Article Text

Abstract
Aim: Choroidal perfusion, affected in age related macular degeneration (AMD), is difficult to objectively assess given the overlying retinal circulation. This study more objectively compared choroidal perfusion parameters in a group with non-neovascular AMD to an unaffected age matched control group.
Methods: 21 non-neovascular AMD subjects and 21 age matched control subjects without evidence of AMD underwent assessment of their choroidal blood flow in a case-control study. Scanning laser ophthalmoscope indocyanine green (ICG) angiograms were analysed by a new area dilution analysis technique. Four areas in the perifoveal region and two areas in the temporal peripapillary retina were evaluated by producing a graph of intensity of fluorescence of each area over time. The mean of the filling times and the heterogeneity of the filling times were assessed.
Results: The means of the filling times within the perifoveal regions and the hetereogeneity of the filling times between regions within the same eyes were significantly greater in the AMD patients compared with the control subjects.
Conclusions: Delayed and heterogeneous filling of the choroid was objectively demonstrated in eyes with non-neovascular AMD compared with age matched controls without evidence of AMD, using an area dilution analysis technique applied to ICG angiography.
- choroidal perfusion perturbations
- age related macular degeneration
Statistics from Altmetric.com
The pathogenesis of age related macular degeneration (AMD), the leading cause of irreversible visual loss in the United States, remains elusive. Abnormalities in the choroidal circulation have been previously described using fluorescein angiography,1–6 laser Doppler flowmetry,7 colour Doppler imaging,8,9 and indocyanine green (ICG) angiography,10–12 but it is not possible to determine if these blood flow abnormalities are causative or the result of AMD.13 Clinical study of this relation is complicated by the heterogeneous nature of this disease. Furthermore, it is very difficult to quantify choroidal blood flow angiographically given the overlying retinal circulation, which complicates analysis. In this current study, a new analysis technique was applied to ICG to objectively evaluate choroidal perfusion in subjects with non-neovascular AMD compared with subjects with normal eyes.
METHODS
Study subjects
Study subjects were recruited from a university based referral retina practice over a 6 month period. Consecutive patients who met the inclusion and exclusion criteria were asked to participate. Subjects were deemed eligible for inclusion into the AMD population if their study eye showed non-neovascular macular degeneration, defined according to the International Classification System as a degenerative disorder in patients greater than 50 years of age with “soft drusen greater than 63 microns, hyperpigmentation and/or hypopigmentation of the RPE, . . . or geographic atrophy of the RPE.”14 In those study subjects who showed non-neovascular AMD in both eyes, the eye with the better level of corrected visual acuity was chosen as the study eye in order to maximise fixation behaviour and minimise corrections for eye movements during angiographic image analysis described below. Subjects were excluded if both eyes showed neovascular AMD, defined according to the International Classification System as the presence of “RPE and associated neurosensory retinal detachment, (peri)retinal hemorrhages, or (peri)retinal fibrosis on masked analysis of fundus photos or evidence of choroidal neovascularization (CNVM) on fluorescein angiography.”14 Red free videophotography and fluorescein scanning laser ophthalmoscopy/angiography were performed before study entry on all subjects to rule out evidence of CNVM in the study eye.
Control subjects were also recruited over the same 6 month period from a university based referral retina practice. Consecutive subjects who met the inclusion and exclusion criteria were asked to participate. They were excluded if they showed evidence of either non-neovascular or neovascular AMD in either eye as defined above. Red free videophotography and fluorescein scanning laser ophthalmoscopy/angiography were performed before study entry on these subjects as well to confirm absence of non-neovascular or neovascular AMD in either eye. Inclusion and exclusion criteria were monitored by assessment of stereoscopic fundus photographs, red free videoangiography, and fluorescein scanning laser angiography. These assessments were performed by a retinal specialist masked to the subjects' identity and masked to the results of the choroidal blood flow analysis.
Both control and study subjects were deemed ineligible if they had a history of diabetic retinopathy, ophthalmic or retinal artery occlusion, retinal vein occlusions, hypertensive retinopathy or choroidopathy, or known history of significant carotid stenosis. Additional exclusion criteria for both study and control subjects included glaucoma, optic neuropathy, macular dystrophies, ocular inflammatory disease, retinal detachment, or media opacity sufficient to preclude examination and follow up. In addition, subjects were excluded if they were unable to give informed consent, or had a history of allergy to fluorescein, radiographic dyes, shellfish, or iodine. Subjects who did not meet the inclusion and exclusion criteria did not participate in this study.
