epithelial lesions due to HSV in corneal grafts where the recipients had no previous history of herpes infection.10-13 These infections are generally presumed to have been transmitted to the recipient via the donor material.
We report two further cases of culture proved HSV infection in newly transplanted recipients with no previous history of herpes simplex keratitis (HSK). In addition, the fellow donor cornea of one of the transplanted corneas was noted to have undergone endothelial destruction while in organ culture and was therefore considered unsuitable for transplantation.
Methods
CASE 1
An 81 year old woman with Fuchs' endothelial dystrophy and cataract underwent a penetrating keratoplasty (PK) combined with an extracapsular cataract extraction and posterior chamber lens implant. The surgery was performed uneventfully using 8 mm donor and 7.75 mm recipient trephines. The donor cornea had been obtained from a 70 year old man who had died from carcinomatosis. The death to culture time was 31 hours and the time in organ culture at 34°C was 18 days. The final endothelial assessment, performed 2 days before grafting, was 2900 cells/mm2. Organ culture medium screened for bacterial and fungal contamination after 7 days of culture and 1 day before issuing failed to reveal evidence of bacterial or fungal contamination. Serological screening for HIV antibody, hepatitis B surface antigen, and HCV antibodies was negative. The original host button was submitted for histopathology.
On the first postoperative day the graft was thickened and hazy. There was complete absence of epithelium over the graft. The patient's visual acuity was counting fingers only. Postoperative treatment consisted of topical prednisolone acetate (1%) four times a day, chloramphenicol (0.5%) four times a day, and cyclopentolate (1%) twice a day. The patient reattended 7 days later with increased pain and reduced vision. On examination the vision was hand movements only. The graft remained thickened, hazy, and de-epithelialised. There were numerous folds in Descemet's membrane with pigment deposits on the endothelium. A swab was taken from cornea from which HSV was cultured. Despite commencement on oral aciclovir (800 mg four times a day) and topical aciclovir (3% five times a day) in addition to her previous medication, the patient's condition did not improve. Four weeks after the first graft was performed the patient underwent a successful repeat graft which remains clear 11 months later. The patient continues to take systemic aciclovir (400 mg twice a day). The excised corneal button was submitted for histopathology, immunohistochemistry (IHC), transmission electron microscopy (TEM), and polymerase chain reaction (PCR) analysis for HSV DNA.
CASE 2
A 35 year old man underwent uncomplicated penetrating keratoplasty for keratoconus. He was fit and healthy except for atopic disease. There was no history of cold sores or any other eye infections. The donor was a 43 year old man who had died from a cardiac arrest. The death to culture time of the donor cornea was 24 hours and the time in organ culture was 22 days. The donor material was stored in the same conditions and subject to the same tests as described above. The original host button was submitted for histopathology.
On the first postoperative day, the corneal graft remained clear with an intact epithelium. One week later a central epithelial defect was noted on the donor cornea. Despite treatment with a bandage contact lens and topical antibiotics the epithelial defect persisted with eventual extension of the epithelial defect onto the host cornea. By then the whole graft was oedematous and cloudy. Two weeks after the initial graft was performed a viral swab was taken from the cornea from which HSV was cultured. The patient was treated with topical and systemic aciclovir. Complete healing of the epithelium was noted after 1 week. As the graft remained oedematous a regraft was performed 5 weeks after the initial surgery. The excised corneal button was submitted for histopathology, IHC, TEM, and PCR analysis for HSV DNA. There was no recurrence of HSV infection 12 months following the regraft although the patient has had several episodes of successfully treated graft rejections. The patient continues to take systemic aciclovir 400 mg twice a day.
VIRAL CULTURE METHODS
Swabs in virus transport medium were inoculated on to Hep2, Vero, and human embryo lung fibroblast cell cultures. These were examined on daily basis for evidence of a cytopathic effect.
