Article Text

Abstract
AIMS To determine the accuracy of intraocular lens (IOL) power calculation in a group of pseudophakic children.
METHODS A retrospective analysis of biometric and refractive data was performed on 52 eyes of 40 infants and children, who successfully underwent cataract extraction and IOL implantation. The following parameters were included: age at the time of surgery, keratometry, axial length, estimated refraction, and the power of IOL implanted. The postoperative refractive outcome was taken as the spherical equivalent of the refraction at 3 months after surgery. The prediction error was taken as the absolute difference between the estimated and actual postoperative refraction. The data were analysed to assess the effects of age at the time of surgery, keratometry, and axial length on the accuracy of calculation of IOL power.
RESULTS For the overall group the mean and median prediction errors were 1.40 D and 0.84 D (SD 1.60). The mean and median prediction errors in eyes with axial lengths ⩾20 mm were 1.07 D and 0.71 D (SD 0.98) and in eyes <20 mm were 2.63 D and 2.61 D (SD 2.65). The mean and median prediction errors in eyes in children aged ⩾36 months were 1.06 D and 0.68 D (SD 1.02) and in children aged <36 months was 2.56 D and 2.29 D (SD 2.50). The differences between the prediction errors for both axial length and age were statistically significant (p<0.05).
CONCLUSIONS For the overall group IOL power calculation is satisfactory. In eyes with axial lengths less than 20 mm and in children less than 36 months of age larger errors can arise. This study demonstrates the need for an IOL formula specifically designed for paediatric use.
- intraocular lens
- paediatric cataract surgery
Statistics from Altmetric.com
Posterior chamber intraocular lens (IOL) implantation is gaining widespread use in the treatment of childhood cataract, as a consequence of advances in microsurgical techniques and IOL design. Recent reports have indicated that lens implantation in older children is a safe and effective treatment although not without some risk, including fibrinous uveitis, pupil capture, and capsular fibrosis.1-4 There is a growing trend towards IOL implantation surgery in infants,5 whose eyes are still undergoing rapid growth and refractive change.67 Many surgeons choose to aim for postoperative hypermetropia in young children and infants to allow for myopic shift as the eye grows.28-10 It is therefore fundamental that the calculation of IOL power should be as accurate as possible in giving a predictable postoperative refraction.
Many formulas have been devised, the first generation formulas being theoretically derived1112 but proving to be inferior to the empirically derived formulas.13 Since then new generation formulas have come into existence which are modifications of previous theoretic and regression derived formulas including the SRK II and Holladay formulas. The SRK/T formula14 was developed using theoretical formulas addressing the issues of postoperative anterior chamber depth, retinal thickness, and corneal refractive index optimised by regression analysis. Despite this refinement in IOL formulas, there is evidence that those in current use have lower predictive accuracy in eyes with very short axial lengths.1516
Methods
All children (age <16 years) who underwent uncomplicated cataract surgery and IOL implantation between February 1994 and February 1998 were included in the study. We retrospectively reviewed the records of 40 children and data on 52 eyes are presented. All children had congenital or developmental cataract. No children in the group developed glaucoma preoperatively or postoperatively. Keratometry was performed using a Nidek hand held keratometer and axial length measurement using a Storz Compuscan. Measurements were taken on cooperative older children in clinic and on young children under general anaesthesia just before cataract surgery. Over the study period the SRK II and SRK T formulas were used, in conjunction with the IOL manufacturers' A constants, to calculate IOL power. All children <12 months of age at the time of surgery had IOL power calculated using the SRK/T formula.
SURGICAL TECHNIQUE
Cataract surgery was performed through a tunnelled scleral incision. A keratome was used to enter the anterior chamber through clear cornea in a stepped fashion. Continuous circular capsulorhexsis or “can opener” capsulectomy (in surgery before 1995) was performed under viscoelastic. Lens material was removed using an automated irrigation/aspiration technique and the wound was enlarged to allow implantation of a rigid poly(methylmethacrylate) IOL into the capsular bag. Wound closure was performed using 10/0 Vicryl or 10/0 monofilament nylon sutures.
