Article Text

Abstract
Aim: To study “manual small incision cataract surgery (MSICS)” for the rehabilitation of cataract visually impaired and blind patients in community based, high volume, eye hospital setting; to compare the safety and effectiveness of MSICS with conventional extracapsular cataract surgery (ECCE).
Methods: In a single masked randomised controlled clinical trial, 741 patients, aged 40–90 years, with operable cataract were randomly assigned to receive either MSICS or ECCE and operated upon by one of eight participating surgeons. Intraoperative and postoperative complications were graded and scored according to the Oxford Cataract Treatment and Evaluation Team recommendations. The patients were followed up at 1 week, 6 weeks, and 1 year after surgery and their visual acuity recorded.
Results: This paper reports outcomes at 1 and 6 weeks. 706 of the 741(95.3%) patients completed the 6 week follow up. 135 of 362 (37.3%) of ECCE group and 165 of 344 (47.9%) of MSICS group had uncorrected visual acuity of 6/18 or better after 6 weeks of follow up. 314 of 362 (86.7%) of ECCE group and 309 of 344 (89.8%) of MSICS group had corrected postoperative vision of 6/18 or better. Four of 362 (1.1%) of ECCE group and six of 344 (1.7%) of MSICS group had corrected postoperative visual acuity less than 6/60. There were no significant differences between the two groups for intraoperative and severe postoperative complications.
Conclusion: MSICS and ECCE are both safe and effective techniques for treatment of cataract patients in community eye care settings. MSICS needs similar equipment to ECCE, but gives better uncorrected vision.
- extracapsular cataract surgery
- small incision cataract surgery
- India
Statistics from Altmetric.com
Cataract is the chief cause of avoidable blindness in India and throughout the world.1 There are an estimated 9–12 million blind in India, half of which can be attributed to cataract.2 It is estimated that another three million develop visually disabling cataracts each year.3 Cataract extraction accounts for the majority of the workload of ophthalmic units worldwide. Extracapsular cataract extraction with posterior chamber intraocular lens implantation (PCIOL) was the most frequent surgical technique until the past decade.4
The use of a smaller incision with the advantages of faster rehabilitation, less astigmatism5 and better postoperative vision without spectacles led to phacoemulsification becoming the preferred technique where resources are available. However, cost, both in terms of equipment and training has limited its use in the developing world. Thus there is a dichotomy with different standards of care between the developed and the developing world. Manual small incision surgery in which the nucleus is delivered through a 6–6.5 mm scleral tunnel is claimed to have similar advantages6,7 to phacoemulsification.
High quality, high volume cataract surgery is needed in community eye care centres to effectively manage the large backlog of cataract blindness8; but so far the effectiveness of manual small incision surgery has not been formally compared to the established extracapsular technique in this setting. Our study was to make this comparison with a prospective randomised controlled clinical trial in a community based eye hospital setting.
