Article Text

Abstract
Aim: To evaluate the effect of intravitreal triamcinolone acetonide on the visual acuity of patients with exudative age related macular degeneration, to assess the duration of a possible effect, and to evaluate clinical side effects of the treatment.
Methods: The study included 67 patients (71 eyes) who presented with exudative age related macular degeneration of predominantly or total occult type (n = 68) or classic type (n = 3), and who received once, or repeatedly, an intravitreal injection of 25 mg of crystalline triamcinolone acetonide. Mean follow up time was 7.46 (SD 3.54) months (range 3.1–19.57 months).
Results: Visual acuity increased significantly (p <0.001) from 0.16 (0.11) to a mean maximum of 0.23 (0.17). Postoperative visual acuity was highest 1–3 months after the injection. 47 (66.2%) eyes gained in maximal visual acuity and 11 (15.5%) eyes lost in visual acuity. Intraocular pressure increased significantly (p <0.001) from 15.1 (3.1) mm Hg at baseline to a maximal value of 23.0 (8.25) mm Hg. At the end of follow up, intraocular pressure again decreased significantly (p<0.001) to 16.8 (4.9) mm Hg. No cases of postoperative infectious endophthalmitis, rhegmatogenous retinal detachment, or proliferative vitreoretinopathy occurred. Owing to a decrease in visual acuity after an initial increase, six patients received a second intravitreal triamcinolone acetonide injection after which visual acuity increased again in three eyes.
Conclusions: Intravitreal injection of 25 mg of crystalline triamcinolone acetonide merits further study for the treatment of exudative age related macular degeneration.
- age related macular degeneration
- triamcinolone acetonide
- intraocular pressure
- steroid response
Statistics from Altmetric.com
Exudative age related macular degeneration is one of the most frequent reasons for marked loss of vision, and consequently, for legal blindness, in the elderly population of Western countries.1–3 Ocular photodynamic therapy with verteporfin has been demonstrated to reduce vision loss in patients with predominantly classic type of exudative age related macular degeneration.4–6 For the predominantly occult type, however, none of the currently available treatments have been shown to be markedly effective in reducing the loss of vision.
Intravitreal triamcinolone acetonide has increasingly been used in pilot studies for treatment of intraocular proliferative, oedematous, and neovascular diseases, such as long standing macular oedema due to central retinal vein occlusion,7,8 diffuse diabetic macular oedema,9,10 proliferative diabetic retinopathy,11 neovascular glaucoma,12 proliferative vitreoretinopathy,13 chronic pre-phthisical ocular hypotony,14 chronic uveitis,15–19 persistent pseudophakic cystoid macular oedema, and other clinical conditions.20,21 In aqueous humour and in silicone oil, triamcinolone acetonide has been found up to 6 months and up to 8 months, respectively, after the intravitreal injection.22,23 Systemic or local side effects, besides a cataractogenic effect, infectious endophthalmitis, and secondary ocular hypertension leading in some patients to secondary chronic open angle glaucoma, have not been reported so far.24 In view of its potentially anti-oedematous and anti-angiogenic effects as suggested by the studies on macular oedema, neovascular glaucoma, and proliferative diabetic retinopathy,7–12 and based on the experiences gathered in previous studies on exudative age related macular degeneration by Penfold, Challa, Danis and colleagues,25–28 the purpose of the present study was to evaluate whether intravitreal triamcinolone acetonide may be helpful to stabilise or even to improve visual acuity in patients with neovascular age related macular degeneration. Secondary aims of the study were to assess the duration of a possible effect of intravitreal triamcinolone acetonide and to evaluate clinical side effects of the treatment.