POLYMERASE CHAIN REACTION METHODS
HSV PCR was a modification of the method of Cohenet al 14 using primers KS30 and KS31 and digoxygenin labelled probe sequence KS51 and PCR-ELISA detection (Boehringer Mannheim, Lewes, East Sussex; catalogue No 1 636 111). The guanidinium method was used to extract viral DNA as described by Casas et al.15
HISTOPATHOLOGY
Tissue for light microscopic assessment was fixed in 10% phosphate buffered formalin containing 0.1% cetylpyridininum chloride (CPC), following which it was processed into paraffin wax. Sections were cut at 6 μm and mounted on 3-aminopropyl-6-ethoxysilane (APES) coated glass slides. For routine histology, sections were stained with haematoxylin and eosin, and periodic acid Schiff (PAS). For IHC, sections were dewaxed, trypsinised, and preincubated in normal horse serum to block non-specific binding sites, and rabbit anti-HSV-1 antiserum (Dako, UK) was applied for 1 hour at a dilution of 1:400. Bound antibody was visualised by a standard avidin-biotin complex (ABC) revealing system (Techmate, Dako, UK) with 5,5′ diaminobenzidine (DAB) as chromogen. Sections of brain from a case of herpes simplex encephalitis provided the positive control, and sections which were stained with omission of the primary antibody, provided the negative controls.
Tissue for electron microscopy was fixed in 2.5% glutaraldehyde, following which it was dehydrated in graded alcohols and processed into Araldite resin. Areas of tissue containing keratocytes were identified using semithin (1 μm) sections stained with toluidine blue. Following this sections were cut at 90 nm, mounted on grids, and stained with 2% uranyl acetate and Reynold's lead citrate before examining on a Jeol 100CX electron microscope.
