Article Text

Abstract
Background/aims: It is well documented that non-concordance with occlusion therapy is both substantial and a major factor leading to treatment failure. Parental understanding in previous work has been found to be poor in key areas such as the critical period and effect of age on prognosis. Research in other areas of medicine has shown that the level of understanding can have a direct effect on the level of concordance. The aims of this study were to assess the ability of educational material in the form of a leaflet, to improve parental understanding of amblyopia and occlusion, and subsequently increase concordance.
Methods: Parents of children aged between 1 and 7 years receiving a minimum of 1 hour of occlusion for amblyopia were recruited. A randomised controlled trial was undertaken where, on inclusion, the patients were randomised into a leaflet group, whose parents were issued with written educational material, and a control group whose parents did not receive the written information. Patients were paired and matched for age (<2 years difference) and amount of prescribed occlusion (no more than 1 hour difference). Concordance was monitored by a parental diary and knowledge and parental reasons for non-concordance were assessed by a questionnaire. Concordance was analysed by means of a concordance index and by calculating the proportion of non-concordant parents by setting a threshold of concordance at 80%.
Results: Parental knowledge was significantly greater in the leaflet group (88% had complete knowledge) compared to the control group (49% had complete knowledge) (p <0.001). There were also differences between the groups in the area of the treatment regimen, with errors only occurring in the control group (three patients occluded the incorrect eye), but this did not reach statistical significance. Concordance was significantly greater in the leaflet group (mean concordance index 0.85) compared to the non-leaflet group (mean concordance index (0.71) (p <0.001). Comparison of the proportion of non-concordant parents was also statistically different (p <0.005) at 0.23 (95% CI 0.13 to 0.35) for the leaflet group compared to 0.54 (95% CI 0.41 to 0.67) for the control group.
Conclusion: A large proportion of patients would benefit by increasing parental knowledge in key areas such as the critical period, importance of occlusion, and potential negative consequences of not treating amblyopia. Written information is a simple, inexpensive, easy to implement, yet effective method of improving parental understanding and subsequent concordance.
- concordance
- compliance
- occlusion
- amblyopia
- randomised controlled trial
Statistics from Altmetric.com
Non-concordance is consistently reported as a major factor contributing to the failure of occlusion therapy.1–5 The extent of non-concordance is substantial and has recently been reported to be as high as 54%.6 Other studies have reported levels of non-concordance ranging between 49%7 and 12%.4 It is difficult to compare these studies however, as methodological differences in areas of study design (prospective v retrospective) and the method of measurement used (parental diary v clinic attendance) will undoubtedly have influenced the recorded level of non-concordance. Various factors relating to non-concordance have been proposed including increasing age,5 decreasing age,4 social deprivation,7 low visual acuity,4 and poor parental understanding of the critical period and treatment regimen.6 Of these, parental understanding is unique as this factor could be easily manipulated by educational material.
In order to achieve concordance with occlusion therapy, which may at times be difficult to implement because the child might be unwilling to cooperate or it might be considered socially undesirable, parents must have full understanding of the issues surrounding amblyopia and its treatment. Knowledge is required of the critical period and the reducing prognosis with age. This would help induce a sense of urgency and prevent the treatment being delayed by the parents until a time when they consider the occlusion would be more easily tolerated. Understanding of the aims of the occlusion therapy is also required. Parents who believe that surgery is an option if the occlusion fails may be less likely to concord and parents may become disillusioned if they incorrectly believe that wearing the occlusion will eradicate the strabismus. Finally, a lack of understanding of the treatment regimen, of either which eye to occlude or the length of prescribed occlusion wear would also lead to non-concordance. Understanding has been shown in other areas of medicine to have an impact on concordance via its effect on memory and satisfaction.8 These effects are illustrated in an adaptation of Ley's cognitive model (Fig 1).9 Understanding of amblyopia and related issues has a direct effect on increasing concordance and an indirect effect by improving memory and satisfaction following the consultation. A major review undertaken in the area of concordance in general medicine10 revealed that the main factors associated with non-concordance were the Health Belief Model variables (perceived vulnerability, seriousness of the illness, effectiveness of the treatment, and costs and barriers),11 influence of family and friends, duration of therapy, complexity of regimen, patients' satisfaction, patients' expectations being met, and level of supervision by the therapist. The majority of the factors are pertinent for occlusion therapy and most would be strongly influenced by the extent of parental understanding.
