Article Text

Abstract
Aims: To assess the aetiological factors associated with the occurrence of perforating ocular injuries in children in an urban setting and to assess the visual outcomes of such injuries.
Methods: All cases of perforating ocular injury presenting to a single paediatric hospital (age less than 16 years) over a 17 year period were identified by a medical record search. All new cases of perforating ocular injury identified were included. All information was obtained retrospectively from the medical records.
Results: There were 72 cases identified. The commonest causes of perforating ocular injury were sharp tools (knives/scissors) poked by the child into his/her own eye (17%), or objects thrown at the child (17%). Injuries were most likely to have occurred at home (58%). The age range for injuries was 8 months to 14 years 8 months. Perforating ocular injury was most frequent in the 3–6 year group (32%) followed by the 6–9 year group (25%). Males were more frequently involved than females (48–24). There was no correlation between the laterality of the eye, the time of day of the occurrence, or the day of the week of the occurrence. The final acuity achieved was better or equal to 6/12 in 36% and less than 6/60 in 31%. Injuries occurred more frequently on weekends than on weekdays. There were six enucleations (8%). Follow up was for an average period of 25 months.
Conclusions: Penetrating ocular injury occurs most frequently in the home setting and mostly as the result of the use of sharp tools or by thrown objects. Prevention of penetrating ocular injury requires greater education of children and their carers especially on the potential dangers within the home.
- perforating ocular injury
- aetiology
- trauma
- children
Statistics from Altmetric.com
Perforating ocular injuries are a frequent cause of unilateral visual loss. Children account for between 20% and 50% of all ocular injuries.1–3 It has been estimated that 90% of all ocular injury are preventable.4 Strategies for prevention require a knowledge of the cause of injury and may hence enable more appropriate targeting of resources towards prevention of such injuries. The aetiology of paediatric ocular injuries is likely to differ from that of adults, and is hence worthy of further investigation.
The principles of management of penetrating ocular injury are the same for children and adults. However, the management of the child is made more difficult by variable cooperation with both assessment and continuing therapy. The possibility of amblyopia in young children further complicates treatment.
This study addresses the epidemiology of penetrating ocular injury in children presenting to a single institution in a metropolitan centre. It also reviews the outcomes of these injuries.
METHODS
All cases of full thickness perforating ocular injury presenting initially to the Royal Alexandria Hospital for Children in Sydney, Australia, between 1 January 1983 and 31 December 1999 were identified by a medical record search for the ICD code 871. Royal Alexandria Hospital for Children is a paediatric hospital (age 0–16 years) and is a tertiary referral centre. Patients who were initially repaired at other hospitals were excluded as were partial thickness lacerations. Cases were only identified if they were admitted to hospital, though it was assumed this would have included all cases. Patient records were reviewed to determine age, sex, day and time of injury, place of injury, cause, site and nature of injury, operations performed, complications, and final visual acuity.
RESULTS
For statistical analysis, 95% confidence intervals were calculated to indicate precision around percentages and to estimate statistical significance from expected frequencies.
A total of 72 cases of perforating ocular injury were identified. Follow up was for an average of 2.1 years. The age range of injuries was 7 months to 14 years 8 months. Injuries were more frequent in the 3–6 year age group and 6–9 year age group. Males were affected in 67%. This is statistically significant when compared to an assumed equal sex distribution in the young population (95% CI 55% to 77%). When injuries were categorised by age and sex there was an almost equal number of injuries for males and females in the less than 3 years age group and a male predominance of injuries in all other age groups (95% CI 58% to 83%) (Fig 1).

Age and sex at time of perforating ocular injury.
Mechanisms of injury were categorised into groups where two or more similar causes were identified (Table 1). The commonest types of injury were from sharp tools being poked by the child into his/her own eye or from objects thrown at the child. A typical example of the former injury was a child cutting rope with a knife towards him/her and on cutting the knife has followed through into his/her eye. Thrown objects included a variety of objects such as stones, metal objects, sticks, and glass. Falls occurred onto sharp objects such as table corners and bedside furniture. The group “hit with sharp tools” included several sticks poked into the eye, a knife, and sharp pieces of plastic or metal. Miscellaneous causes are listed in Table 2.
Grouped causes of perforating ocular injury
Miscellaneous causes of perforating ocular injury
The place of occurrence of injury is shown in Table 3. The commonest location for a perforating ocular injury to occur was in the home (58%). Injuries at school were infrequent (1%). Insufficient data were available to determine the location of injury in 22%.
Place of injury
The right eye was involved in 54%. This was not statistically significant (95% CI 42% to 66%). Wounds were predominantly involving the cornea only (58%) or were corneoscleral (29%). Wounds involving the sclera alone accounted for 13%. The lens was involved in 42%. There was uveal prolapse in 68%. The wound was less than 5 mm in length in 38%, 5–10 mm in 33%, and more than 10 mm in 24%. There were insufficient data for recording in 5%.