METHODS
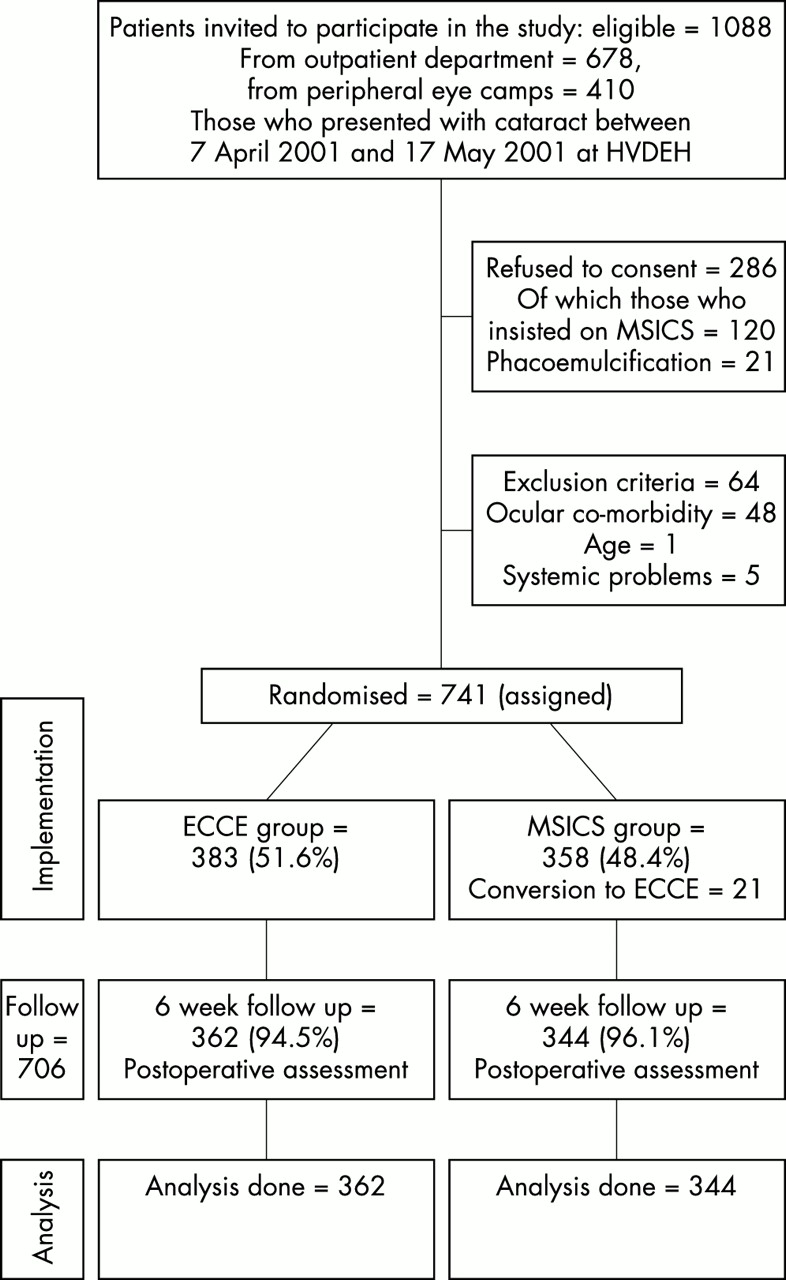
The trial setting was at Poona Blind Men’s Associations HV Desai Eye Hospital (HVDEH), Pune, India. All the 678 patients who attended the outpatient department of HVDEH in the specified study period and had been admitted for cataract surgery were requested to participate in the trial. Also all the 410 patients who had been admitted for cataract surgery in camps organised by the Solapur District Blindness Control Society in the specified study period, and who were transported to HVDEH, were invited to participate in the trial. Out of these 1088 patients, 286 refused to consent for the study, while another 61 were excluded as per preset exclusion criteria (that is, only 741 out of 1088 were taken for randomisation and further study, while 347 were considered non-study cases (Table 1 and Fig 1). The major reason for refusal was that patients preferred one kind of surgery (141 out of the 286), small incision or phacoemulsification, and were operated upon as per their choice. The exclusion criteria were any ocular co-morbidity capable of compromising vision, if they needed combined surgical procedures, or if the axial length of the eye was more than 26 mm. The age limit was set between 40 to 90 years.
Reasons for exclusion from the randomised trial

Recruitment, randomisation, and flow of patients through the various stages of the trial.
