Article Text

Abstract
AIM To determine the visual benefit of cataract extraction in patients with retinitis pigmentosa and to identify risk factors for poor outcome.
METHODS A retrospective analysis was undertaken of a continuous series of 142 eyes of 89 patients with retinitis pigmentosa undergoing cataract surgery between 1985 and 1997.
RESULTS Mean age at surgery was 47.5 years (range 24–81 years). In 100 eyes there was posterior subcapsular lens opacity alone, 37 eyes also had moderate nuclear sclerosis, and five had only nuclear sclerosis. All patients had central visual fields of <10°. Overall, mean visual acuity improved from 1.05 (SD 0.38) preoperatively to 0.63 (SD 0.49) postoperatively on the logMAR scale. Significant postoperative capsular opacification occurred in 88/139 eyes (63%) and 45.1% required capsulotomy. Anterior capsulotomy was undertaken in 5/52 (9.6%) eyes undergoing phacoemulsification. Postoperative macular oedema was noted in 20 (14%) eyes. Visual acuity improved in 109 eyes (77%), was unchanged in 29 eyes (20.5%), and worsened after surgery in four eyes (2.5%). 86/89 patients reported major improvement of visual function.
CONCLUSIONS Cataract surgery for relatively minor lens opacities is beneficial in patients with retinitis pigmentosa, and most report subjective improvement of visual symptoms. The incidence of capsular opacification is high and anterior capsular contraction may occur. The number of eyes with poor vision due to macular oedema was unexpectedly low.
- retinitis pigmentosa
- cataract
- clinical outcome
Statistics from Altmetric.com
Cataract is a recognised complication of all types of retinitis pigmentosa (RP). When compared with patients with age related cataract, patients with RP develop lens opacities at a relatively young age.1-3 In addition, in the presence of RP, a relatively minor lens opacity may cause disproportionate functional symptoms. Apart from the general risks of cataract surgery, there are specific additional factors that may result in a poor visual outcome after cataract extraction in the presence of RP. These include:
- (1)
Outer retinal atrophy at the macula in advanced RP.
- (2)
Macular oedema is a common complication of RP, occurring in approximately 10–15% of patients,45 although a prevalence of up to 70% has been reported on fluorescein angiography.67 Macular oedema (Irvine Gass syndrome) develops in approximately 1% of normal patients after cataract surgery using current surgical techniques,8 and it might therefore be expected that cataract surgery would precipitate or exacerbate macular oedema in patients with RP.
- (3)
There is a risk of phototoxic retinal damage in normal patients undergoing cataract extraction.9 The threshold for light damage is probably lower in RP, which could adversely affect visual outcome.
- (4)
Posterior capsular opacification and anterior capsular contraction is more aggressive in the presence of RP,10-19 The reason for the increased cellular proliferation on the capsular remnant in retinal dystrophies is unknown, although the cellular nature of the posterior capsule in retinal dystrophies may account for this.19-21
Despite the potentially poor result in terms of visual acuity, we consider that it is important that patients with RP and cataract are offered early cataract surgery. However, patients should also have realistic expectations of the outcome of surgery. To provide better data on the incidence of these complications and their effect on outcome, and hence the potential risks and benefits of surgery, we have reviewed the records of a large series of patients with RP who had cataract surgery.
Patients and methods
The records of all patients with RP who had cataract extraction between 1985 and 1997 were assessed retrospectively with regard to age, heredofamilial pattern of RP, visual fields (Goldmann or confrontation if very constricted), morphology of cataract, preoperative and postoperative symptoms and visual acuity, surgical complications, incidence of macular oedema and capsular opacification, and subjective response to surgery. The Snellen visual acuity preoperatively and at the time of discharge from the cataract service was converted to the logMAR scale. Recommendation for surgery was made when the lens opacities were considered as the cause of poor central vision rather than macular changes. Surgery was either by extracapsular or phacoemulsification technique, with the coaxial illumination reduced to the lowest practicable level.
Results
There were 89 patients (142 eyes) with RP who had cataract surgery between 1985 and 1997 (54 male and 35 female). Mean follow up was 32.7 months (range 1–156 months). The average age at surgery on the first eye was 47.3 years (range 24–81 years) and 48.9 years for the second eye. Patients with X linked disease had surgery approximately 10 years earlier than the other groups (Table 1). The most common visual complaint was of glare and blurring of vision in bright light, and all patients had preoperative visual fields of ⩽10°. The predominant cataract morphology in 137 eyes (96.5%) was a combined posterior cortical and posterior subcapsular lens opacity; 37 (27%) of these also had some nuclear sclerosis and five eyes only had nuclear sclerosis. The morphology of the cataracts did not differ significantly between heredofamilial groups on clinical examination. Extracapsular cataract extraction and intraocular lens (IOL) implantation was undertaken in 90 (63%) eyes, and the remainder had phacoemulsification and IOL implantation. Three eyes had a posterior capsular rupture during surgery; of these, one had an anterior chamber IOL and two were left aphakic.