PATIENTS AND METHODS
The prospective clinical interventional case series study included all 67 patients (71 eyes; 38 right eyes) who presented with neovascular age related macular degeneration, who received one or more than one intravitreal injection of 25 mg of triamcinolone acetonide, for whom follow up time was longer than 3 months, and who did not undergo cataract surgery in combination with the intravitreal injection. Exclusion criteria were classic type of exudative age related macular degeneration unless the patients were ineligible for photodynamic therapy, and previous therapy of neovascular age related macular degeneration by photodynamic therapy. History of glaucoma and history of intraocular surgery including cataract surgery or retinal or vitreoretinal surgery were not exclusion criteria. A subretinal haemorrhage should not have extended beyond the temporal vascular arcade. All patients were fully informed about the experimental character of the therapy. All patients signed an informed consent. The study was performed at a university hospital. The ethics committee of the university had approved the study following the tenets of the Declaration of Helsinki. All patients were to be re-examined at the first postoperative day, in the first postoperative week, and from then on at monthly intervals. Mean age of the patients was 77.72 (SD 7.21) years (median 77.6 years; range 60.1–100.1 years), mean refractive error was 0.38 (2.17) dioptres (median +0.50 dioptres; range −8.00 to +5.00 dioptres). For four patients, both eyes received an intravitreal injection of triamcinolone, with a time interval of 3.5–5 months between the injections.
Six patients received a second intravitreal injection of triamcinolone into the same eye with a mean time interval of 4.83 months (range 3.1–7.0 months) between the injections. One patient received a third injection 5.7 months after the second injection. All patients who received a second or third intravitreal injection had shown an improvement in visual acuity after the preceding injection, and an eventual deterioration 3–5 months after the injection.
Mean follow up time after the first injection was 7.46 (3.54) months (median 7.33 months; range 3.1–19.57 months) (n = 71). For the second injection, mean follow up time was 5.66 (1.73) months (median 5.38 months; range 3.93–8.90 months) (n = 6), and follow up time after the third injection was 5.7 months (n = 1).
Fluorescein angiogram performed for all patients showed an exudative age related macular degeneration with a subfoveal neovascularisation membrane. The membrane was totally or predominantly (>50%) occult in 68 (95.8%) eyes, and it was predominantly classic (>50%) or totally classic in three (4.2%) eyes. For the three patients with the classic type or with the mostly classic type of subfoveal neovascularisation, photodynamic therapy had been recommended but was refused by the patients for various reasons such as cost and immobility. According to the fluorescein angiogram, the whole study group was divided into a subgroup with classic or mostly classic type of subfoveal neovascularisation (n = 3; 4.2%), a subgroup with the occult or mostly occult type of subfoveal neovascularisation without subretinal haemorrhage (n = 59; 83.1%), a subgroup with subretinal haemorrhage (n = 7; 9.9%), and a subgroup with detachment of the retinal pigment epithelium (n = 2; 2.8%). All four subgroups did not vary significantly (p>0.10) in age, refractive error, duration of the follow up period, and preoperative visual acuity.
All patients complained about a loss of vision which had been documented by an ophthalmological examination within 3 months before the intravitreal injection (n = 16 eyes, loss of 0.10 or more of visual acuity), or which had been experienced earlier or had not been documented by an ophthalmological examination (n = 55 eyes). Mean visual acuity at baseline of the study was 0.16 (0.11) (Snellen charts) (median 0.20; range finger counting to 0.50) (Table 1) (Figs 1 and 2), mean intraocular pressure measured 15.1 (3.1) mm Hg (median 16 mm Hg; range 8–24 mm Hg). Twenty three (32.4%) eyes were pseudophakic. The remaining 48 eyes (67.6%) were phakic.