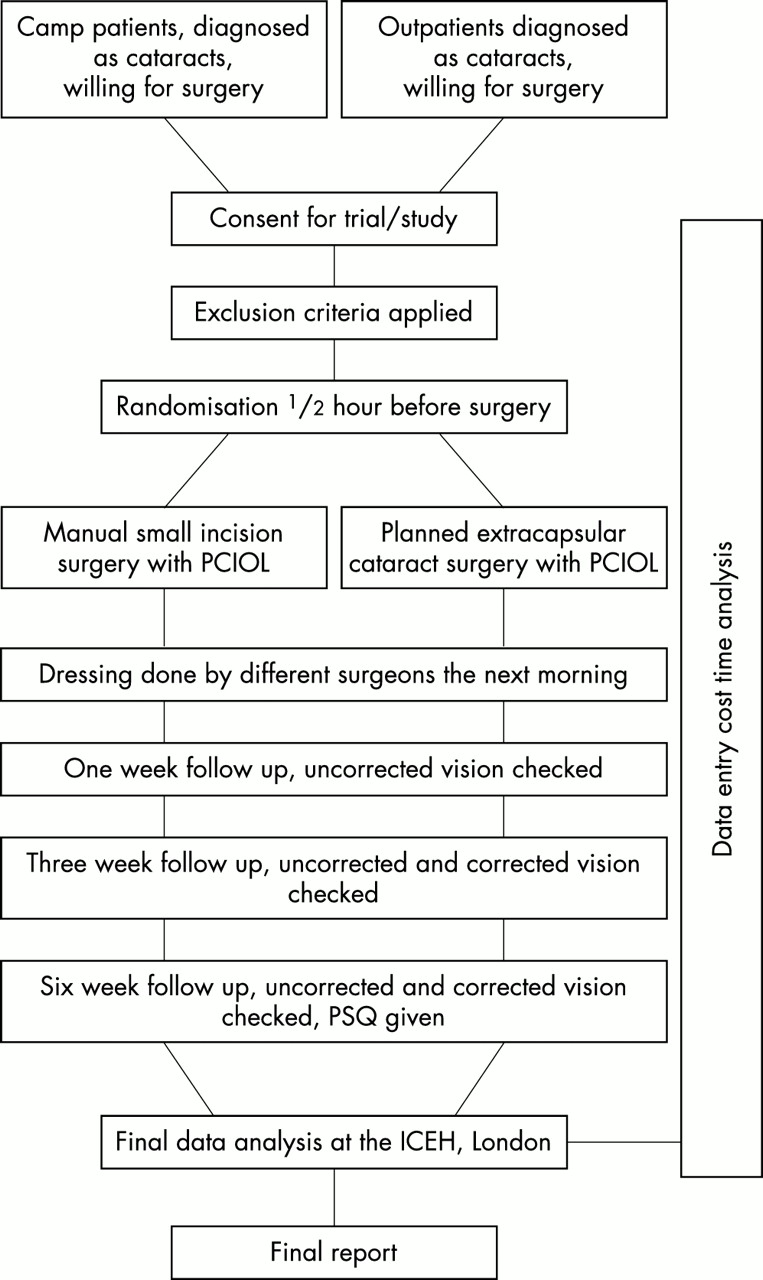
The two planned treatments were extracapsular cataract extraction (ECCE) and manual small incision cataract surgery (MSICS). In both techniques a posterior chamber intraocular lens was implanted (PCIOL). Figure 2 is the flow chart for the trial.

{kind=link}
{kind=link}
Flow chart for randomised control trial to gauge the viability of manual small incision surgery for quick and effective visual rehabilitation of the cataract patients in community eye care settings.
Table 2 shows the distribution of prognostic factors in the two treatment groups, extracapsular cataract extraction (ECCE) and manual small incision cataract surgery (MSICS). Percentages are of the total number in the treatment group. There was no significant difference between the two groups for sex and age. The average age of ECCE group was 64.32 years (SD 8.43) and of the MSICS group was 64.04 years (SD 8.96).