Subjects were asked to sign an informed consent before undergoing ICG angiography and study participation. The institutional review board of the Indiana University School of Medicine approved all protocols.
Ophthalmic evaluations
In all subjects, intraocular pressure was measured by Goldmann tonometry. Systemic blood pressure was measured by sphygmomanometry. Ocular perfusion pressure (OPP) was calculated from these two measurements as: OPP = 2/3 mean arterial pressure − IOP. Mean arterial pressure (MAP) is calculated as MAP = diastolic blood pressure + 1/3 (systolic − diastolic blood pressure). Severity of the non-neovascular AMD in all subjects fulfilling the inclusion and exclusion criteria was estimated to the nearest 5% from stereoscopic fundus photographs based on percent macular area (within 3000 μm from the fovea) occupied by RPE mottling, drusen, or geographic atrophy. These assessments were also performed by a retinal specialist masked to the subjects' identity and masked to the results of the choroidal blood flow analysis.
ICG angiography
ICG angiography was performed on the scanning laser ophthalmoscope (Rodenstock SLO 101). Red free images were first obtained with a 488 nm argon laser at 40° to locate the macula relative to the optic disc. The argon laser was shut down, and a 795 nm near infrared laser was used to perform the angiogram. The ICG was prepared by dissolving 25 mg of ICG into 2 ml of solvent (instead of the typical 10 ml) and 1 ml of this solution was then injected per examination. The small volume of dye allows a rapid injection time of approximately 1 second. The injection was immediately followed by a 2 ml saline flush. Verbal commands were used to guide subject fixation so that the nasal edge of the disc was at the edge of the video frame centred vertically, the macula toward the centre of the screen. The examination was recorded on S-VHS videotape, digitised, and processed offline, as detailed below.
Analysis
An investigator masked to the subjects' assignment to the AMD or control population performed area dilution analysis (ADA) on the digitised ICG angiograms using an HRX digital image processor (Amtronics, New Orleans, LA, USA) with customised software. Area dilution analysis has been described in detail in the literature.15 Six locations, each a 6° square, on the image were identified for analysis (Fig 2). Four areas around the fovea and two areas in the temporal peripapillary retinal area were evaluated. After correcting for eye movements, the average brightness of the area contained in each box was computed for each frame of the angiogram. Area brightness was graphically determined with time on the X axis and brightness on the Y axis (Fig 3). Since the exact concentration of ICG in each region cannot be determined, the single brightest area of any frame was set to a value of 1 in order to normalise the curves for intersubject comparison; this would also correct for differences in uveal and RPE pigmentation between individuals, which could potentially influence brightness.
Intensity curves were analysed by quantifying the dye arrival times (amount of time required to rise to 10% and 63% above baseline) and the slope of the filling portion of the curves (Fig 3). The dye dilution curve reaches 10% brightness some time before reaching 63% brightness, and the 10% filling consequently reflects earlier choroidal filling. In addition, the 10% time contains a larger systemic component in which the time from injection to appearance in the choroid makes up a large portion of the measurement. The 63% filling time contains a larger representation of the time that the dye spends moving through the choroid. The slope correlates with the speed of blood entrance into the choroid. Each of these haemodynamic parameters can be evaluated by performing individual area analysis, mean analysis of the four perifoveal or six total areas, and analysis of the regional spread (maximum minus minimum) to determine haemodynamic homogeneity.
Statistical analysis
Two tailed unpaired t tests and χ2 tests were used to compare demographic and haemodynamic parameters between the AMD and normal groups. Non-parametric comparison with Mann-Whitney U test was used to compare haemodynamic parameters between the sex groups in the normal and AMD groups.
RESULTS
Twenty one AMD and 21 control subjects were evaluated. Table 1 summarises their demographics. Three of the 21 AMD subjects showed neovascular AMD in the fellow eye. There were no statistically significant differences in any of the perfusion characteristics in the study eyes between these subpopulations. However, additional subjects would be required to generate sufficient power to more fully explore this issue in the future, as this current study was not designed to address this issue. There was a statistically significant difference in sex between the groups (p=0.0278); however, when the results of the area dilution analysis were compared between sexes separately within the AMD and control groups, there was no difference in test results between sex groups (p>0.05, Mann-Whitney U test). Also shown in Table 1 is a statistically significant difference in mean systolic blood pressure, but there was no statistically significant difference in the diastolic blood pressure or the ocular perfusion pressure.