Results
VIRAL STUDIES
Herpes simplex virus was cultured from corneal swabs taken from both cases. HSV specific PCR performed on both recipients' corneal buttons was negative. However, PCR for HSV-1 was positive from the failed donor corneas in both cases.
HISTOPATHOLOGY
Case 1
The recipient's cornea was thickened and hazy without evidence of inflammation, scarring, or vascularisation. The epithelium was partially detached and Descemet's membrane was thickened and laminated with numerous guttate excrescences. There was a marked reduction in the endothelial cell count. The appearances were of endothelial insufficiency as seen in Fuchs' endothelial dystrophy. IHC and TEM were negative for HSV.
The failed graft was almost completely denuded of epithelium and endothelium, and the posterior surface was bowed due to oedema. Keratocytes were considerably reduced in number, those remaining appearing necrotic. Cells containing melanin pigment were present on the posterior surface of the cornea (Fig 1).
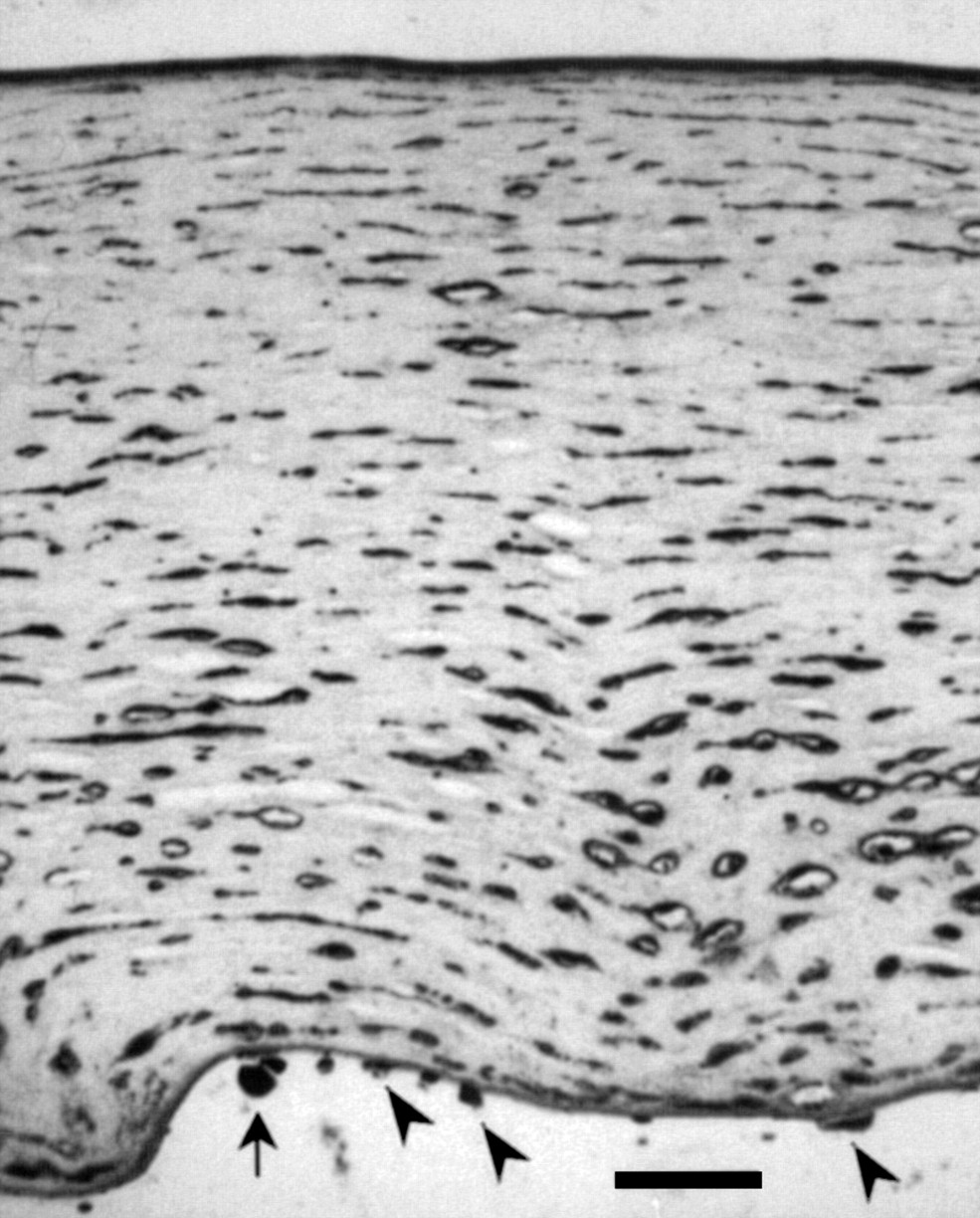
Case 1. The cornea is devoid of epithelium and the posterior surface is bowed as a result of oedema. Virtually all keratocytes are strongly positive for HSV-1, as are the remaining endothelial cells (arrowheads). Bowman's layer and Descemet's membrane are diffusely positive, possibly reflecting viral load in this tissue. A pigment-containing phagocyte (arrow) is present on the posterior surface of the cornea. (Immunohistochemistry, anti-HSV-1, DAB with haematoxylin counterstain. Scale bar = 100 μm).