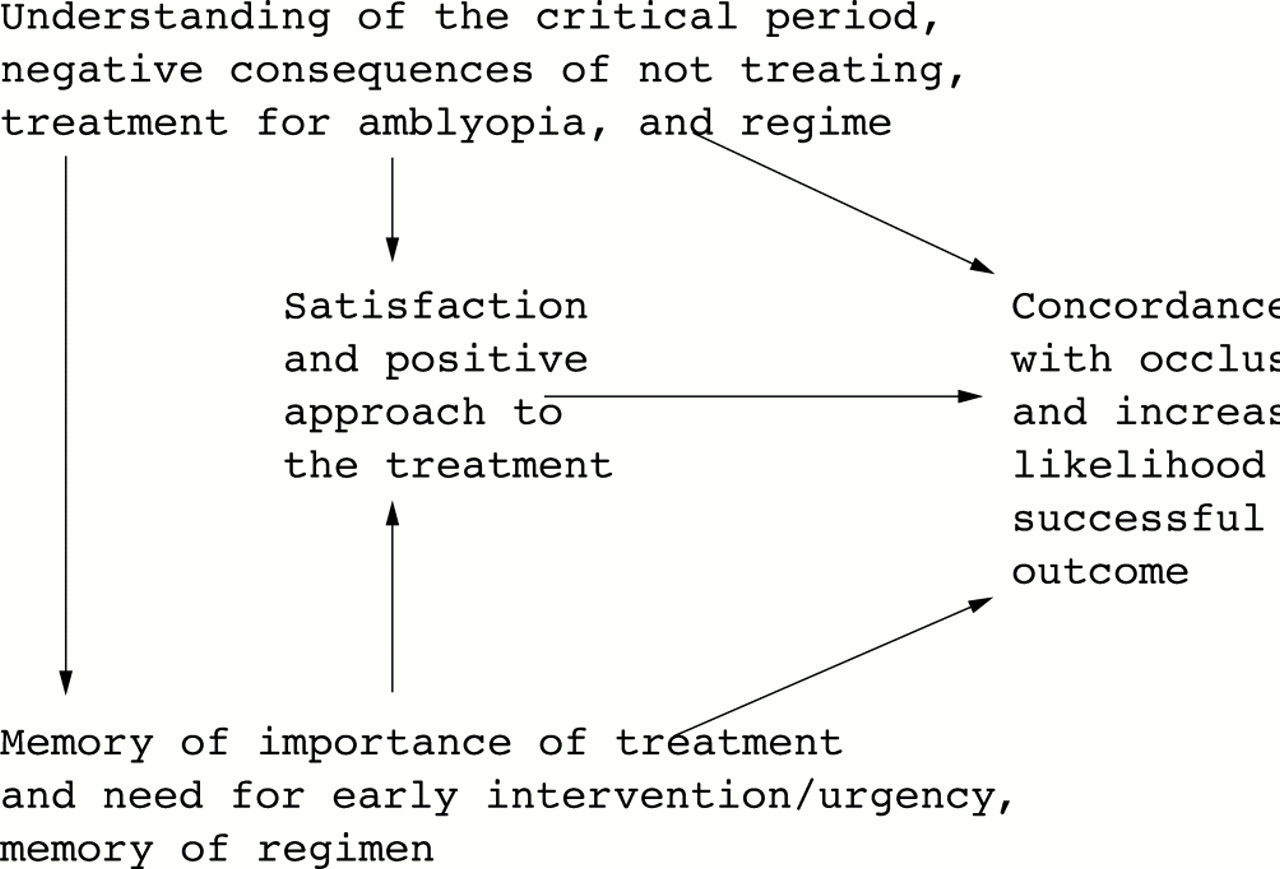
Adaptation of Ley's cognitive model.