Distribution of baseline characteristics of both groups
Surgical technique
In ECCE, a 12–14 mm corneoscleral section was made after raising a conjunctival flap, the lens capsule opened and the lens nucleus expressed or removed with a vectis without fragmentation. The manual irrigation aspiration system was then used to remove the remaining cortical matter and a 6.5 mm three piece PMMA intraocular lens was inserted into the capsular bag, and the incision closed with five 8-0 interrupted sutures. In MSICS, a 6.5–7.5 mm scleral tunnel was created with a straight or frown incision. A side port was created to facilitate intraocular manipulations. The capsule was opened with continuous curvilinear capsulorrhexis and the nucleus was dislocated into the anterior chamber. Viscoelastic was injected around the nucleus and an irrigating vectis was inserted below it. The nucleus was then delivered in whole, or in parts, through the scleral tunnel. The remaining cortex was removed with manual irrigation-aspiration and a 6.5 mm three piece PMMA lens implanted in the bag. The irrigating fluid was inserted through the side port to test the integrity of the tunnel.
Assessment before surgery included measurement of visual acuity, examination to exclude other eye disease, keratometry, A-scan and general physical examination and urine testing. The IOL power calculation aimed for emmetropia.
All the surgeons were proficient in ECCE and MSICS and were required to have performed a minimum of 500 of ECCE and 50 of MSICS. The surgical protocol for each technique was standardised to reflect best practice by experienced surgeons. A total of eight surgeons, with 2–5 years post-residency were recruited for the study.
The outcome measures were as follows.
The primary outcome was the proportion of patients having uncorrected and corrected visual acuity of 6/18 or better at 6 weeks by both techniques. This was measured with the Snellen’s charts at 6 metre distance.
The secondary outcomes were:
Complications, both intraoperative and postoperative, with either technique. They were graded and scored as described by the Oxford Cataract Treatment and Evaluation Team (OCTET) protocol9 (see appendix 1 and 2). Failure to implant an IOL and/or conversion from MSICS to conventional ECCE was recorded. Grade I were trivial complications (scores 1–4) that may have needed medical therapy, but were not likely to result in a marked drop in visual acuity. Grade II were intermediate complications (scores 5–8) that needed medical therapy, and would have resulted in a marked drop in visual acuity if left untreated. Grade III were serious complications (scores 9–13) that would have needed immediate medical or surgical intervention to prevent gross visual loss.
The average surgical time for each technique. Surgeon time was measured from the start to the end of the procedure; putting on to removing the lid speculum. This was measured with a stopwatch in minutes and seconds.
Data were also collected on vision related quality of life, patient satisfaction, and economic outcomes, which will be presented in a subsequent article.
Uncorrected postoperative visual acuity
Corrected postoperative visual acuity
OCTET grades and scores for intraoperative complications
Types of moderate to severe intraoperative complications
OCTET grades and scores for postoperative complications, at 6 week follow up
Types of postoperative complications with OCTET score more than 2, at 6 week follow up
Intraoperative complications by OCTET grade and score
Postoperative complications by OCTET grade and score
Outcomes were assessed on the first postoperative day, the first week, the sixth week and after 1 year of surgery. Spectacles were prescribed on the 6 week postoperative visit to all patients.
Sample size estimation
Assuming 1.1 randomisation, 80% power (and ∝ = 0.05) to detect a difference between proportion of 10% or more in uncorrected postoperative visual acuity (for example, 60% v 70%), the required sample size calculated to be 584 patients in total. Allowing for 20% loss to follow up, the study aimed to randomise a total of 720 patients.
Ethical considerations
An informed consent based on the guidelines of the Helsinki protocol was taken from all patients. The ethics committee of the hospital approved the study design; both the techniques were accepted standards of care.
Assignment
Each patient was randomly allocated to one of the two groups by drawing lots (ballots). There was always a 50% chance of the patient getting one particular kind of intervention. The operating surgeons also drew ballots for the type of surgery they were supposed to do that day, at the beginning of the theatre list immediately before scrubbing. This random assignment was done in the presence of the anaesthetist, operation theatre senior nurse, and another non-operating ophthalmologist. One surgeon did only one kind of surgery (ECCE or MSICS) at each operating session. This resulted in some surgeons doing more surgeries of one kind if the operating list was more compared to the other technique when the list was shorter. This unorthodox method was used to help calculate the cost of consumables used for a particular kind of surgery. In a high volume setting, some consumables are utilised for several successive procedures, which helps save valuable resources, time and money. This was done to increase the external validity of the study. Imbalance of surgeon assignment may have introduced bias, but this was dealt with by stratification by surgeon in the analysis.