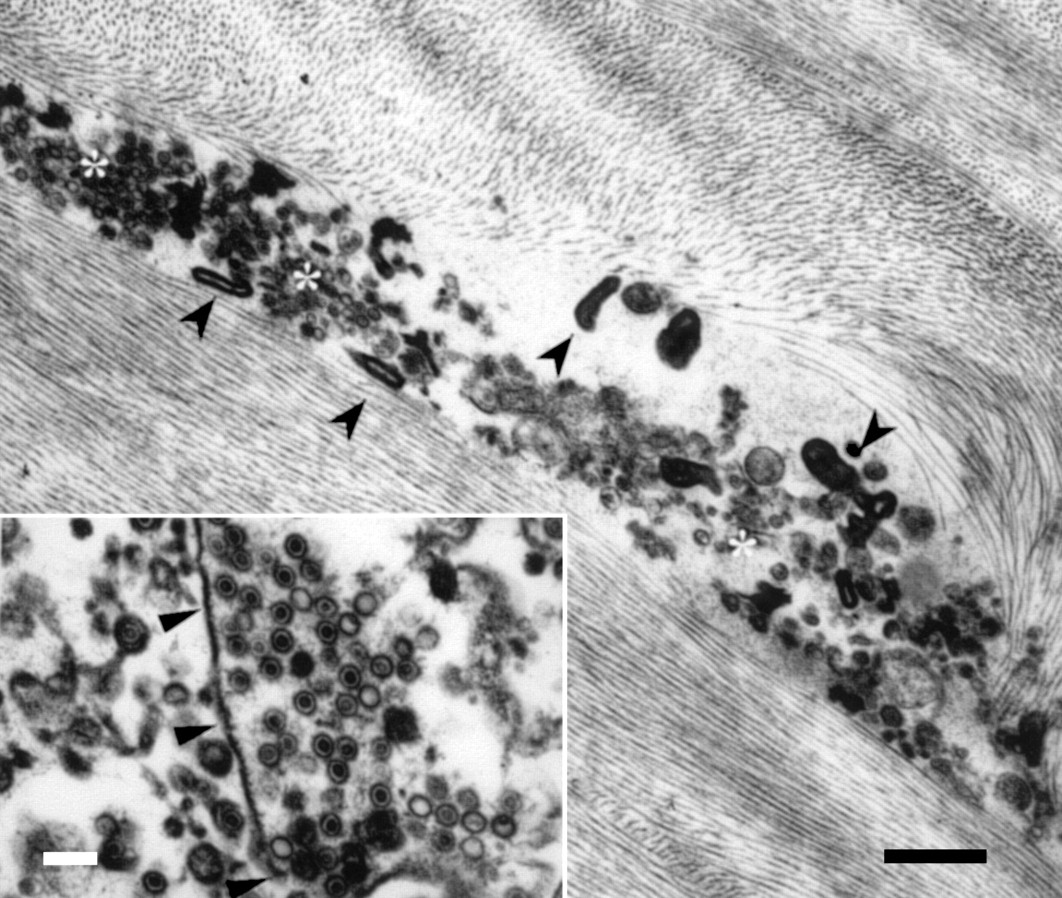
There was no inflammatory infiltrate, vascularisation, or scarring. IHC showed many HSV-1 positive keratocytes and the few remaining endothelial cells were HSV-1 positive. Electron microscopy revealed large numbers of herpesvirus particles within degenerating keratocytes (Fig 2).
{kind=link}
{kind=link}
Case 1. Electron micrograph showing a disintegrating keratocyte, with no plasmalemma or nuclear membrane remaining, and “myelin figures” (arrowheads) indicative of membrane breakdown. Groups of viral particles (asterisks) are present (scale bar = 1.8 μm). Inset: Another keratocyte in which the nuclear membrane is intact (arrowheads) and in which there are numerous herpes simplex viral particles, intact and empty, within the nuclear compartment and the cytoplasm (scale bar = 225 nm).
Case 2
The recipient corneal button showed features typical of uncomplicated keratoconus. There was no evidence of scarring, inflammation, or vascularisation. IHC and TEM were negative for HSV.
The failed graft showed epithelial oedema and diffuse stromal scarring. Many anterior keratocytes showed nuclear condensation and fragmentation characteristic of apoptosis and there was severe depletion in the number of endothelial cells. IHC showed HSV-1 positive keratocytes and TEM confirmed the presence of herpes viral particles within keratocytes as observed in the first patient.
FELLOW DONOR CORNEAS
The fellow cornea of the graft used for case 1 showed marked endothelial cell necrosis on endothelial assessment with less than the critical number of endothelial cells considered suitable for transplantation. Unfortunately, the cornea was discarded before any viral or histopathological studies were performed. The fellow cornea to the graft used for case 2 was transplanted uneventfully elsewhere into another individual with macular corneal dystrophy. This patient had a clear graft 2 months after surgery but was lost to follow up thereafter.