The power of the IOL implanted, the estimated postoperative refraction, and the age at the time of cataract surgery were recorded. The early postoperative refractive outcome was taken as the spherical equivalent of the refraction at 3 months after surgery. The absolute difference between estimated and actual postoperative refraction was calculated for all eyes and this was termed the prediction error. The data were analysed to assess the effects of axial length, keratometry, and age at the time of surgery on the accuracy of IOL power calculation. The differences between subgroups were analysed using the Mann-Whitney U test, with p <0.05 regarded as significant.
Results
Twelve children underwent bilateral IOL implantation and all children <36 months of age underwent unilateral IOL implantation surgery. Figure 1 shows age at time of surgery versus axial length.
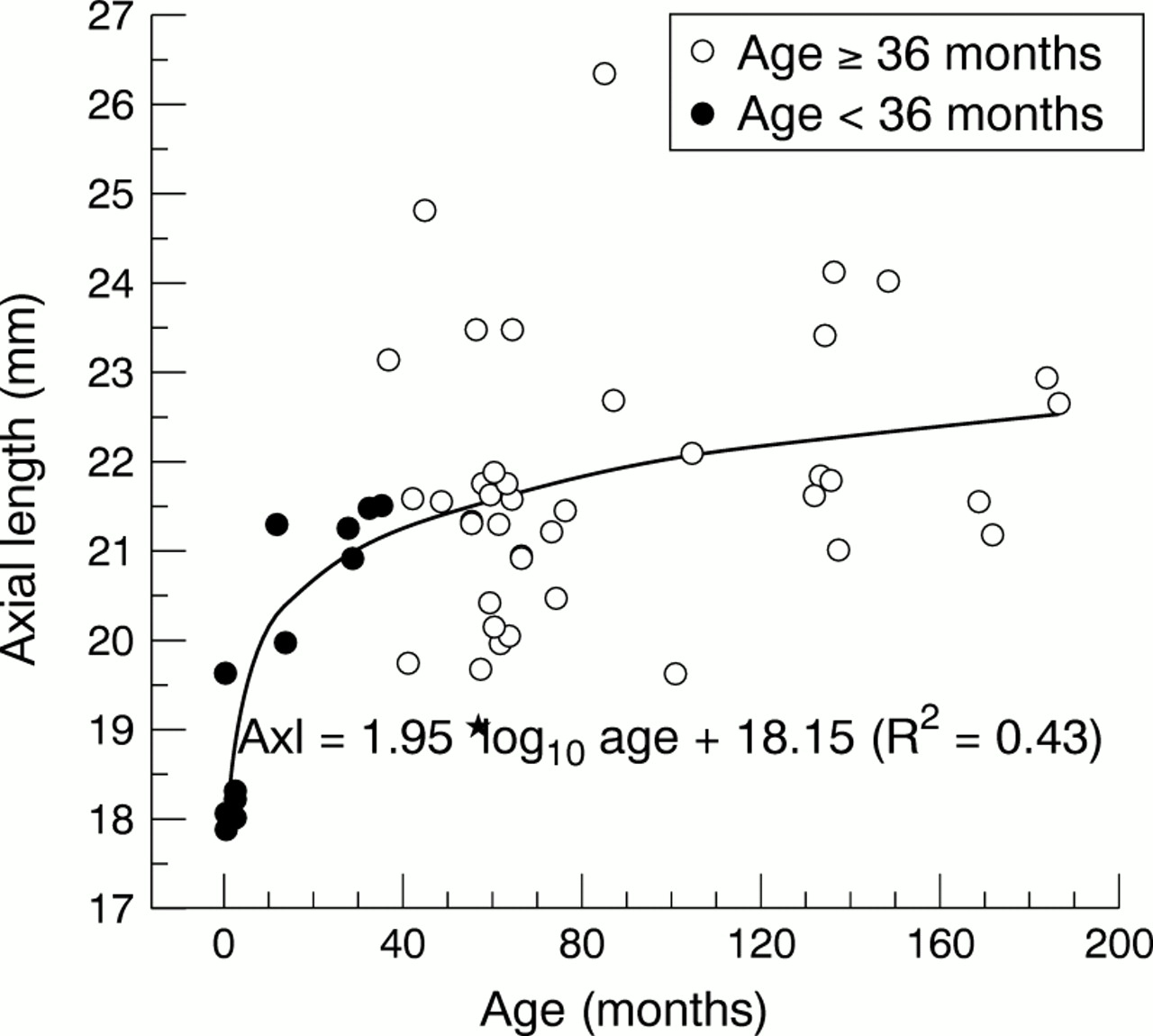
Axial length (mm) versus age at surgery (months).