Masking
The patients were not informed as to the type of intervention they would receive, in the OT and during follow up. The surgeons were unaware until scrubbing up which surgery they would perform that day. They were also unaware which patient would be brought to them for surgery and did not examine the patients the next day. Internee doctors and optometrists did postoperative visual acuity testing and administering the questionnaires. They were not told about the type of surgery done.
Health workers interviewing the patients were also unaware of the assignment. The optometrists and ophthalmic assistants examining the patients could have found out postoperatively about the type of surgery done.
RESULTS
In all, 362 of the 383 (94.5%) ECCE patients and 344 of the 358 (96.1 %) MSICS patients completed (presented for) the 6 week follow up. Their corrected and uncorrected visual acuity are as given in Tables 3 and 4. The 35 patients lost to follow up were similar on the first postoperative day.
The 135 out of the 362 (37.3%) cases of the ECCE group and 165 out of the 344 (47.9%) cases of the MSICS group had uncorrected (without glasses) postoperative vision of 6/18 or better (Table 3). There is a significant difference between the two groups using the χ2 test. Using 2 × 2 tables, risk ratio is 1.21, 95% confidence limits are 1.06<RR<1.37. There is a significant difference between the two groups for uncorrected visual acuity. On doing stratified analysis for surgeon as confounder, crude risk ratio is 1.21 and summary risk ratio is 1.16 (1.02<RR<1.33), p value 0.1278. The χ2 test does not suggest that risk ratios differ by stratum, thus confounding is small.
A total of 314 out of 362 (86.7%) cases of ECCE group and 309 of the 344 (89.8%) cases of the MSICS group had corrected (after retinoscopic refraction) postoperative vision of 6/18 or better (Table 4). Using 2 × 2 tables, risk ratio is 1.30, 95% confidence limits are 0.86<RR<1.96. There is a no significant difference between the two groups for corrected visual acuity. Using a Mantel-Haenszel summary χ2 test for stratified analysis, with surgeon as confounder, crude risk ratio is 1.3 and summary risk ratio is 1.17 (0.76<RR<1.8).
Four of the 362 (1.1%) in the ECCE group and 6 of the 344 (1.7%) in the MSICS group have corrected postoperative visual acuity less than 6/60, a poor outcome by any standards. There is no significant difference by the χ2 test.
The 366 of the 383 surgeries (95.6%) in the ECCE group and 329 of the 358 surgeries (91.9%) in the MSICS group were without any intraoperative complications (Table 5). Of the 358 patients who were assigned to the MSICS group, 21 nevertheless underwent ECCE surgery (SI-EC); either because the surgeons converted by extending the incision on facing an intraoperative difficulty, or because they felt they would not be able to do the MSICS in the very beginning after seeing the cataract (hard nucleus, miotic pupil). These 21 patients had a higher average intraoperative OCTET score and took longer time.
Seventeen of 383 surgeries in ECCE group and 29 of 358 surgeries in MSICS group had an intraoperative complication episode. Using 2 × 2 tables, risk ratio was 1.04 (1.00<RR<1.08). Moderated to severe intraoperative complications (posterior capsule rent and vitreous loss), were 10 (in 383) in ECCE group and 18 (in 358) in MSICS group (Table 6). The risk ratio was 1.03 (1.00<RR<1.06). Thus there was no significant difference between the two groups for the intraoperative complications.