Visual acuity (mean (SD); median; range) after the first intravitreal injection of 25 mg triamcinolone acetonide; p value: significance of difference from the preoperative value
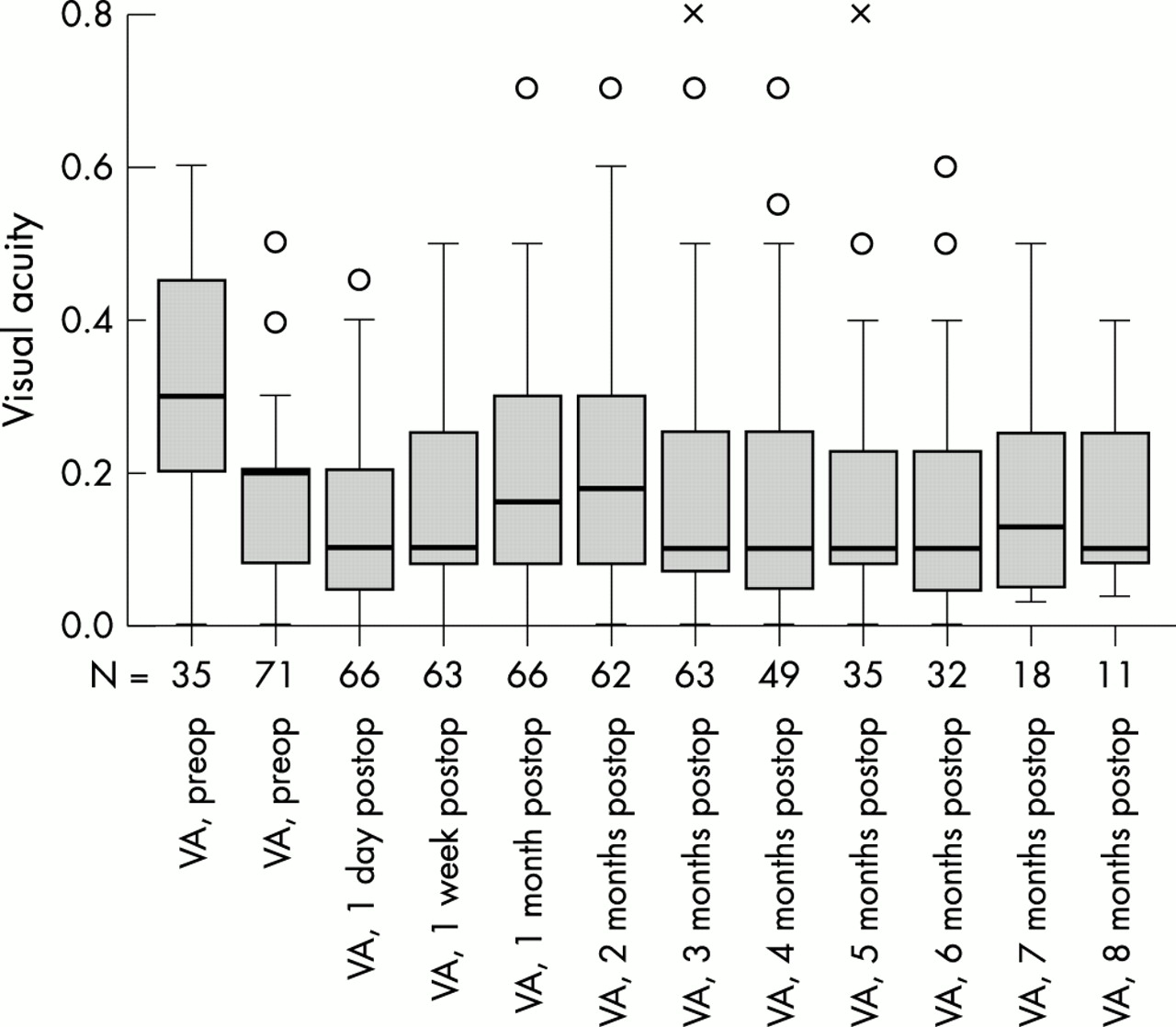
Box plots showing the visual acuity (VA) before and after the intravitreal injection of triamcinolone acetonide. Measurements in Snellen units.