Discussion
We describe the occurrence of HSV infection in transplanted donor tissue. It has long been recognised that there is a potential, though small, risk of transmission of HIV, hepatitis B and C by corneal transplantation.16 While potential donors are screened by history and by serology for HIV, hepatitis B and C, HSV is a common pathogen in the cornea and seroepidemiology indicates that up to 95% of the population over 60 years of age may carry HSV specific antibodies.17
Neither of our patients had a previous history of ocular HSV infection. The first patient underwent classic primary graft failure. Possible causes of primary graft failure include poor surgical technique, poor donor material and poor eye banking technique, inadequate storage in organ culture, or infection of the donor material. However, the surgery was straightforward and routine. A qualitative and quantitative assessment of the donor endothelium indicated good quality and microbiology of the medium during culture and at issue was sterile. The coincidence of primary graft failure with a positive PCR, IHC, TEM and culture for HSV in the donor graft button but negative results of the same tests in the excised host cornea, strongly implicates HSV activation as the precipitating cause of graft failure. Endothelial cell necrosis was observed in the fellow donor cornea during organ culture, an observation previously reported in our centre as being associated with HSV.6 This suggests the possibility that HSV may have been present in the donor tissue and that viral replication could have occurred in organ culture causing endothelial necrosis in one cornea and widespread infection in the other cornea after transplantation. Unfortunately, this cannot be proved, as the fellow donor cornea was discarded before the presence of HSV could be established.
IHC, in situ hybridisation (ISH), PCR, and TEM have detected herpes simplex virus within donor corneas where endothelial necrosis had occurred in organ culture.6 7 The fellow donor cornea from one of these non-viable corneas was transplanted into a female who subsequently underwent graft failure. Histopathological examination of this cornea showed almost total loss of keratocytes and depletion of endothelial cells. Although TEM was not performed to confirm the presence of herpesvirus-like particles and immunohistochemistry was equivocal, ISH and positive PCR amplification for herpes simplex virus DNA confirmed the presence of HSV DNA. Similarly Cockerhamet al,8 in a retrospective study of primary graft failures, demonstrated HSV DNA by PCR from two out of three donor corneas. In neither case did the recipient cornea have amplifiable HSV DNA. In a further study, DNA belonging to HSV types 1 and 2 was amplified in eight out of 19 donor corneas with primary graft failure but not in control corneas.9 Their findings led them to believe that HSV in the donor cornea may be pathogenic in some cases of primary graft failure. The question arises as to whether the amplification of HSV DNA fragments by PCR is adequate proof of virus capable of replicating in the tissue. In both our patients virus was cultured during the acute stages implying active viral replication in these tissues and large numbers of virions were demonstrated in the removed graft buttons by electron microscopy.
Our second patient developed a persistent central epithelial defect in the donor cornea after 1 week. This enlarged to involve the host cornea despite treatment with topical antibiotics and bandage contact lenses. Only after a delay of a few weeks was herpes simplex identified in culture from a corneal swab. This delay in diagnosis is commonplace, typical dendrites being seen rarely in newly acquired HSV keratitis after PK.10 There have been several other reports of persistent epithelial defects appearing in grafts shortly after transplantation proved to be due to HSV in individuals with no previous history of HSK.12 13 The incidence of HSK after PK has been quoted as being over 14 times higher than that in the normal population.13 These reports assert that a high index of suspicion should be maintained, even when the recipient has had no previous history of herpetic eye disease. It can be argued that increasing the frequency of administration of topical steroids from the first postoperative day may have averted the progression of primary graft failure in the first patient. However, without the concomitant administration of antiviral agents, it is unlikely that this would have altered the clinical course, as endothelial necrosis can result from a direct cytopathic effect of viral replication occurring unchallenged in a steroid treated environment.