Ninety four of 383 patients in ECCE group and 121 of 358 patients in MSICS group had a postoperative complication event in the first 6 weeks of follow up (Table 7). By applying the χ2 test, using 2 × 2 tables, risk ratio is 1.14 (1.04<RR<1.25). If only moderate complications are taken into account (OCTET grade II; there were no severe complications, grade III), there were three of 383 in ECCE group and five of 358 in MSICS group. By doing χ2 test, using 2 × 2 tables, risk ratio was 1.01 (0.99<RR<1.02). Thus while there is no significant difference between the two groups for the moderate or severe complications, MSICS group is associated with slightly more postoperative complications. Descemet’s folds and corneal oedema were more common in MSICS group.
DISCUSSION
There is a difference between the two groups (ECCE, MSICS) for the uncorrected postoperative visual acuity; 37.3% patients of the ECCE group and 47.9% of the MSICS group have postoperative vision of 6/18 or better without spectacles. After retinoscopic refraction, the figures are 86.7% and 89.8% respectively. The difference is narrowed. This compares with the results seen in Tilganga Eye Hospital, Kathmandu, Nepal; 87.1% patients had corrected postoperative visual acuity better than 6/18 after 2 months in a community eye hospital based setting.10 But this does not compare with the outcomes in Madurai Intraocular Lens Study (MILS)11 and the phaco trial in England.12 Twenty six eyes had visual acuity<6/60 due to astigmatism.
There was a poor outcome (postoperative visual acuity <6/60) in 1.1% patients of ECCE group and 1.7% of MSICS group. This is similar to complications and poor outcomes in MILS11 and the phaco trial.12 Great care was taken to maintain asepsis during the preoperative, surgical and postoperative procedures. The patients and health workers were educated to recognise and report any sign of infection.
The posterior capsular rent was the commonest major intraoperative complication. It was more frequent in MSICS group (18 in 358 surgeries), compared to ECCE group (10 in 383 surgeries). MSICS had however proportionately less incidence of vitreous loss (six in 18 rents, as against six in 10 in ECCE) as the self sealing incision helped maintain the anterior chamber and contain the vitreous. Anecdotally, the incidence of capsular rupture was higher in hypermature and hard cataracts and those with small fixed pupil. The latter caused difficulty in bringing the nucleus in anterior chamber during the MSICS. The mean OCTET score for intraoperative complication was slightly higher for MSICS, especially those that had to be converted to ECCE. Iridodialysis was a complication seen only in the MSICS group (two patients).
Iritis, posterior capsular opacification and Descemet’s folds were the commonest postoperative complications. The latter one was more common in the MSICS group (Table 8). 75.5% of patients in the ECCE group did not have any complication episode in the 6 weeks, but only 67.7% of MSICS were free from it. None of the patients had any grade III complications, endophthalmitis, hypopyon or pupillary block glaucoma. The sample size was insufficient to demonstrate complications, as the study was designed for good, not poor outcome.
Internal validity (deviations from the protocol)
All the patients with diagnosed operable cataract, whether outpatients or camp recruited patients, who were admitted to the hospital in the study period, were requested to participate. Mature and hard cataracts, which formed a significant proportion of the surgical workload, were not excluded. But two high myopes and one lens induced glaucoma were inadvertently taken for assignment, two to ECCE group and one to MSICS group and had subnormal results. Two patients of ECCE group were found to have ARMD and optic atrophy after surgery. All these patients were nevertheless analysed in the study. The 21 patients of the MSICS group who finally underwent ECCE were also analysed on ‘the intention to treat’ basis. Surgeon learning curves may be a reason for this.
The patients were unaware which intervention they received. However the medical and paramedical staff could have easily discovered the intervention done, even if they were not told about it.
In all, 706 of 741 (95.28%) of the patients could be followed up for 6 weeks. The followed up patients mirrored the baseline criteria. Extensive preoperative briefings and close community contacts, especially for camp patients, ensured that those with moderate to severe complications, or poor postoperative visual acuity reported back to the hospital. A major postoperative event is unlikely to have been missed. The twenty four ophthalmic assistants, 14 ophthalmologists, two anaesthesiologists, two social workers, five scrub nurses, four theatre assistants, three OPD nurses and three administrative staff, who contributed to the study all formed part of the regular hospital team. All of them were extensively briefed and a pilot was run for the study. Two optometrists and two internee doctors were recruited and trained for visual acuity testing and patient questionnaires, and to have an outsider’s perspective. A multimember multidisciplinary ethical committee reviewed the proceedings on regular basis.