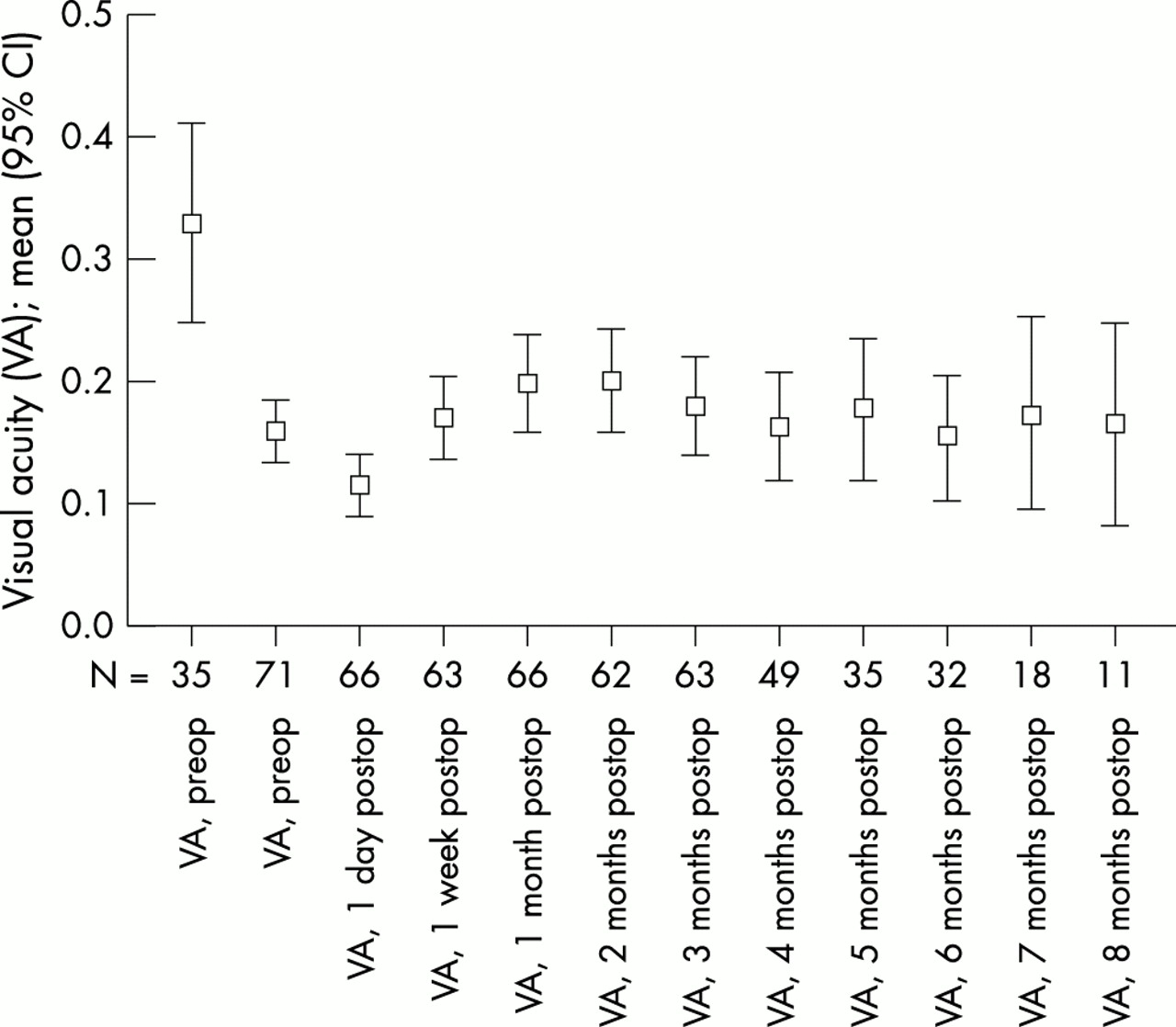
Graph showing the mean and confidence intervals (95%) of visual acuity (VA) before and after the intravitreal injection of triamcinolone acetonide. Measurements in Snellen units.
At baseline of the study and at repeated intervals afterwards, all patients underwent a routine ophthalmological examination including standardised visual acuity measurement using Snellen charts, slit lamp biomicroscopy, Goldmann applanation tonometry, and ophthalmoscopy. The examinations were routinely performed at the first day after the injection, 1 week after the injection, 1 month after the injection, and at monthly intervals from then on. Eight (11.3%) patients skipped one or two follow up examinations within the first 3 months after the injection and returned for a later re-examination (Table 1). For all patients included in the study, the results of at least one examination performed at least 3 months, or later, after the intravitreal injection were available. Upon slit lamp biomicroscopy, the degree of lens opacification in the subcapsular layer, the cortical layer, and the nuclear layer of the lens was graded using a subjective scale ranging from 0 for very clear lens to 5 for very pronounced opacification.
