Article Text

Abstract
Background: To assess the reproducibility of ophthalmodynamometric measurements using a new, Goldmann contact lens associated, device allowing biomicroscopic visualisation of the optic disc.
Methods: The prospective clinical study included 87 eyes of 58 subjects presenting with a normal fundus (n=40), or ocular diseases (n=47). With topical anaesthesia, a Goldmann contact lens, fitted with a pressure sensor mounted into the holding ring of the contact lens, was placed onto the cornea. Pressure was applied onto the globe through the contact lens, and the pressure values obtained when the central retinal vessels started pulsating were noted. The measurements were performed 10 times.
Results: The mean coefficients of variation for redeterminations of the collapse pressure of the central retinal vein and artery were 16.3% (SD 11.4%), and 8.5% (4.1%), respectively.
Conclusions: A simple and new, Goldmann contact lens associated, ophthalmodynamometer allows central retinal artery and vein collapse pressure measurements which are reproducible in a clinical setting.
- ophthalmodynamometry
- central retinal vein collapse pressure
- central retinal artery collapse pressure
- intraocular pressure
Statistics from Altmetric.com
- ophthalmodynamometry
- central retinal vein collapse pressure
- central retinal artery collapse pressure
- intraocular pressure
Ophthalmodynamometry is a relatively old method to determine the pressure in the central retinal vessels. Popular in the 1960s and 1970s, it included increasing the intraocular pressure by indenting the globe with a device applying a standardised pressure on the globe, and observing the optic nerve head ophthalmoscopically.1–4 Owing to the cumbersome methodology leading to problems with a standardised indenting of the globe and difficulties in observing the optic nerve head and in detecting the pulsations of the retinal vessels, the technique was mostly abandoned when Doppler sonography was introduced into medicine and allowed the assessment of the blood perfusion of the carotid arteries. With the development of a new ophthalmodynamometer consisting of a conventional Goldmann contact lens and a pressure sensor mounted into the holding ring of the contact lens, however, the problems of the original technique of ophthalmodynamometry may have partially been reduced.5,6 Standardisation of the pressure applied onto the globe has been facilitated, and the biomicroscopic observation of the optic nerve head should become easier by using a slit lamp and a Goldmann contact lens instead of an ophthalmoscope. An additional advantage of the new technique may be that it can be performed by a single examiner who no longer needs the help of a second person indenting the globe.
Since for a new method, reproducibility of its measurements has to be determined as a first step for its validation, we aimed to evaluate the reproducibility of the new ophthalmodynamometric technique in a clinical setting by examining normal subjects and patients with different ocular diseases.
PATIENTS AND METHODS
The prospective clinical observational study included 87 eyes (46 right eyes) of 58 subjects (31 females) with a mean age of 67.8 (SD 10.3) years (range 40.8–95.1 years). Refractive error ranged between −7 dioptres and +5 dioptres. The study group was composed of 40 eyes with a normal appearance of the fundus, with or without cataract; 15 eyes with primary or secondary open angle glaucoma; seven eyes with a stenosis of the carotid artery; six eyes with dilated retinal veins in the sense of a retinal stasis syndrome; four eyes with diabetic retinopathy; four eyes with dilated episcleral veins; three eyes with branch retinal vein occlusion; three eyes with endocrine orbitopathy; two eyes with increased intracranial pressure; two eyes with a macular hole; and one eye with central retinal vein occlusion. For 29 subjects, both eyes were included in the study. For the remaining 29 subjects, only one eye was examined for reasons such as dense cataract or a recently performed surgical intervention. The methods applied in the study adhered to the tenets of the declaration of Helsinki for the use of human subjects in biomedical research.