External validity
The HVDEH, a comprehensive dedicated community eye care centre, is mostly staffed by ophthalmologists who have 1–5 years’ post-residency experience. An ophthalmology residency is typically 2–3 years in India. This reflects the trend in most community eye care centres in the Third World. The surgeon profile is of people trained in different centres and of varying experience. A large proportion of paramedical staff do not have more than 1 year of formal healthcare qualification, but are trained in-house under supervision for eye care. A well established community outreach program ensures patient recruitment. This is supplemented by emphasis on quality, which helps generate the high volume necessary for the subsidised care. Ninety per cent of patients are non-paying or pay less than $12 for all their care. Preoperative and postoperative procedures are kept to bare essentials. Manual small incision surgery does not need any additional or costly consumables and the fixed facility is the same.
The research protocol was designed to reflect the actual working of the community eye care centre/hospital as close as possible. The randomisation sequence was designed to reflect the high quality, high volume operation theatre setting. Thus the cost of consumables and time for surgery calculated would mirror the use in regular circumstances. Preoperative, postoperative and follow up procedures were kept the same.
This pattern mirrors and can be followed by any centre in the rural and urban areas of the developing world.
Limitations of the study
The preoperative astigmatism and postoperative astigmatic decay were not compared. Also endothelial cell count, before and after both the techniques was not recorded due to lack of necessary equipment. Considering the increased incidence of postoperative Descemet’s folds in one arm, it would have been illuminating.
The surgeons had experience of high quality high volume surgery, which may not be available everywhere. The surgeon learning curves were not explored, as also the different styles. The cataract hardness grading was not done even though hard cataracts and small pupils accounted for the majority of conversions to ECCE from the MSICS group.
CONCLUSION
Manual small incision surgery is as safe as conventional ECCE surgery. The difference in intraoperative and postoperative complications is small. It gives uncorrected postoperative visual acuity of 6/18 or better in a greater proportion of patients (47.9% for MSICS as compared to 37.3% for ECCE); but the difference between two groups is smaller for the corrected postoperative visual acuity (89.8% in MSICS group and 86.7% in ECCE group having corrected visual acuity 6/18 or better after surgery).
A large proportion of patients do not wear their postoperative refractive (spectacle) correction.13 Considering this, wherever the requisite surgical expertise is available, manual small incision surgery is recommended as the procedure of choice for effective rehabilitation of the cataract patients.
Acknowledgments
This study was funded by a grant from HV Desai Eye Hospital, Pune and the Department for International Development, UK.
We thank Drs Darwin Minassian and Mark Myatt for help in data analysis. Drs Daksha Patel and Ellen Schwartz helped in planning the study. Dr Rahul Deshpande helped with the camp management; Drs Sucheta Kulkarni, Shilpa Joshi, Mahesh Dalvi, and Bageshri Gogate helped in translating and validating the questionnaires, information sheets and consent forms. We are grateful to Niranjan Pandya and the ethical committee of the HVDEH and Dr Doshi, the district ophthalmic surgeon, Solapur District, for permitting the study. Drs Arif Adenwalla, Tasnim Parkar, Megha Aghor, Kuldeep Dole, Kavita Verappa, and Amar Maske helped with the follow up, Drs Vikram Dalvi, Anand Reddy, Capt Kshirsagar, and Mr Amit Shinde with the patient interviews. Dr BR Shammanna helped with the write up and Dr Deepak Anpat, Mrs Shakuntala Kamble, and Dr Milind Joshi with patient assignment.
REFERENCES
Footnotes
Series editors: W V Good and S Ruit