The intravitreal injection of triamcinolone acetonide was performed under sterile conditions in the operating theatre using an operating microscope. With topical anaesthesia, a paralimbal paracentesis was performed to puncture the anterior chamber and to reduce the intraocular volume. At a distance of 3.0–3.5 mm from the limbus, 25 mg triamcinolone acetonide in 0.2 ml of Ringer’s solution were transconjunctivally injected. The pharmacy prepared the solution free of solvent agents or other vehicles, to generally prevent any potentially toxic effect of a vehicle to intraocular tissues.29,30 Out of the original ampoule containing 40 mg of triamcinolone acetonide in 1 ml, the appropriate volume representing 25 mg of triamcinolone acetonide was taken, diluted in Ringer’s solution, and pressed through a Millipore filter. The triamcinolone crystals which, owing to their size, could not pass through the filter, were re-diluted in Ringer’s solution, and the whole procedure was repeated three times, finally resulting in a solution of 0.2 ml containing 25 mg of triamcinolone acetonide crystals.
A major difference between the studies on the intravitreal application of triamcinolone acetonide performed by others and the present investigation is the dosage of triamcinolone intravitreally injected. In most of the previous studies on intravitreal triamcinolone acetonide for cystoid macular oedema, diabetic macular oedema, and macular degeneration performed by other researchers, a dose of 4 mg of triamcinolone acetonide was used. Reasons why we used a dose of 25 mg of triamcinolone acetonide instead of 4 mg are that right from the beginning of our ongoing triamcinolone studies, now involving more than 300 patients with various diseases, we have used the same dose of 25 mg of triamcinolone acetonide, and we have not seen side effects so far that may be attributed to that high dosage.8,9,11–14,19,22–24 It also holds true for repeated intravitreal injections of 25 mg of triamcinolone acetonide.31 An additional reason was that in preceding studies on the intravitreal use of 4 mg of triamcinolone acetonide for patients with exudative age related macular degeneration, the therapeutic effect has not been quite clear.25–27
For statistical analysis, the non-parametric Wilcoxon test was used to compare the changes in visual acuity, intraocular pressure, and in the amount of cataract during the study period. To compare between the subgroups of the study, the Wilcoxon-Mann-Whitney test was applied.
RESULTS
Visual acuity
After the first injection, mean visual acuity increased significantly (p <0.001) from 0.16 (0.11) at baseline of the study to a maximum of 0.23 (0.17) (median, 0.20; range finger counting to 0.80) during the follow up period (Table 2) (Figs 1–3). The highest postoperative visual acuity was achieved 1–3 months after the injection (Figs 1–3). Comparing the visual acuity measurements at baseline of the study with the measurements obtained during the follow up period, the increase in visual acuity was statistically significant for the examinations performed 1 month (p = 0.04) and 2 months (p = 0.04) after the injection (Table 2). The preoperative visual acuity data and the visual acuity measurements obtained at the end of the follow up period did not differ significantly (p = 0.17). Compared with the peak of visual acuity measurements 1 and 2 months after the injection, visual acuity significantly decreased towards the end of the follow up period, parallel to a disappearance of the triamcinolone acetonide crystals out of the vitreous cavity.
Study population differentiated into subgroups according to the change in visual acuity

Diagram showing the individual course of visual acuity after the first intravitreal injection of triamcinolone acetonide for all eyes included in the study.
Comparing the preoperative visual acuity with the best postoperative visual acuity, 47 (66.2%) eyes gained in visual acuity and 11 (15.5%) eyes lost in visual acuity. Visual acuity was unchanged for 13 (18.3%) eyes. Nineteen (26.8%) eyes gained in visual acuity by more than 0.1. In 28 (39.4%) eyes, gain in visual acuity was equal to or less than 0.1. These three study subgroups did not vary significantly in age, refractive error, and duration of follow up period (Table 3). Preoperative visual acuity was significantly (p = 0.008) higher in the group with a higher gain than in the subgroup with a small gain in visual acuity (Table 3). The subgroup with a higher gain in preoperative visual acuity, however, did not differ significantly (p = 0.62) in visual acuity from the subgroup with no gain or loss in visual acuity. Correspondingly, taking the whole study group, preoperative visual acuity was not significantly correlated with the postoperative change in visual acuity.