The ophthalmodynamometer (Meditron GmbH, Poststrasse 19-21, 66333 Völklingen, Germany) consisted of a conventional Goldmann contact lens fitted with a pressure sensor ring at its outer margin where the Goldmann contact lens is usually held during an ophthalmoscopic examination. Into the holding grip of the Goldmann contact lens, a pressure sensor was incorporated consisting of five parts: (1) a metallic holding grip with (2) a metallic cover on the outer surface acting to compress flexible structures in the interior part of the holding grip; (3) the flexible trabeculae composed of copper-beryllium and acting as the main pressure measuring unit; (4) a metallic structure on which the trabeculae rest; and (5) the plastic ring which is in contact with the contact lens and which is usually taken to hold the Goldmann contact lens. The calibration curve is linear. The measurements are given as relative units. The pressure sensor ring was connected by a thin cable with a small monitor on which the pressure continuously measured by the sensor ring could be read. After medical mydriasis using tropicamide 0.5%, the Goldmann contact lens of the ophthalmodynamometer was placed onto the corneal surface with topical anaesthesia. By slightly applying increasing pressure onto the contact lens, the optic nerve head was continuously observed biomicroscopically. When the central retinal artery or its branches on the surface of the optic nerve head showed early pulsations, the pressure measured by the sensor ring in the Goldmann contact lens was noted. When in an independent and second step of the examination, the central retinal vein or one of its branches on the optic disc surface started to show pulsations, the value given by the pressure sensor was noted as the central retinal vein collapse pressure. All measurements were repeated nine times.
For all eyes included in the study the retinal arterial collapse pressure could be determined. Thirty (34.5%) eyes showed a spontaneous pulsation of the central retinal vein, so that the central retinal vein collapse pressure was measured by ophthalmodynamometry for 57 eyes.
In a first step, the individual coefficient of variation as a measure of the reproducibility of the technique was calculated as the quotient of the standard deviation divided by the mean of the measurements for each individual patient and subject included in the study. In a second step, the overall coefficient of variation was determined as the ratio of the mean standard deviations divided by the mean of the means what was equivalent to the mean of the individual coefficients of variations.