Heredofamilial type of RP and age at surgery
VISUAL ACUITY
The average preoperative logMAR acuity was 1.05 (SD 0.38), with a range of 0.3–2.2. Only one patient had an acuity of 0.3 or better before surgery. Overall, visual acuity improved to 0.63 (SD 0.49) postoperatively on the logMAR scale, an average improvement of 0.42 log units.
Following surgery, the best spectacle corrected visual acuity improved in 109 eyes (77%), was unchanged in 29 eyes (20.5%), and worsened in four eyes (2.5%). The preoperative visual acuity of the 29 eyes which had no visual improvement following surgery was worse than eyes that improved, with an average preoperative logMAR acuity of 1.23 (range 0.5–2.2). A subjective improvement of symptoms was reported in 86 (96.6%) patients.
MACULAR OEDEMA
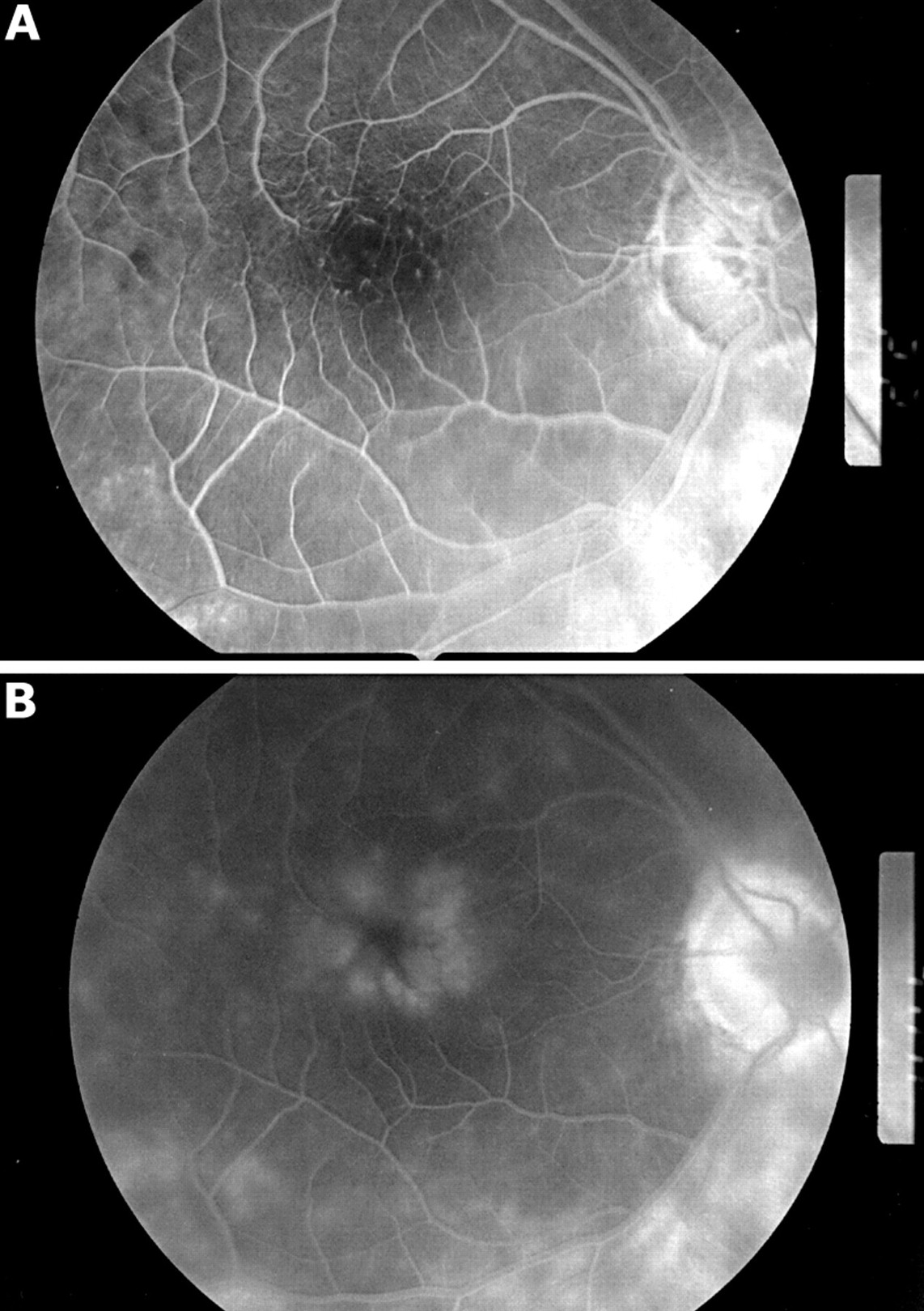
Macular oedema was identified postoperatively in 20 (14%) eyes by fluorescein angiography (Fig 1), and was suspected in a further 15 eyes, although angiography was not undertaken in all these. In those eyes in which postoperative macular oedema was noted, the mean visual acuity still improved from 0.98 preoperatively to 0.52 postoperatively on the logMAR scale. Macular oedema that was not noted preoperatively was present in all four eyes in which the visual acuity deteriorated after surgery; in one eye this only developed after exchange of an IOL that dislocated following a YAG laser anterior capsulotomy.