Parental understanding would therefore seem to have a key role in determining the level of concordance with occlusion therapy. In various areas of medicine, understanding of medical information has been shown to be poor12 and this may be attributable to the use of medical jargon,13 patients' own theories about their illness,14 a reluctance to ask questions,15 and a poor memory for information when presented in a verbal format.16 Recall of information has been shown to be far higher in patients who received written information compared to those who did not.17 A review of research investigating the effects of written information revealed that 97% of the studies reported increased knowledge, 60% had increased concordance, and 57% demonstrated an improved outcome.18 In the field of occlusion therapy understanding of amblyopia and related areas was shown to be greater in a group who received a booklet, compared to those who did not and there was also a change in attitudes (related to the Health Belief Model variables) towards the disease and treatment that would be likely to increase concordance.19 The study, however, did not explore the effect of the increased understanding and improved attitudes on concordance. The aims of this study therefore were to assess the effect of a leaflet on the level of knowledge in key areas of amblyopia and occlusion therapy and to determine the effect of increased understanding on parental concordance.
MATERIALS AND METHODS
A detailed description of the methods used in this study has already been documented in earlier work.6 To summarise, all patients (new and existing) receiving a minimum of one hour's occlusion for all types of unilateral amblyopia were eligible for recruitment, following informed parental consent. Patients meeting the inclusion criteria were recruited over a 3–4 month period. On inclusion to the study patients were randomised into a leaflet group (who received educational information in the form of a leaflet) or a control group (who did not receive written educational material). The method chosen for randomisation was the tossing of a coin as this is a simple method, easily implemented by the clinicians, and requires the least instructions to follow so as to not unduly increase their workload. The dependent variable in this study therefore was concordance with occlusion therapy, the independent variable was parental understanding and knowledge of amblyopia, occlusion therapy, critical period, and prognosis. The independent variable was manipulated by educational material in the form of a leaflet. Patients were paired, being matched for age (allowing up to 2 years difference) and the length of prescribed occlusion time (allowing up to 1 hour difference). While it is disputed whether the age of the patient and severity of amblyopia are related to concordance, pairing of these variables was necessary to eliminate any possible effect on the concordance. In order to accurately match the children in both groups a quasi-randomisation technique was used. Children were randomly assigned to one of the groups and their length of prescribed occlusion and age was noted. The process continued and the children were paired in line with the criteria stated above. As the required number of patients in each group was reached any remaining patients who had not been paired were noted. The next patient who attended having met the matching requirements for that individual was then automatically placed in the other group in order to complete the final pairings.
The leaflet was constructed by printing in landscape on both sides of A4 size card; by folding into three, a six page leaflet was produced. The print chosen was Times New Roman, with a minimum of 12 point throughout, as recommended by the RNIB20 to ensure the document was legible. The front of the leaflet was designed to gain the attention of the reader using the title “IMPORTANT” followed by a brief explanation of the aim of the leaflet. The different types of refractive error were then simply explained together with the way in which they are treated by means of spectacle correction. At this point emphasis was placed on the importance of wearing glasses during the critical period. Strabismus was then explained, indicating possible aetiologies. The treatment of strabismus was also discussed with strong emphasis given to the fact that surgery would align a cosmetically poor strabismus but not improve the vision. Finally, amblyopia was addressed. Reasons for amblyopia occurring were given along with information on what the condition actually entailed. Occlusion therapy was stated as the main method of treatment for amblyopia and again strong emphasis was given to indicate that patching should commence as early as possible, vitally before 7 years of age, and that it does not correct the strabismus. The last section of the leaflet indicated the important role of the parents in ensuring the treatment is undertaken effectively and that the children themselves are unlikely at present to be aware of the importance. The final point stressed the potential negative effects of untreated amblyopia, including the risk of blindness following the loss of the non-amblyopic eye and career restrictions. Space was given in this section where details of the treatment regimen, eye to be occluded, and number of hours could be recorded. This could be used for reference by the parents during the treatment in cases of poor memory. Sentences were kept short and simple language used whenever possible.
Concordance was monitored by means of a parental diary. Parents were instructed to record the length of time the patch was worn (to the nearest half hour) each day for a 4 week period. Parental understanding of amblyopia and occlusion and parents' own reasons for non-concordance were determined by means of a questionnaire (Table 1). Parents could choose the reasons they felt most accurately described why they had failed to occlude or, if they wished, provide their own alternative if necessary.