RESULTS
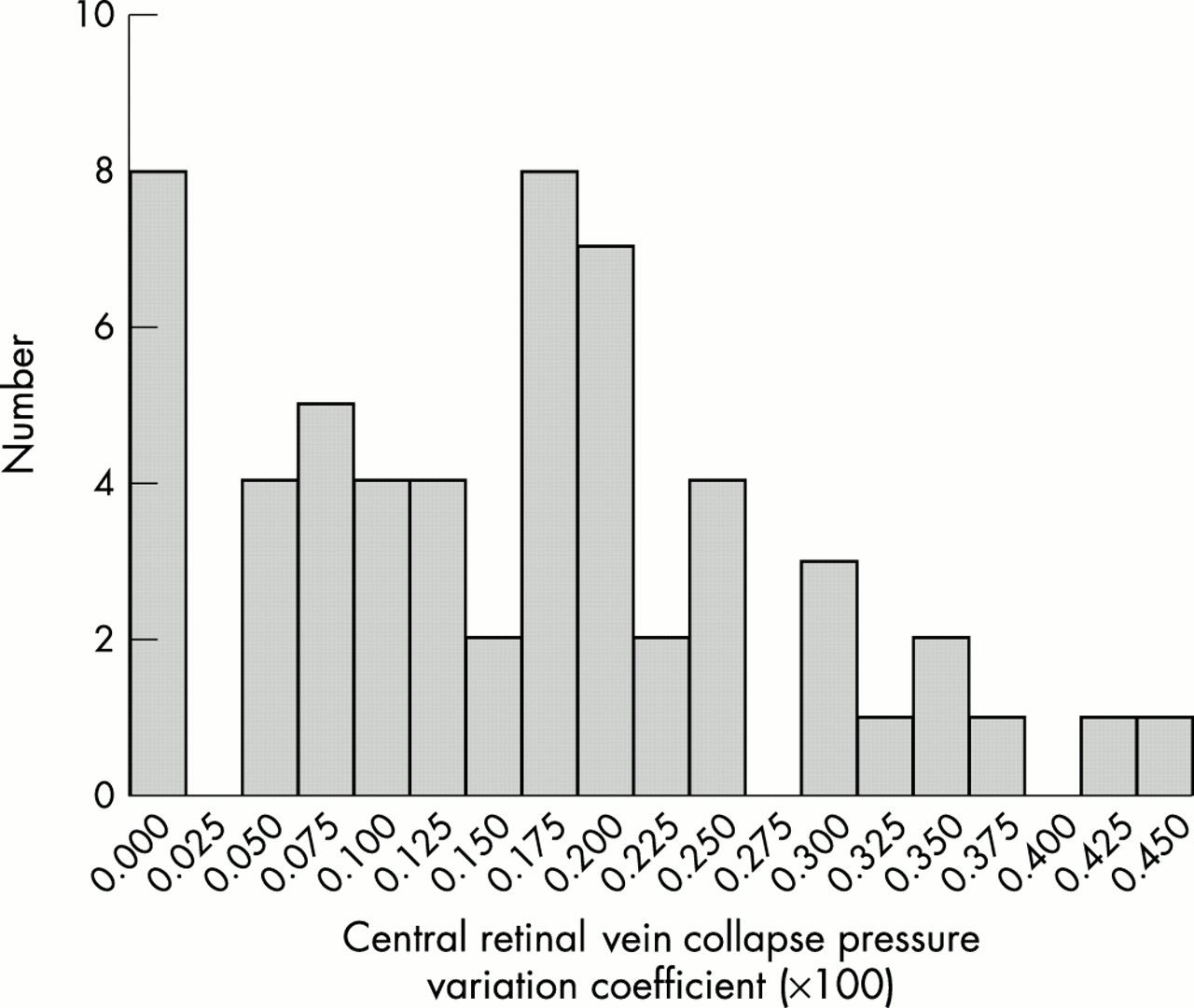
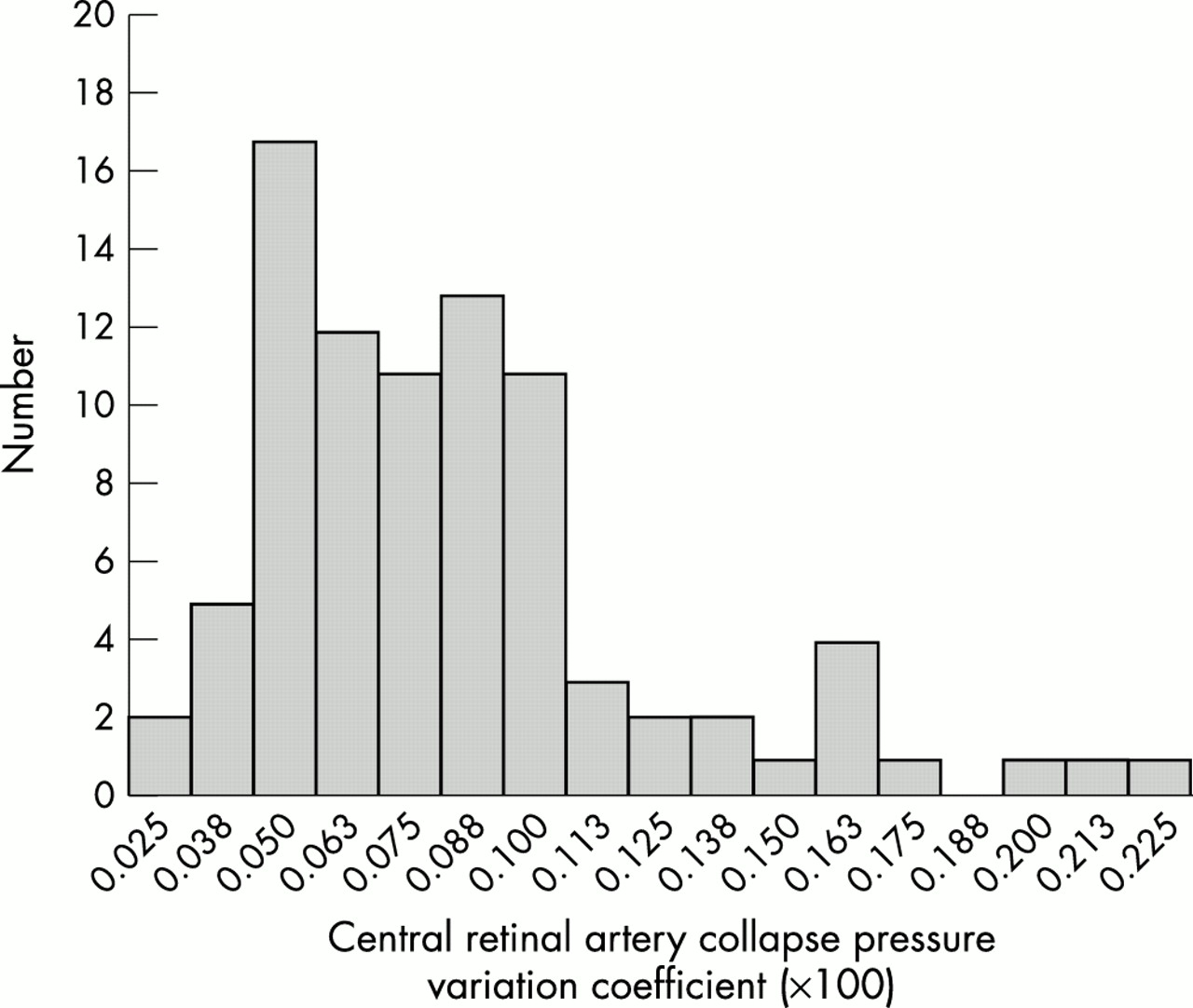
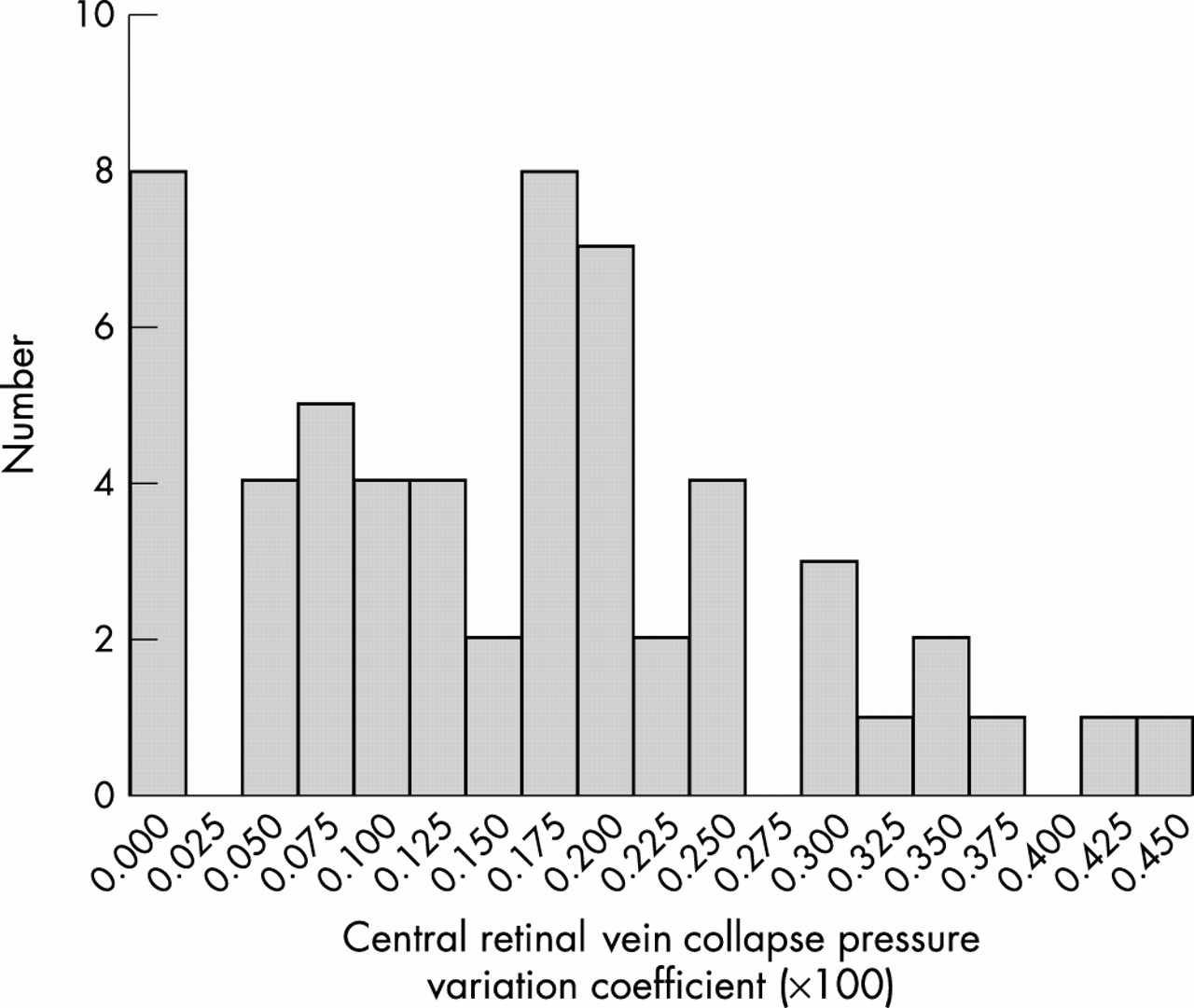
The mean coefficient of variation measured 16.3% (SD 11.4%) for the redeterminations of the central retinal vein collapse pressure in the eyes without spontaneous central retinal vein pulsation (n=57), and 8.5% (4.1%) for the remeasurements of the central retinal artery collapse pressure (n = 87) (Figs 1 and 2). Including the eyes with spontaneous central retinal vein pulsation, the coefficient of variation measured 10.7% (12.0%) for the redeterminations of the central retinal vein collapse pressure. The coefficient of variation for the redeterminations of the venous collapse pressure and the coefficient of variation for the redeterminations of the arterial collapse pressure, respectively, were statistically independent of age (p = 0.89 and p = 0.84, respectively), sex (p = 0.07, and p = 0.14, respectively), systolic blood pressure (p = 0.62 and p = 0.63, respectively), and blood pressure (p = 0.77 and p = 0.66, respectively).