For the overall group of 52 eyes, axial length ranged from 17.9 to 26.36 mm (mean 21.34, median 21.41, SD 1.72), corneal radii from 6.58 to 8.43 mm (mean 7.57, median 7.62, SD 0.41), and age at the time of cataract surgery from 1 to 186 months (mean 70.48, median 60.5, SD 49.68).
Table 1 shows the prediction error data in the subgroups used for the statistical analysis. The data were subdivided for the eyes with axial lengths <20 mm and ⩾20 mm, corneal radii <7.3 mm and ⩾7.3 mm, and age at surgery <36 months and ⩾36 months.
Prediction errors for the subgroup data
For the overall group the prediction error ranged from 0.07 to 9.19 D (mean 1.4, median 0.84, SD 1.6). Prediction error was significantly greater in eyes with axial lengths <20 mm (p = 0.04) and in eyes in children <36 months at the time of surgery (p = 0.03). There was a trend towards greater prediction error in eyes with corneal radii <7.3 mm, but this was not significant (p = 0.2).
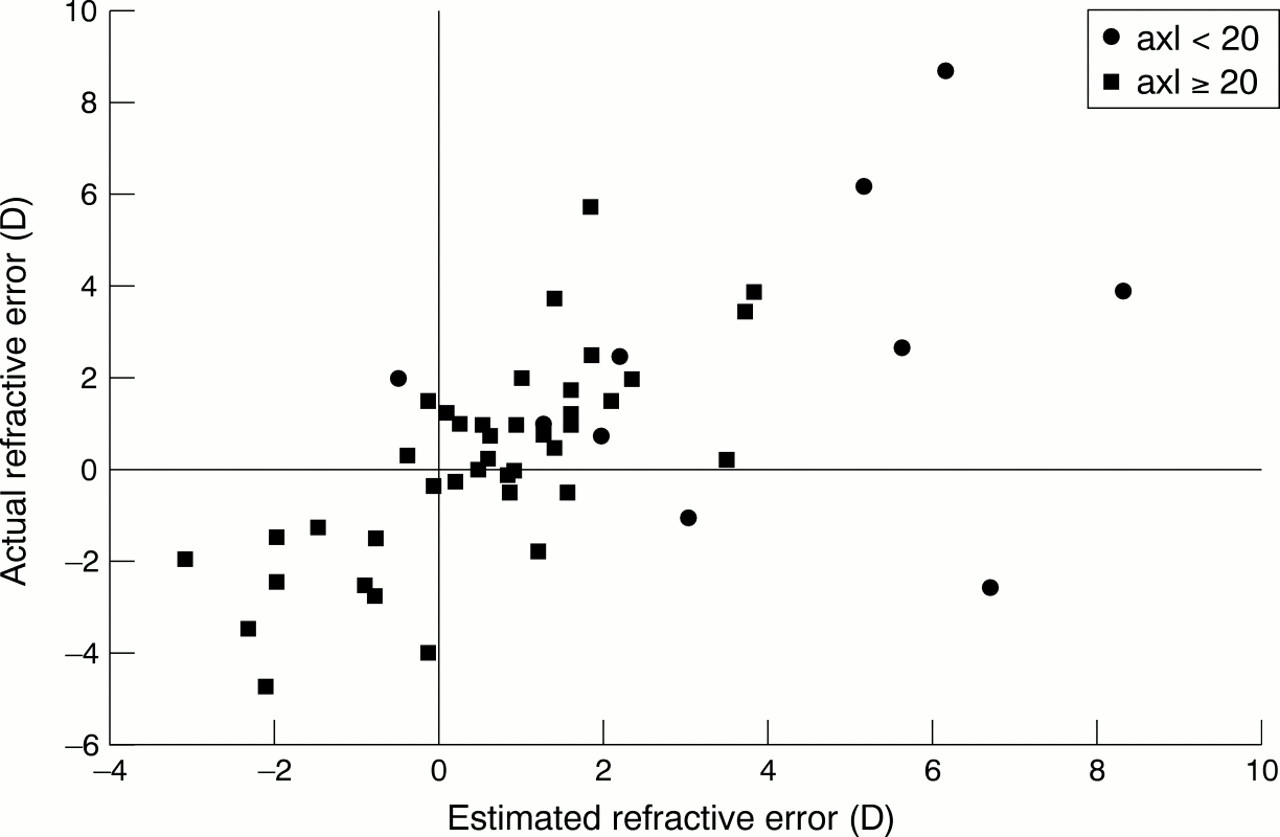
Figure 2 shows a scatter plot of estimated refractive error versus actual refractive error for axial length <20 mm and ⩾20 mm. This shows a tendency for the shorter eyes to have a lower actual than estimated refraction—for example, one of the eyes was estimated to be +6.69 D postoperatively but the actual refraction was –2.50 D, creating a prediction error of 9.19 D. Other shorter eyes with estimated hypermetropic outcomes were found to be nearly emmetropic postoperatively.