Study population differentiated into subgroups according to the change in visual acuity
Dividing the whole study group into a subgroup with classic or mostly classic type of subfoveal neovascularisation, a subgroup with the occult or mostly occult type of subfoveal neovascularisation without subretinal haemorrhage, a subgroup with subretinal haemorrhage, and a subgroup with detachment of the retinal pigment epithelium, all four subgroups did not vary significantly (p >0.10) in gain in visual acuity.
Expressing the postoperative change in visual acuity in Snellen lines, 10 (17.5%) out of 63 eyes showed a loss of three lines or more after 3 months of follow up, and nine (14.3%) eyes showed an improvement of at least three lines (Fig 4). A loss in visual acuity of at least six lines after a follow up period of 3 months was found in one (1.6%) eye, and a gain of six lines was observed in one (1.6%) eye. After a follow up period of 6 months, nine (28.1%) out of 32 eyes showed a loss in visual acuity of at least three lines, and five (15.6%) eyes showed an increase in visual acuity by at least three lines (Fig 5). A loss in visual acuity of at least six lines after a follow up period of 6 months was found in one (3.1%) eye.

Histogram showing the distribution of the change in visual acuity 3 months after the intravitreal injection of 25 mg of triamcinolone acetonide.

Histogram showing the distribution of the change in visual acuity 6 months after the intravitreal injection of 25 mg of triamcinolone acetonide.
Taking into account the six eyes with a second injection, visual acuity increased in three (50%) eyes about 1 month after the re-injection, and declined again after about 3 months (Table 4) (Fig 6).
Visual acuity (mean (SD); median; range) after the second intravitreal injection of 25 mg triamcinolone acetonide

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagram showing the individual course of visual acuity after the second intravitreal injection of 25 mg of triamcinolone acetonide.
Intraocular pressure
Intraocular pressure increased significantly (p <0.001) from 15.1 (3.1) mm Hg at baseline of the study to a mean maximal value of 23.0 (8.25) mm Hg (median 21.0 mm Hg; range 13–64 mm Hg), and again decreased significantly (p <0.001) to 16.8 (4.9) mm Hg (median, 16 mm Hg; range 10–34 mm Hg) 7 months after the injection.
The intraocular pressure measurements taken at the end of the follow up period were slightly and significantly (p = 0.001) higher than the pressure measurements taken at baseline of the study. During the study period, intraocular pressure was higher than 21 mm Hg in 35 (49.3%) eyes. In all but one of these eyes, intraocular pressure could be normalised by topical antiglaucomatous medication. Glaucomatous damage of the optic nerve, or increase in pre-existing glaucomatous optic nerve atrophy, as determined by biomorphometry of the optic nerve head,32 was not detected. One eye with pre-existing primary open angle glaucoma before the intravitreal injection showed intraocular pressure measurements of higher than 60 mm Hg. This eye underwent standard penetrating filtering surgery after which intraocular pressure was normalised to values less than 21 mm Hg.
Cataract and other complications
The degree of cataract increased significantly (p <0.001) in all layers of the lens examined. The degree of subcapsular posterior cataract increased from 0.15 (0.36) relative units to 0.77 (0.89), the degree of cortical cataract increased (p = 0.001) from 1.38 (0.57) relative units to 1.79 (0.41) relative units, and the degree of nuclear cataract increased (p = 0.001) from 1.48 (0.68) relative units to 1.96 (0.59) relative units. The increase in the degree of cataract was significantly (p <0.05) correlated with the duration of the follow up time (p = 0.004 for the nuclear cataract; and p = 0.004 for the subcapsular posterior cataract), and with the number of intravitreal re-injections of triamcinolone acetonide.
With respect to other complications of the intravitreal injection of triamcinolone acetonide, we found that in none of the patients cortisone crystals had settled on the macular region. The crystals were preretinally located in the vitreous cortex at the 6 o’clock position and did not interfere optically with vision. Additionally, a toxic effect of triamcinolone acetonide crystals lying on the macular has not been shown, yet. No cases of postoperative infectious endophthalmitis, rhegmatogenous retinal detachment, or proliferative vitreoretinopathy occurred.