Content of questionnaire
Content and face validity of the diary, questionnaire, and leaflet were assessed by several orthoptists. No revisions were deemed necessary but it was suggested that a reading ease score (Flesch Reading Ease)21 should be calculated using Microsoft Word to ensure that the documents were easily readable. A score of 85 on a 100 point scale was achieved for the questionnaire and a score of 80 for the leaflet. This is well above the recommended minimum score of 70, with a score 80 and above indicating that the text would be understood by a child and 95% of adults between 25 and 65 years.22 The diaries and questionnaires were piloted on parents of 20 children receiving occlusion and the leaflet was piloted on several laypeople. Following this, an extra question (“would occlusion be more effective at 2 years or 6 years?”) was added to the questionnaire to ensure all the elements of the critical period were explored. The laypeople were questioned regarding the material they had read in the leaflet to ensure the desired knowledge had been obtained. No difficulties were encountered regarding ability to understand the content or assimilate the knowledge and thus no changes were made to the leaflet. Analysis of the level of parental knowledge from the pilot study revealed that written information could be expected to increase the proportion of concordant parents by 25% and up to 35% if the effect of the written information on memory was included. A sample size calculation based on the estimated increase in concordance of 25%, with confidence of preventing a type I error at 0.05 and type II error at 0.20, revealed that 55 parents would be required in each group.
Diaries and instructions were issued to the parent at the clinic as soon as they had agreed to join the study and informed consent had been obtained. Those in the leaflet group were also given the educational material aimed to enhance their concordance. After a 4 week period the patients were routinely reviewed at the clinic and at this time the parent was asked to complete the questionnaire. The questionnaires were immediately collected to maximise return rates. The parents were advised that neither the diary nor the questionnaire would be seen by the orthoptist treating their child and, if they wished, the documents could be mailed directly to the author. This would encourage the parents to be open and honest, and reduce any anxiety or feelings that they were in some way being judged. It was not considered necessary to formally mask the orthoptist who collected the questionnaire and diary, as they could not influence the outcome. The number of hours of occlusion wear over the 4 week period was calculated for each patient. Concordance was analysed by means of a concordance index23 where occlusion was recorded in the diary (hours)/prescribed occlusion (hours). Statistical comparison of means was achieved by using a related t test. The proportion of non-concordant parents was also calculated. In order to achieve this it was necessary to set a threshold of concordance. For the purposes of this and previous research6 parents with a concordance index greater than 0.80 were deemed to be concordant. The proportion of parents in the leaflet and control group were analysed using McNemar's test.
RESULTS
A total of 130 patients (65 pairs) were recruited, but eight pairs of patients were lost to follow up. Data on five pairs of patients were lost as a result of diaries being lost by parents and data were lost on three pairs of patients because the diaries were not returned because parents failed to attend appointments. The leaflet and control group were well matched for the variables of prescribed occlusion wear and age. The mean amount of prescribed occlusion for the leaflet group was 3.2 hours (median 3 hours, range 1–10 hours) with a mean age of 4.4 years (median 4 years, range 1–7 years), compared to 3.3 hours (median 3 hours, range 1–10 hours), and 4.6 years (median 5 years, range 2–7 years) for the control group. The age and length of prescribed occlusion of the patients that were excluded were not markedly different from the sample that remained.
Parental knowledge
The questionnaires were analysed for both the leaflet and control group. The first four questions explored parental knowledge of their awareness that their child had amblyopia, the treatment for this condition, and the prognosis (Table 2). Parental knowledge in the key area of the critical period was poor in the control group. To determine the effect of the leaflet in improving knowledge, the proportion of knowledgeable parents (achieving all correct answers) was calculated for both groups. For this analysis parents who gave reasons for non-concordance such as “I will wait until my child is older and more cooperative,” “I will wait until my child understands the reasons for the treatment,” and “the treatment does not work” were included with parents who gave incorrect responses to the questions and were deemed to have poor knowledge. Of the leaflet group, 50 parents (88%) had complete knowledge, compared to 28 (49%) of the control group (p <0.001). The next two questions of the questionnaire assessed the information exchange regarding the treatment regimen, which had been recorded on the leaflet. The proportion of parents giving a correct response to the length of time they have been told to occlude was 100% for both groups. However, only 54 (95%) parents in the control group indicated they were occluding the correct eye compared to 57 (100%) for the leaflet group (p >0.05). The reasons given by parents for their non-concordance were evaluated for both groups (Table 3). Two parents with a concordance index of more than 0.80 gave reasons but were not included given the negligible amount of their non-concordance. Each non-concordant parent provided a reason and no parent gave more than one reason. A variety of reasons were given for the non-concordance but comparison of both groups revealed that the most common reasons in the control group were attributable to poor knowledge, accounting for 68% of the non-concordant parents compared to only 15% of the leaflet group.