Demographics
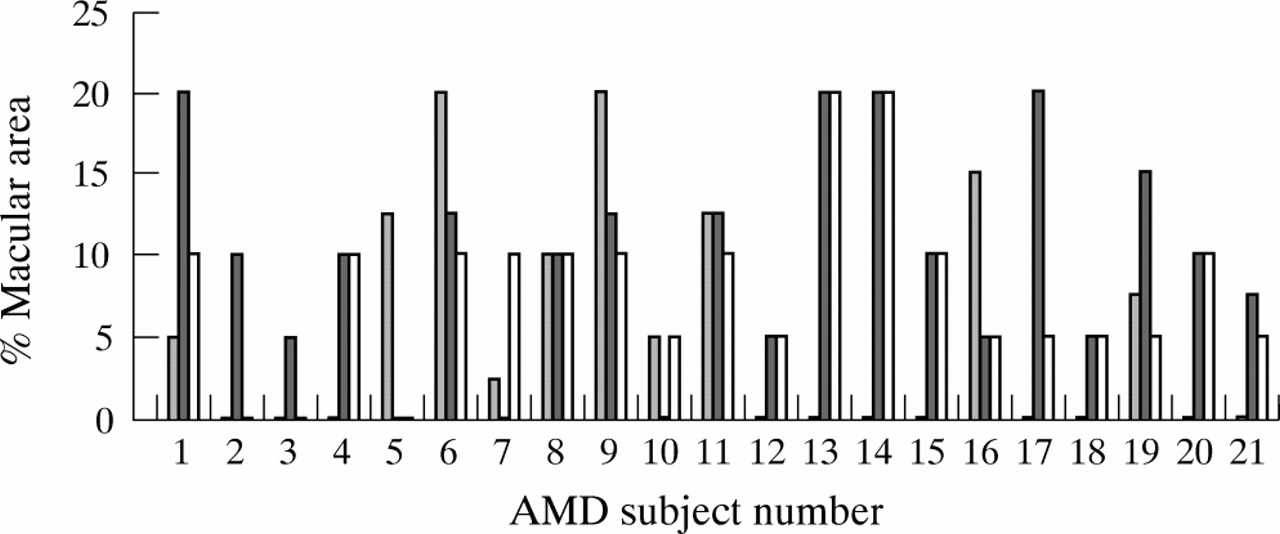
As noted above, severity of the non-neovascular AMD in all subjects was determined in a masked fashion from fundus photographs based on estimated percentage macular area (within 3000 μm, from the fovea) occupied by RPE mottling, drusen, or geographic atrophy. The distribution of these macular findings is presented in Figure 1. No subject showed a severity score of greater than 20%.

Macular findings in the AMD subjects. Severity of the non-neovascular AMD in all subjects fulfilling the inclusion and exclusion criteria was estimated to the nearest 5% in a masked fashion from stereoscopic fundus photographs based on percentage macular area (within 3000 μm from the fovea) occupied by RPE atrophy, drusen, and RPE mottling. The distribution of these macular findings (RPE atrophy, drusen, and RPE mottling: first, second, and third bar respectively) is presented for each of the 21 AMD subjects.
The area dilution analysis data are summarised in Table 2. The spread of 10% filling times (1.81 (SD 1.10) v 0.85 (0.42) seconds, p=0.0006) was greater in AMD patients than in normal subjects for the four perifoveal regions. Similarly, the mean of 63% filling time (30.15 (9.32) v 24.83 (3.87) seconds, p=0.0202) and the spread of 63% filling time (1.86 (1.05) v 0.93 (0.60) seconds, p=0.0010) was greater in AMD patients than in normal subjects for the four perifoveal regions and these results were highly statistically significant. Unlike the results from the 10% filling times, these results from the 63% filling times remain statistically significant when the two peripapillary areas are included in the analysis.