{kind=link}
Macular oedema in a patient with RP. (A) Early phase of fluorescein angiogram, (B) late phase of fluorescein angiogram.
CAPSULE OPACIFICATION
There was a high incidence of posterior capsular opacification. YAG laser capsulotomy was performed in 60/139 (43.2%) eyes, but this incidence increased to 51% in those eyes with more than 6 months of follow up (118 eyes). A further 28 eyes had capsular thickening which was not considered sufficient to cause visual impairment or there was macular oedema that might have been aggravated by intervention. Five patients with anterior capsular contraction required either a surgical or a YAG laser anterior capsulotomy.
Discussion
Patients with RP typically develop a combined posterior cortical and posterior subcapsular cataract which, when combined with a restricted central visual field, may cause significant additional visual disability even when the opacity appears to be relatively minor. Glare is a major symptom and patients may require cataract extraction at a relatively young age. The mean age at surgery of 47–58 years in previous studies13-1619 and 47.5 years in our study compares with the mean age at surgery of 72.5 years for age related cataract at this institution.22 The age at surgery was lower in patients with X linked RP in our study.
The visual acuity in 23% of eyes did not improve after surgery, and their preoperative visual acuity was worse than the group as a whole. Postoperatively, the majority of these eyes had confirmed or suspected macular oedema but we could not exclude preoperative macular oedema in all of these cases. Macular oedema in RP can be difficult to diagnose owing to the extremely slow leak of fluorescein on angiography, irregular pigmentation at the level of the retinal pigment epithelium, and the reluctance of the ophthalmologist to subject the patient to the bleaching effect of the procedure. In all four cases in which the visual acuity deteriorated following surgery macular oedema was documented, although in one case this only occurred after secondary intraocular surgery. The incidence of postoperative macular oedema was lower than we had expected.
Over 96% of patients reported a functional improvement in their visual symptoms following surgery despite the acuity being unchanged or worse in almost a quarter of eyes. This suggests that other measures of visual function may be indicated when assessing patients with RP for cataract surgery and evaluating benefit.
The high incidence of capsule opacification (63%) in this series is comparable with other reports.13 Not all of these eyes have had a capsulotomy, either because of the pre-existence of suspected macular oedema or because it was considered that the capsular opacity was not sufficient to reduce visual function. As 24 eyes had less than 6 months of follow up it is probable that final percentage requiring capsulotomy will be higher. The reason for the high incidence of posterior capsular opacification in patients with RP is not understood, but mediators released by the neurosensory retina may modify lens fibre growth and differentiation.11 It has been suggested that the abnormal retina causes a hypercellular posterior capsule and the characteristic posterior cataract in RP,1219-21 and as this is not influenced by surgery continued cellular growth might be expected. Similar stimuli may cause the contraction of the anterior capsulorhexis that was observed in five of the 52 (9.6%) eyes that had phacoemulsification, leading to dislocation of the foldable plate-haptic silicone IOL into the anterior chamber in one case. This risk has been previously identified.101823 Hayashi et al reported a 45% decrease in the anterior capsule opening at 6 months after surgery in patients with RP compared with a decrease of 4.6% in a control group.18
It is evident from our series that patients with RP benefit from early cataract surgery, and that the vast majority have a subjective improvement in their symptoms of glare. The benefit of surgery for patients with a poor preoperative visual acuity is less marked, usually because of pre-existing macular disease, but postoperative macular oedema was less common than expected. Patients with RP appear to be susceptible to anterior capsule contraction and therefore a small capsulorhexis should be avoided. It would appear to be sensible to avoid silicone IOLs because of the risk of their dislocation if an early capsulotomy is required.