Comparison of parental knowledge between the leaflet and control group
Comparison of parental reasons for non-concordance between the leaflet and control group
Concordance
The concordance indices were analysed to determine the effect of the increased knowledge obtained by those parents who had received the extra educational material in the leaflet group. The mean concordance index for the leaflet group was 0.85 (median 0.88, range 0.4–1.0) compared to 0.71 (median 0.75, range 0.1–1.0) for the control group (p < 0.001). The proportion of non-concordant parents in the leaflet group was 0.23 (95% CI 0.13 to 0.35) compared to 0.54 (95% CI 0.41 to 0.67) for the control group (p <0.005) (Fig 2).

{kind=link}
{kind=link}
Distribution of parents in relation to the concordance index (n =57 pairs). Open bars represent the control group (n = 57); solid bars represent the leaflet group (n = 57).
DISCUSSION
The patients recruited to the study were representative of the typical amblyopic population presenting at an eye unit. All types of amblyopia were recruited except for stimulus deprivation as no patients presented with this condition during the study period. This simply reflects the reduced incidence of this type of amblyopia and would not have introduced any form of bias to the findings. This is because the aim of the study was to assess the effect of written information on understanding and concordance and not to assess the effect on the outcome of the treatment. Patients in both groups were well matched for age and length of prescribed occlusion. This was considered necessary to eliminate any effect of these variables between the groups, as the effect of age on concordance has been variable between different studies.4,7 Given that the majority of patients could be matched following randomisation, it is not felt that the automatic consecutive placement of some children into one of the groups, in order to achieve accurate matching, would have introduced any substantial bias. Subsequent analysis of the control group demonstrated no correlation between length of prescribed occlusion wear and non-concordance, as reported elsewhere,6 but at the time of the study period no evidence was available to rule out the effect of this potential bias. The level of visual acuity was not matched as the level of prescribed occlusion generally reflects the level of acuity with greater levels of occlusion being prescribed for more severe amblyopia. Also the introduction of another variable, if not absolutely essential, only serves to add methodological problems, making matching of the subjects more difficult.
Parental knowledge of the critical period and the importance of the age at which treatment commences were poor in the control group. Failure of parents to appreciate these facts means that there would be no sense of urgency to the treatment, which itself could lead to non-concordance. Parents may also actively choose to delay the treatment until their child reaches an age when either they can decide whether or not they wish to have the treatment themselves or reach an age when the rationale for the treatment can be more easily explained and understood. Knowledge in the leaflet group was far superior and the educational material was therefore successful in increasing the level of parental understanding in each area that was examined. In order to analyse the difference in knowledge between the two groups quantitatively it was decided to class the parents as knowledgeable only if all questions were answered correctly (and if none of the parental reasons indicated poor knowledge), rather than creating a scoring system. It was considered that a parent could obtain a high score if most questions were answered correctly despite, for example, being unaware of the prognosis being more favourable at 2 years rather than 6 years. Poor knowledge in just one area may have important consequences for non-concordance and a high score in this case would be misleading. It was deemed more useful to identify the proportion of parents who had adequate knowledge from the remainder of parents with inadequate knowledge in whom poor understanding may have contributed to their non-concordance. Three patients in the control group were occluding the incorrect eye compared to no errors in the leaflet group. While the difference between the groups was not statistically significant, it is of clinical significance. The confusion may have arisen owing to a misunderstanding between the clinician and the parent or perhaps because of poor memory, both of which would be improved by increased knowledge. The leaflet used in this study incorporated a space where details of the regimen could be recorded and used for reference at a later date if required. This would help to reduce this type of error but as the proportion of parents who occluded the incorrect eye was low it is not possible from the sample size used to draw any firm conclusions as to whether the leaflet group had no errors as a result of the educational material or simply by chance.