Area dilution analysis (mean (SD))
As noted above, the 10% time contains a larger systemic component in which the time from injection to appearance in the choroid makes up a large portion of the measurement. The 63% filling time contains a larger representation of the time that the dye spends moving through the choroid. If the dye is moving slowly through the choroidal vasculature due to sluggish choroidal haemodynamics, the slope of the filling curve will be shallow and slow, and the 63% time will be significantly delayed from the 10% time. If the dye moves rapidly through the choroid then the slope will be steep and the filling times will be similar. The 63% filling time is consequently more sensitive than the 10% filling time with regard to choroidal haemodynamics; the differences in the results between the 10% and 63% filling times is consequently not unexpected. It should also be noted that the regional spread (maximum minus minimum) reflects haemodynamic homogeneity within one eye and not between subjects. Consequently, the statistically significant results with respect to regional spread do not originate from differences in AMD manifestations between subjects. Rather, there is increased haemodynamic heterogeneity between the analysed regions of the choroid in an AMD subject compared with a control subject. These filling time results taken together imply slower and more heterogeneous filling of the choroid in AMD patients compared with control subjects.
As noted above, the slope of the filling portion of the curves is indicative of the speed with which the ICG enters the choroid. The analysis showed that the mean slope of the filling portion of the curve (0.084 (0.031) v 0.104 (0.018), p = 0.0136) was slightly lower in the AMD patients than in normal subjects for the four perifoveal regions, but when the two peripapillary regions were included in the analysis, the differences were not statistically significant. These results are consistent with the implications from the filling time analysis. These results also suggest that the differences are most pronounced in the perifoveal region. Analysis of the duration of the fluorescence in the AMD patients compared to the normal subjects revealed no significant difference.
DISCUSSION
In this current study, a new analysis technique was applied to ICG angiography to more objectively evaluate choroidal perfusion in subjects with non-neovascular AMD compared with subjects with normal eyes. These techniques have been previously described.15 In brief, the entire 40 degree ICG angiogram is divided into a number of small regions (Fig 2) and dilution curves (Fig 3) are created for each region. Although the exact concentration of ICG in each region cannot be determined, simultaneous acquisition of dye dilution curves from these regions within the choroid facilitates comparison of relative concentrations between these regions and allows for assessment of the various timing parameters. Since the six analysis regions are identically positioned on each subject's angiogram, the resulting analysis represents an objective evaluation of choroidal perfusion characteristics and does not rely on subjective assessment. In addition, ICG facilitates study of the choroidal circulation for several reasons. Firstly, ICG better delineates the choroidal circulation than fluorescein because the near infrared light absorbed by ICG penetrates the retina pigment epithelium better than the shorter wavelength absorbed by fluorescein. Also, unlike fluorescein, ICG is strongly bound to plasma proteins, which prevents diffusion of the compound through the fenestrated choroidal capillaries, and permits better delineation of choroidal details. The use of scanning laser ophthalmoscopy for ICG angiography further improves the technique as the confocal design eliminates scattered and reflected light, while the single spot laser illumination improves contrast.

Indocyanine green angiography analysis areas. A 40 degree indocyanine green choroidal angiogram using scanning laser ophthalmoscopy. Six locations, each a 6° square, on the image are identified for area dilution analysis. A and D correspond to the peripapillary regions, while B, C, E, and F correspond to the perifoveal regions.

{kind=link}
{kind=link}
{kind=link}
Dye dilution curves. Haemodynamic parameters in area dilution analysis of indocyanine green choroidal angiography using scanning laser ophthalmoscopy. Area dye dilution analysis identifies five parameters from the brightness maps: 10% filling time, 63% filling time, the slope of each curve, the duration of the each curve, and the maximum intensity of brightness. The 10% and 63% filling time (seconds) is the amount of time required to reach a brightness 10% and 63% above baseline. The slope (arbitrary unit: intensity/s) is calculated by dividing the intensity change by the time lapsed between 25% and 75%. The duration (seconds) is the time between 75% in the ascending and descending curves.
In the current study, subjects with non-neovascular AMD showed significant delay and heterogeneity of filling within the perifoveal region of non-neovascular AMD patients when compared with normal age matched controls. As noted above, the haemodynamic heterogeneity is measured within each eye and not between subjects; consequently, this statistically significant result does not originate from differences in AMD manifestations between subjects, but from increased haemodynamic heterogeneity between the analysed regions of the choroid in an AMD subject compared with a control subject. These differences were most pronounced in the perifoveal regions, suggesting that the choroidal perfusion anomalies in non-neovascular AMD show some preferential involvement of the perifoveal choroid. The pathophysiological basis for this perifoveal change is unclear; it is intriguing that the other changes observed in AMD (drusen, RPE mottling, choroidal neovascularisation, etc) also preferentially present in the macula instead of extramacularly. Although the subjects in this study were not sex matched, sex differences between the groups are unlikely to account for the results, because there was no difference between sex groups when the results of the area dilution analysis were compared between sexes within each of the AMD and control groups. Likewise, it is unlikely that the differences in systolic blood pressures between the groups account for the results since there was no significant difference in ocular perfusion pressure between the groups. Compared to blood pressure, ocular perfusion pressure (2/3 mean arterial pressure − IOP) is believed to more accurate reflect the vascular inflow to the eye since it accounts for the intraocular pressure; consequently this parameter is commonly used for assessing ocular perfusion in ocular blood flow studies.16–18 Furthermore, these results were not unexpected and very consistent with previous studies, which have suggested very similar choroidal perfusion abnormalities in AMD using conventional angiographic techniques.