The time of injury occurrence was grouped into 2 hour periods from 8 am. There was a trend towards more injuries occurring between 4 and 6 pm with 12 of the 48 cases, where the time of injury was recorded occurring during this period but this was not statistically significant. Injury occurrence by month showed no specific seasonal trend. Saturday was the most frequent day for injuries to occur (16 cases). Weekends accounted for 30 injuries, weekdays for 42. Mondays and Fridays accounted for a greater number of injuries than mid-week. None of these trends reached statistical significance.
There was little correlation with school holidays, with only 18 cases occurred during the holidays and, of these, 11 occurred at a weekend. School holidays account for 20% of the year. Of the injuries 25% occurred during school holidays. This was not statistically significant.
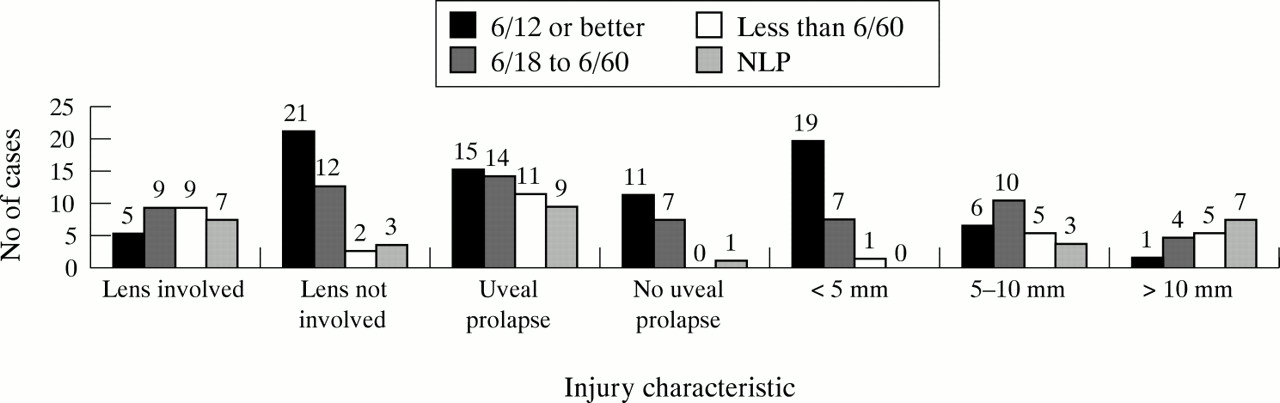
The overall outcome showed 36% attained visual acuities of 6/12 or better. However, 31% had acuities of worse than 6/60 (Fig 2). Final acuity showed a trend, but not statistically significant variation towards better acuity in cases where the lens was not involved, there was no uveal prolapse and the wound sizes were smaller. These features are shown in Figure 3.
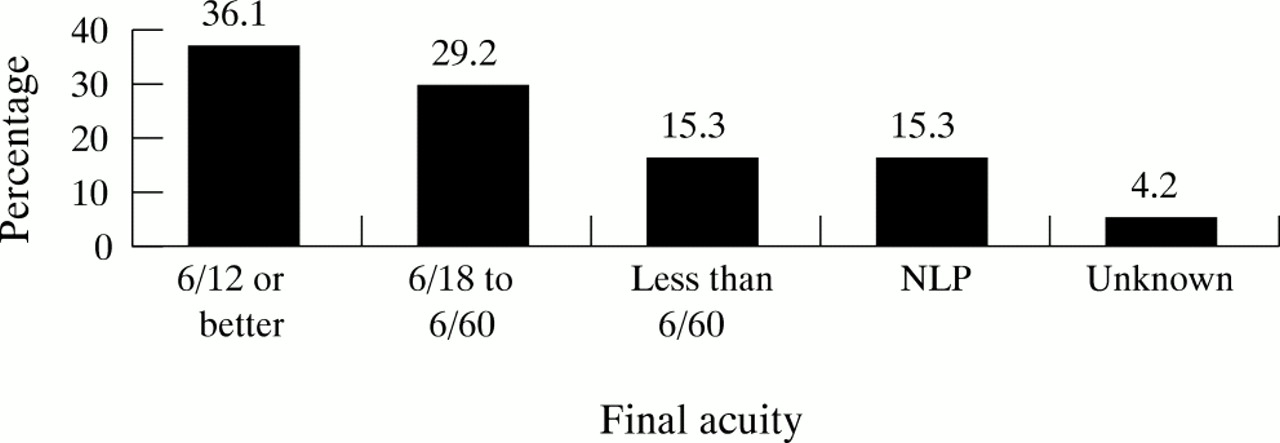
Acuity outcome.
{kind=link}
{kind=link}
{kind=link}
Acuity outcome correlated with lens involvement, uveal prolapse, and wound size.