Concordance was significantly greater in the leaflet group compared to the control group. The increase in knowledge achieved by the introduction of written material was therefore successful in improving parental concordance. Significant differences in concordance were present when both the mean concordance indices and proportion of non-concordant parents were compared between the two groups. Clearly the proportion of non-concordant parents will vary depending on where the threshold of non-concordance is set. The 80% threshold was considered a reasonable level to choose, as parents who begin to fall below this level (averaged over the whole treatment period) will be failing to occlude for a substantial period of time. Adjustment of the level of the threshold for non-concordance, either an increase or decrease, did not alter the finding of a statistically significant difference between the groups. The success of the effect of improving understanding and knowledge to increase concordance is important. The extent of the problem of non-concordance with occlusion therapy and the resulting consequences on the outcome has already been discussed and these issues have been well documented. The present study did not aim to assess the effect of concordance on outcome and a much longer follow up period would be required in order to assess this satisfactorily. Although lack of information on outcome may be considered to weaken the possible conclusions that can be made from this study, it has been consistently reported that non-concordance is one of the main factors responsible for treatment failure. While the difficulties in implementing the treatment have been explored, little research has been undertaken to investigate methods that could increase the level of concordance. This study has demonstrated a practical method by which concordance can be improved and as a direct result of this an improvement in acuity would clearly be expected. It is accepted that the level of parental concordance may vary during the treatment period and that this study only assessed a snapshot of one month of the total course of treatment. However, this is unlikely to have any influence on the differences found between the two groups. It is also accepted that written information cannot be expected to improve concordance in all parents. However, analysis of the parental reasons for non-concordance (Table 3) revealed that 68% of parents in the control group gave reasons indicating poor knowledge. It would appear therefore that a substantial number of parents would benefit from extra educational material to increase their understanding and subsequently their concordance. It could be argued that the leaflets would not in fact be read by many of the parents. Research in other areas though does not show this to be the case. Patients generally want to have more information and it has been shown that between 89% and 95% of patients read information booklets.24 This could be maximised if parents were handed the leaflets by a clinician with a verbal reinforcement of the importance of the contents. In order for the leaflets to be effective attention must also be drawn to the presentation and design and a good readability score obtained. For this study the content of the leaflet was designed with the sole purpose of providing and emphasising only key information that would be likely to improve concordance. The aim was not to provide a general information booklet about eyes and strabismus.
The method used to assess concordance was by means of a parental diary. Discussion of its validity and good comparisons with objective techniques have already been made in earlier work.6 It is accepted that this method may lead to some underestimation of the degree of non-concordance as parents may not always fully admit to the extent of their non-concordance. However, steps were taken to minimise this possibility by ensuring confidentiality and anonymity from the orthoptist treating their child. Both groups used the same method to measure the concordance and therefore this area of potential bias would not have influenced the effect of the leaflet on concordance. As objective techniques become more readily available23,25 it would be useful to conduct further research involving methods of improving non-concordance using both diaries and objective patch monitors for comparison.
In conclusion it would be beneficial to a large proportion of patients if their parents were issued with a simple leaflet aimed at improving knowledge in key areas such as the critical period, which also emphasised the importance of occlusion and possible negative consequences of failing to treat amblyopia, in conjunction with verbal reinforcement. It is necessary for parents to understand the aims and reasons for the treatment, perceive an element of urgency, and be aware of the seriousness of the condition (issues relating to the Health Belief Model variables11) in order for the decision to be made that the positive benefits outweigh the negative difficulties of having to implement the treatment. Unlike behavioural techniques, which are often impractical for use on large numbers of people, written information is simple to produce, easy and inexpensive to implement, yet a highly effective method of increasing concordance.
Acknowledgments
Orthoptic colleagues for advice and help in undertaking the study at Southport and Ormskirk (NHS) Trust and St Helens Hospital/Community (NHS) Trust.
REFERENCES
Linked Articles
- BJO at a glance