In particular, this study corroborates and amplifies results from previous studies using fluorescein angiography,1–6 laser Doppler flowmetry,7 colour Doppler imaging,8,9 and ICG angiography,12 For example, delayed choroidal filling has been noted angiographically in patients with neovascular AMD.1–3 The use of fluorescein angiography to study the choroidal circulation has several limitations that include leakage of fluorescein from the choroidal circulation, and the overlying retinal circulation that complicates analysis. Nevertheless, the results obtained in the current study are consistent with these previous fluorescein angiographic studies. One group recently used laser Doppler flowmetry in subjects with non-neovascular AMD to show that the choroidal blood flow was decreased at the centre of the fovea compared to a control group.7 This technique cannot be readily applied outside the foveal centre as the overlying retinal circulation would Doppler shift the reflected light from the laser and prevent analysis of the choroid. This study and the current study, however, are complementary; this earlier study showed alterations in choroidal flow in the foveal centre and current study confirmed alterations with some perifoveal region specificity, although the foveal centre itself was not measured. Colour Doppler imaging has been used to evaluate the retrobulbar vasculature in AMD; two groups have found statistically significant differences in the central retinal and posterior ciliary arteries in patients with AMD compared to controls.8,9 This technique, however, assays the retrobulbar vessels and consequently better correlates with bulk flow to the choroid (posterior ciliary arteries) and to the retina (central retinal artery) without any macular region specificity. Bischoff and Flower were first to demonstrate that the ICG angiograms of AMD cases were abnormal,10 and Prunte and Niesel were first to subject ICG angiograms from AMD patients to quantitative analysis, using parameters such as the mean time for arterial, capillary and venous filling and a parameter corresponding to the amount of perfused capillaries in the choroid.11 Another group more recently used a new analysis technique based on indocyanine green angiography to compare the choroidal circulation in patients with AMD to a control group, and noted a statistically significant increased frequency of presumed macular watershed filling, which they described as “characteristic vertical, angled, or stellate-shaped zones of early-phase indocyanine green videoangiographic hypofluorescence, assumed to be hypoperfusion, which disappeared in the early phase of the angiogram.”12 This technique, however, requires subjective interpretation and cannot provide quantitative analysis of choroidal filling parameters. In addition, this study included a heterogeneous population of both neovascular and non-neovascular AMD patients.
In summary, the current study objectively demonstrates delayed and heterogeneous filling of the choroid in patients with non-neovascular AMD with some perifoveal region specificity. These results corroborate and amplify the work of previous authors as detailed above. Future studies using this technique should be designed to fully compare perfusion characteristics in subjects with bilateral non-neovascular AMD to subjects with unilateral neovascular AMD in the fellow eye. Assessing perfusion differences between these bilateral non-neovascular and unilateral neovascular forms would be of interest in the future since the underlying pathophysiology may differ between these populations. For example, it is unclear if the choroidal perfusion defects demonstrated in non-neovascular AMD lead to localised choroidal ischaemia and a subsequent neovascular response. Finally, it should be noted that it is not possible to determine if the choroidal perfusion abnormalities has a causative role in non-neovascular AMD, if they are simply an association with, or result of, another primary alteration. Much further study is warranted, given the prevalence of AMD, the limited understanding of its pathophysiology, the devastating consequences, and the lack of effective treatment.
Acknowledgments
Supported in part by grants from the Indiana Lions' Club; an unrestricted grant from Research to Prevent Blindness, Inc, New York, and NIH grant EY10801. Dr Ciulla is a recipient of a career development grant from Research to Prevent Blindness, Inc. Dr Harris is a recipient of the Research to Prevent Blindness international scholar award.