Histogram showing the distribution of the individual coefficients of variation of ophthalmodynamometric measurements of the central retinal artery collapse pressure.
{kind=link}
{kind=link}
Histogram showing the distribution of the individual coefficients of variation of ophthalmodynamometric measurements of the central retinal vein collapse pressure.
The coefficient of variation for the redeterminations of the central retinal vein collapse pressure was significantly (p<0.001) higher than the coefficient of variation for the remeasurements of the central retinal artery collapse pressure. The coefficient of variation of the redeterminations of the central retinal artery collapse pressure depended significantly and negatively (p = 0.007; correlation coefficient −0.29) on the central retinal artery collapse pressure. The coefficient of variation of the redeterminations of the central retinal vein collapse pressure was statistically independent (p = 0.13) on the central retinal vein pressure.
Addressing the question of whether the reproducibility of the measurements varies if, instead of 10 measurements, five measurements were taken, we recalculated the coefficients of variation taking into account only the first five measurements. Using these data, the mean coefficient of variation measured 15.0% (11.0%) for the redeterminations of the central retinal vein collapse pressure, and 7.9% (4.1%) for the remeasurements of the central retinal artery collapse pressure. The coefficients of variation were significantly (p<0.001) lower for the retinal artery collapse pressure measurements than for the retinal vein collapse pressure determinations. The coefficients of variation calculated by taking five measurements did not vary significantly from the coefficients of variation calculated by taking 10 measurements (p = 0.41 for artery collapse pressure remeasurements; p=0.19 for vein collapse pressure measurements).
DISCUSSION
To measure the collapse pressure of the central retinal vessels can be of importance in the assessment of the blood perfusion into, and out of, the eye and brain. Supplying information on the blood pressure of the central retinal artery, ophthalmic artery, and internal carotid artery, ophthalmodynamometry has been used clinically for the detection of haemodynamically significant carotid artery stenosis.1–4,6–10 On the venous side, estimation of the blood pressure in the central retinal vein can give information about the cerebrospinal fluid pressure,5,11–14 the orbital tissue pressure, and the pressure in the cavernous sinus, since the central retinal vein passes, when leaving the optic nerve, through the cerebrospinal fluid space, then runs through the orbit, and enters the superior ophthalmic vein which drains into the cavernous sinus. The clinical importance of the measurement of the central retinal vein collapse pressure may thus be important for patients with presumed elevated intracerebral pressure, patients with arteriovenous fistulas in the cavernous sinus or contributing branches of it, patients with increased orbital pressure such as in endocrine orbitopathy, and patients with occlusions of the central, or branch, retinal veins, to mention only some examples.
The newer techniques for the examination of the ocular blood perfusion system,15,16 such as Doppler sonography which displaced the older technique of ophthalmodynamometry, cannot determine the collapse pressure in the retinal vessels, which may be essential to obtain information about the pressure in the vessels serving the eye, and in the vessels and tissues into which the retinal venous blood is drained. With the new ophthalmodynamometer used in the present study, one may be able to partially overcome the limitations of the old ophthalmodynamometric devices.17,18 Determinations of the retinal blood pressure may become possible with a higher reproducibility. This has been suggested in the present study in which subjects and patients with various ocular, orbital, or cerebral diseases were included, and in which the variation of the ophthalmodynamometric remeasurements was less than 10% for the central retinal artery collapse pressure, and about 15% for the central retinal vein collapse pressure. These figures may be reasonably low so that one may argue that the new device may allow better reproducible ophthalmodynamometric measurements than was possible 30 years ago.
REFERENCES
Footnotes
-
Proprietary interest: none.