DISCUSSION
The unwanted proliferation of intraocular tissue is one of the important problems, largely unsolved, in clinical ophthalmology. This problem arises in subretinal neovascular tissue in eyes with exudative age related macular degeneration, with vascular retinal cells in eyes with ischaemic retinopathies, and with retinal pigment epithelium cells in the case of proliferative vitreoretinopathy. Corticosteroids have long been known to reduce inflammation and to suppress proliferation of cells. Consequently, steroids have been used for treatment of many ocular diseases, given either locally or systemically. Often, however, the intraocular concentration of cortisone was not high enough, or the systemic side effects were too pronounced, to effectively treat the ocular disorder. Taking into account that the eye comprises only 0.01% of the whole body volume, and considering that for achieving high concentrations of a drug at its site of action it is best to apply it directly into the region of required action, Machemer, Peyman, and other researchers studied the possibility of injecting cortisone directly into the eye, in experimental settings in animals as well as in selected clinical situations in patients.20,29,30,33–36 Machemer and co-workers as well as other researchers found that the cortisone may not be toxic to the intraocular tissue.29,30 It agrees with clinical observations of eyes into which cortisone accidentally was injected37 as well as with recent clinical and experimental studies on the therapeutic effect of intravitreal triamcinolone acetonide or other steroids, giving either as an intravitreal injection of crystals or applied in intravitreally implanted slow release devices, for various intraocular oedematous, neovascular, inflammatory, or proliferative diseases.7–21,24–28,31,38–41 Additionally, investigations have been carried out to examine the effect of triamcinolone acetonide on microglial morphology and modulation of permeability and intercellular adhesion molecules in exudative age related macular degeneration,42,43 and on the effect of triamcinolone acetonide on preretinal and subretinal neovascularisation.44–49
In agreement with the previous studies mentioned, the results of the present study suggest that the intravitreal triamcinolone acetonide may be useful to stabilise or temporarily improve visual acuity in patients with progressive exudative age related macular degeneration. The majority of patients included in the present study showed a slight increase or a stabilisation of visual acuity during the follow up period (Figs 1–6). In that context, one has to consider that the effect of the significant increase in the degree of cataract on visual acuity has not been taken into account in the assessment of visual acuity. The cataract associated decrease in visual acuity may have compensated or covered a possible increase in visual acuity due to the effect of triamcinolone acetonide. From the data analysis it has remained unclear which subgroup of patients with exudative age related macular degeneration may benefit most or least from the intravitreal injection of triamcinolone acetonide. There was a tendency that patients with a relatively high preoperative visual acuity may benefit most; however, no statistical significance for this observation was found.
The results of the present study are in agreement with other clinical and experimental studies. In 1998, Challa and co-workers25 evaluated safety and efficacy of intravitreal triamcinolone after 18 months of follow up in patients with exudative age related macular degeneration considered unsuitable for laser photocoagulation. In the non-randomised clinical pilot study, 30 eyes of 28 patients were treated with an intravitreal injection of triamcinolone (4 mg). Of the 20 eyes with initial visual acuity of 0.10 or better, vision was maintained in 11 eyes (55%), while six eyes (30%) suffered severe visual loss (six or more lines). Visual acuity improved in three of 10 eyes with initial vision of 3/60 or worse. The authors concluded that a single intravitreal injection of 4 mg triamcinolone may be reasonably well tolerated and may be helpful in the treatment of exudative age related macular degeneration. In a similar setting, Wingate and Beaumont reported a significant elevation of intraocular pressure of more than 5 mm Hg found in approximately 30% of 113 patients receiving an intravitreal injection of triamcinolone acetonide for treatment of exudative age related macular degeneration.27 Eleven per cent of the patients showed a rise in intraocular pressure of more than 10 mm Hg. These figures fit with data on the corticosteroid responsiveness of intraocular pressure in the general population and with the frequency of an increase in intraocular pressure in the present study. In a randomised clinical trial, Danis and colleagues examined the effects of intravitreal injection of 4 mg triamcinolone acetonide on the visual and clinical course of exudative age related macular degeneration in 27 patients who were compared with a non-treated control group.28 The authors found that visual acuity was significantly (p <0.005) better in the treated group compared with control subjects at 3 and 6 month follow up. Intraocular pressure elevation was seen in 25% of treated patients, but was controlled with topical medications. Progression of cataract was more frequently detected in the treated group. The authors concluded that intravitreal triamcinolone acetonide may provide improvement in visual acuity in exudative age related macular degeneration.