{kind=link}
{kind=link}
Estimated refractive error (D) versus actual refractive error for axial length (axl) <20 mm and ⩾20 mm.
Discussion
Several investigators have reported that formulas currently in use have lower predictive accuracy in eyes with shorter axial length.17 Our results show that for the overall group, the prediction error is satisfactory and is comparable with errors demonstrated in adult groups.16 In our study there was a trend towards a greater prediction error in eyes in children less than 36 months of age, in eyes shorter than 20 mm, and in eyes with corneal radii less than 7.3 although for the latter, sample size is too small to reach significance.
Errors in calculating IOL power may arise in several ways:
(1) INSTRUMENTATION ERROR
Automated keratometry has been shown to be comparable to manual keratometry in adults.18 The steeper corneas of infants may result in inaccuracy, although the effect overall is likely to be small in the calculation of IOL power. Commercial biometers are optimally adapted for measurement of adult eyes and gates may not be set to receive echoes from shorter eyes (see Fig 2 for example). This was the case for Compuscan, which gave a minimum axial length of 17.8 mm. It is therefore essential to ensure that instruments can be calibrated to accept shorter axial length readings. Most instruments use average sound velocity (1550 m/s),19 but in small eyes with congenital cataract the lens is a greater proportion of the total axial length and therefore the average velocity would be faster. Also in eyes with other abnormalities such as persistent hyperplastic primary vitreous the average sound velocity may be inappropriate.
(2) SURGICAL ERROR
Intraocular positioning of the IOL will affect the prediction error, with sulcus fixation producing a relative myopic shift from the estimated refraction. In our series four out of 52 IOLs had hybrid capsular bag/sulcus fixation and three of these eyes had a more myopic refractive error than was estimated. However, the sample size is too small to allow further analysis of this effect on prediction error.
(3) FORMULA ERROR
In our series SRK II and SRK/T formulas were used, although the results were recalculated for SRK/T for analysis of prediction error. It has been shown that the third generation theoretical formulas are more accurate for short eyes. This was attributed to their improved prediction of postoperative anterior chamber depth (ACD). However, the mean ACD in infant eyes is less than that of adult eyes20and this may contribute to inaccuracy of IOL power calculation using current formulas. One strategy for improving prediction accuracy is to measure postoperative ACD and back calculate to modify the IOL formula as suggested by Holladay.21
In a recent study Inatomi22 showed that the SRK/T formula was more accurate than empirical formulas for calculating IOL power in eyes with microphthalmos (axial length <19 mm) and they found increasing prediction error for the shorter eyes in their series.
(4) EYE GROWTH
Figure 1 showed that eyes that had surgery at age <36 months also tended to have shorter axial lengths. It is expected that there will be changes in the ocular dimensions in this group, especially when surgery is performed in the first few months of life. The resulting myopic shift910 will lower the estimated refraction, and this should be borne in mind when comparing estimated and actual refractive outcomes.
In conclusion, the SRK/T formula for IOL power calculation gives satisfactory accuracy overall in predicting postoperative refractive error. However, in eyes with axial lengths shorter than 20 mm and in eyes in children less than 3 years of age unacceptably large prediction errors can arise. There is a trend towards greater prediction error in eyes with corneal radii <7.3 mm, although the sample size is too small for this to reach statistical significance. This study demonstrates the need to identify sources of calculation error, to study the rates of growth of implanted eyes, and to develop an IOL formula specifically designed for paediatric use.
Acknowledgments
The authors would like to thank Dr Neil Parry and Ms Sue Ritchie for their assistance in the preparation of this manuscript.