Two wounds were self sealing and required no initial surgery but both patients went on to have a delayed cataract extraction, and one developed endophthalmitis. Primary lens removal was performed in eight cases, secondary removal in 12 cases. Primary enucleation or evisceration was performed in three cases and secondary enucleation or evisceration in three cases. Owing to the age of the population group the majority of suture removals were performed under a general anaesthetic and an examination under a general anaesthetic of the eye would have been performed at these times. The further procedures that were performed are detailed in Table 4. The following complications were encountered. There was one case of a suture abscess, which settled with suture removal and topical antibiotics. There were no cases of sympathetic ophthalmia. There was one case of fungal endophthalmitis which occurred in a self sealing perforation with plant material. This case developed an intralenticular abscess which failed to settle with topical antibiotics or antifungals. A vitreous tap grew Aspergillus. It settled with intravitreal antifungals and lensectomy. There was one case of infective keratitis which settled with topical antibiotics. Five patients developed retinal detachments which were repaired.
Re-operations
DISCUSSION
Perforating eye injuries represent a significant cause of visual loss. Ocular injuries have been estimated to cost the Australian community $155 million a year with 44% of this cost due to perforating injuries.5
There are only two large recent studies of the aetiology of perforating eye injuries in children (Soylu et al, 242 cases6 Moreira et al, 1463),and two smaller studies (Rudd et al, 46 cases7, Alfaro et al, 30 cases8). These studies were carried out in Turkey,6 Brazil,3 and the United States.7,8 With 72 cases this study is mid-size and in a different country.
The male preponderance of injuries in this study of exactly two to one is less than the findings of previous studies of between three to one and six to one.3,7–9 This difference may relate to different age profiles for these studies of children. The male predominance of injuries may be a result of males and females being engaged in different activities with different degrees of risk of ocular injury. Younger children tend to perform more similar activities and this could explain the equal incidence of injuries in the less than 3 year age group. Similarly Soylu et al6 found that during the early years of life there is no difference in occurrence of perforating ocular injury in boys and girls engaged in unsupervised play.
The high incidence of accidents occurring in the home is clearly of concern. Obviously, children spend a majority of their time at home and hence accidents are more likely to occur there. However, they also spend approximately 10–15% of their waking hours when under the age of 16 in school. Average commencing school age in New South Wales is 5 years and 55% of the children in this study were over this age. Only 1% of injuries occurred at school which suggests there is greater safety in being at school. Also only one of the injuries occurred in childcare. This may suggest that in schools and childcare centres the level of supervision may be greater. Also more careful attention may have been given to the activities conducted and the design of the environment and the availability of dangerous objects.
Although not statistically significant there was a slight predominance of right side injuries. Of the self inflicted injuries 10 involved the right eye and only two the left. These injuries generally occurred while the children were cutting towards themselves. If the children were right handed, which is commoner in the community, right side injuries would be expected to predominate. This may explain the predominance of right sided injuries. If the self inflicted injuries were excluded there would have only been 29 right eye injuries and 31 left eye injuries.
The incidence of injuries from motor vehicle accidents (6%) is similar to other recent studies1,7,10 but lower than in earlier studies.11 The reduction in perforating ocular injuries from the introduction of compulsory seat belt legislation has been well documented12 and is an excellent example of preventative public health measures.
In this study 36% of the children achieved 6/12 or better. Comparisons with other studies are complicated by different age profiles and differing injury profiles. Other paediatric studies reported achieving 6/12 or better in 43% (Alfaro et al),8 46% (Moreira et al),3 and 51% (Elder).13 The trend of these studies would seem to show a worse outcome in paediatric studies than for total or adult population studies (Thompson et al, 61%,14 Esmaeli et al, 50%,15 and Patel et al, 52.2%16). This may reflect the additional problems caused by amblyopia, difficulties in follow up and examining the child, effect of the management, and outcome of paediatric perforating ocular injuries.
As prevention of perforating ocular injuries is clearly the goal it is clear greater attention needs to be directed towards the potential dangers of the home surroundings. Owing to the relatively infrequent incidence of injury in any specific environment eye protection devices are unlikely to be instigated in most of these cases. The majority of injuries occurred in younger children who cannot be fully responsible for their actions; hence, parents and carers need education in preparing the home environment to be safe for children. Adequate supervision and appropriate ocular protection for children must be stressed especially when using sharp tools or scissors or knives. Safer tools such as blunt nosed scissors should be provided and access to sharp or dangerous household utensils should be restricted. Furniture with rounded corners is a more desirable choice for households with children. Plants with thorns are not suitable in gardens with children. Attention should also be directed towards the education of children in the avoidance of potentially dangerous activities. Games involving throwing projectiles should be disallowed. Children playing with pets require supervision and education on how to treat pets. Possible avenues of dissemination of this information would be through schools, medical practices and baby health clinics, and through the media.
Acknowledgments
Thanks to Jennifer Peat, Statistician, Royal Alexandria Hospital for Children, for statistical advice.