The results of the present study and of the other investigations described are in contrast with a recent study by Gillies and colleagues,50 who found no effect of 4 mg of intravitreal triamcinolone acetonide on the development of severe visual loss over a follow up period of 1 year. Reasons for the discrepancy between the studies may be the amount of triamcinolone acetonide injected into the vitreous, in the influence of increasing cataract on visual acuity, and perhaps the necessity of intravitreal re-injections. A hint for the latter is that three of the six patients who received a second intravitreal injection experienced a re-increase in visual acuity after the second injection (Table 4) (Fig 6).
With respect to the duration of the therapeutic effect of 25 mg of intravitreal triamcinolone acetonide, a recent study on patients with diffuse macular oedema found an increase in visual acuity for 17 (81%) of 21 eyes with a follow up period of more than 1 month.51 In that study, visual acuity started to decrease again about 4–5 months after the injection, when the triamcinolone acetonide crystals disappeared. A similar observation was made in the present study in which after an initial rise in visual acuity 2–4 months after the injection, visual performance slightly decreased again, perhaps due to a resolving and disappearing of the triamcinolone acetonide crystals. Six patients received a second injection after which visual acuity increased again in three patients. The question arises whether intravitreal injections of triamcinolone acetonide may be repeated within 3–4 months to keep the intravitreal concentration of steroids relatively high to prevent further growth of subretinal neovascular tissue. One of the main questions in that matter is whether and how many intravitreal injections of such high dosages of steroids as used in the present and previous studies can be tolerated by the eye.
Complications of the intravitreal triamcinolone acetonide were twofold. About 50% of the eyes developed a steroid induced secondary ocular hypertension. In all but one of these eyes, however, intraocular pressure could be normalised by topical antiglaucomatous medication, and glaucomatous damage of the optic nerve was not observed to develop or to progress. Since one eye with pre-existing primary open angle glaucoma before the intravitreal injection developed intraocular pressure readings of higher than 60 mm Hg and needed glaucoma surgery, one may be relatively hesitant to use intravitreal triamcinolone acetonide in eyes with pre-existing open angle glaucoma. The presence of open angle glaucoma, however, may also not be an exclusion criterion for the use of intravitreal triamcinolone acetonide in patients with progressive exudative macular degeneration if no other therapy is available. The other complication observed in the present study was, as expected, the cataractogenic effect of intravitreal triamcinolone acetonide. Although in most of eyes with exudative macular degeneration some degree of cataract is usually present, only less than 20% of eyes who received an intravitreal injection of 25 mg of triamcinolone acetonide underwent cataract surgery within the first 6 months after the injection.51 This suggests that the development of cataract as treatable complication of intravitreal triamcinolone acetonide may not be a contradiction for the intravitreal application of triamcinolone acetonide. Other complications such as postoperative infectious endophthalmitis, rhegmatogenous retinal detachment, or proliferative vitreoretinopathy have not been observed yet in the patients included in the present study.
There are limitations of the present study. Since this is not a randomised study comparing a study group with a control group, the design of the study may be the weakest point of the investigation. Comparing the results of the present study with those of the control group and the Treatment of Age Related Macular Degeneration with Photodynamic Therapy (TAP) Study, however, the patients of the present study do not markedly show worse results with respect to the number of patients with improvement or loss of visual acuity after 3 and 6 months of follow up.4–6 Another limitation of the present study is that the effect of increasing cataract could not be taken into account when assessing the visual acuity after the intravitreal injection. It may serve, however, only to underline the results of the study that the intravitreal injection of 25 mg of triamcinolone acetonide may stabilise or increase visual acuity in some patients with progressive exudative age related macular degeneration.
REFERENCES
Linked Articles
- BJO at a glance