There may be several sources of HSV in patients following keratoplasty including endogenous reactivation of latent virus from the trigeminal nerve18 and the host's own cornea,19 as well as exogenous transmission from the transplanted donor cornea.7 PCR performed on the excised corneal buttons of our recipients confirmed the absence of HSV DNA and HSV antigens, which suggests that the hosts' corneas were an unlikely source of infection. It is still possible that surgical trauma may have reactivated latent virus within their trigeminal nerves with subsequent corneal infection via the corneal nerves. Nicholls et al in an experimental animal model proposed that in latently infected animals, severing corneal nerves during PK caused reactivation of HSV in the trigeminal ganglion and its subsequent release from the nerve endings in the cornea. They demonstrated that the graft-host junction was the region in which release and spread of virus was greatly facilitated but failed to demonstrate spread far into the recipient or donor cornea.18 This mechanism seems less likely in both cases that are presented here, as the graft-host junction was not the initial site of the disease. In patient 1 the whole graft failed within a week, and in patient 2 the central cornea was the initial site of disease, also occurring within a week.
If infection were introduced to an immunologically naive host from transplanted cornea then one may detect a rising titre of anti-HSV antibody. However, this has never been described in any clinical situation and, moreover, has not been demonstrated experimentally.20 It remains uncertain whether serology would be sensitive enough to detect a rising titre of antibody resulting from a localised corneal infection.
Confirmation of infection originating from donor tissue could have been obtained by culturing HSV from the donor fellow cornea that had undergone endothelial necrosis in organ culture. Comparing viral DNA obtained from the donor fellow cornea with that from the transplanted cornea could have proved this pathway of infection if they were shown to be identical. Unfortunately this was not possible, as the fellow donor cornea had been discarded. Another possible source of proof could have been analysis of any viral DNA present within the donor corneoscleral rim. However, this tissue is not routinely stored. Thus, we have no definite proof of the route of infection.
Screening of donor cornea culture fluid for HSV DNA, using a PCR assay, has been considered unjustifiable in a study by Morriset al.21 Only 3.8% of 80 corneas were positive for HSV, yet in all three instances the corneas were successfully transplanted without evidence of primary graft failure, or HSV induced eye disease. Similarly Garweg and Boehnke22 demonstrated HSV-1 DNA by PCR in seven out of 451 fluid samples from organ cultured corneas. A post-transplantation history obtained from four of these corneas with positive PCR for HSV showed an uneventful postoperative course, as did the history of their partner tissues. Cleator et al also found HSV DNA in low levels in some normal corneas destined for transplantation.7 From their observation of an uneventful postoperative course in patients receiving donor corneas possessing HSV DNA, Garweg and Boehnke reasoned that HSV is not transmissible through corneal transplantation.22 Additionally, they found no evidence of viral replication in organ culture and argued that if HSV were capable of reactivation, organ culture would provide the ideal environment for this to occur. However, recent evidence of epithelial dendritiform lesions occurring in donor corneas during organ culture suggests HSV-1 is capable of active replication in this medium.23 24 In one of these cases this was followed several days later by total necrosis of the corneal endothelium24 supporting claims that endothelial necrosis is another manifestation of HSV reactivation in stored donor corneas.
Endothelial necrosis in culture should alert eye bank staff to the possibility of HSV infection being present in the donor mate. We recommend that when endothelial necrosis in a stored donor cornea is noted the fellow eye, if still in storage, should not be used. We would further recommend storage of corneas in which endothelial necrosis has occurred if the fellow cornea has already been transplanted. This may confirm the source of infection in cases of primary graft failure where herpes simplex has been implicated.
We conclude there is now sufficient evidence that HSV be considered as a serious viral pathogen transmissible by corneal transplantation and in particular as a cause of a persistent non-healing epithelium and of primary graft failure.
Acknowledgments
The authors thank Pat Tarpey and Graham Bigley, Department of Histopathology, Clinical Sciences Building, Central Manchester Healthcare Trust, for their valuable assistance in performing the electron microscopy and immunohistochemistry, and Boris Marcyniuk and Tom Kelly, The David Lucas Manchester Eye Bank, Manchester Royal Eye Hospital, Oxford Road, for providing details of the donor corneas in the eye bank.