Article Text

Abstract
Aims: To analyse the occurrence of subretinal fibrosis (SRF) after photodynamic therapy (PDT) with verteporfin in highly myopic eyes with subfoveal choroidal neovascularisation (CNV).
Methods: PDT with verteporfin was performed on 33 eyes of 32 highly myopic patients with subfoveal CNV. Patients were followed for 14–24 months and best corrected visual acuity (BCVA) and angiographic and funduscopic findings were recorded.
Results: Two patients (two eyes) were lost to follow up. SRF appeared in 14 of 31 eyes. SRF appeared more frequently in eyes with a spherical equivalent (SE) of less than −10 D, in patients of age equal to or less than 55 years, and when CNVs were larger than 1500 μm in diameter. SRF appeared more frequently in the group of patients with worse final BCVA.
Conclusions: The appearance of SRF after treatment is correlated with size of the CNV and SE. The results of this study indicate that highly myopic eyes with CNV treated with PDT do not show a decrease in BCVA, even though they develop SRF. The appearance of SRF after PDT in highly myopic CNV does not always imply a loss of BCVA from baseline, though its presence is more frequent in eyes with lower BCVA.
- subretinal fibrosis
- myopia
- choroidal neovascularisation
- photodynamic therapy
Statistics from Altmetric.com
High myopia is an ocular disease characterised by excessive axial length, and a number of changes in the ocular tissues, affecting approximately 2% of general population1 and 27–33% of myopic eyes.2 A major complication and cause of decreased central vision in these eyes is macular choroidal neovascularisation (CNV), which is often followed by subretinal fibrosis (SRF), as part of the myopic maculopathy that is the most common cause of vision loss in highly myopic patients.3
Different patterns of anatomical outcome, with variable results in terms of visual results have been described following the natural history and therapeutic approaches of myopic CNV.3–6
In this study we have investigated the occurrence of subsequent SRF in verteporfin photodynamic therapy (PDT) treated patients, more than a year since treatment was started.
PATIENTS AND METHODS
A total of 32 consecutive patients (33 eyes) with high myopia and subfoveal CNV were recruited from the retina unit at the Instituto Oftalmológico de Alicante, Spain, from June 2000 to February 2001. Informed consent was obtained from all patients.
Inclusion criteria for this study were similar to those previously published for the VIP-1 study and by our group in a previous report.6,7
The initial evaluation included refraction, best corrected visual acuity (BCVA) performed with the ETDRS charts (Lighthouse International, NY, USA), slit lamp examination, tonometry, fundus examination using indirect ophthalmoscopy and biomicroscopy, and fluorescein angiography, which was repeated on a 3 month schedule. Special attention was paid to the appearance of SRF and its relation to age, sex, size of CNV at baseline, spherical equivalent (SE), initial and final BCVA, and number of previous PDT sessions.
SRF was defined as the appearance of a whitish formation under the retina in the absence of blood or exudates which showed staining in late angiographic frames without leakage of fluorescein.8
Eyes were also classified according to the degree of chorioretinal atrophy following Avila’s classification3 in M1-M2 (choroidal pallor, tessellation, posterior staphyloma, or lacquer cracks), and M3-M4 (small atrophic patches to large geographic areas of chorioretinal atrophy in the macula).
Verteporfin PDT was performed as described previously.6,7 Only when angiographic confirmation of CNV was found did patients receive further treatment with PDT, which was performed not earlier than 3 months after the last session, and not later than 1 week after the last angiography.
The status of CNV after PDT was evaluated in terms of (1) active CNV: leakage observed at early phases of FA; (2) stabilised CNV (closed): leakage could not be observed during FA and no changes in the CNV size were observed; (3) enlarged CNV (reactivated): the size of CNV enlarged after treatment, with leakage at early phases of FA; (4) fibrosis: leakage could not be observed during FA but staining appeared at late phases of the FA.
Student’s t test for paired data was used to compare changes in BCVA at baseline and after follow up. The χ2 test was used to determine the association of SRF with different variables.
RESULTS
We have followed 33 eyes from 32 highly myopic patients with subfoveal CNV treated with verteporfin PDT. Two patients (two eyes) were excluded because they were lost to follow up after 6 months, and 31 eyes (11 right, 20 left) from 30 patients (10 male and 20 female) completed at least 14 months of follow up (mean 19.5 (SD 3.4) months, range 14–24 months).
Fourteen of 31 eyes (45%) had developed SRF by the end of follow up. SRF appeared between months 6 and 12 (mean 9.6 (2.7)). SRF appeared in males in four of 11 eyes (36%) (three patients of 10), and in females in 10 of 20 eyes (50%) (p= 0.26, χ2 test).
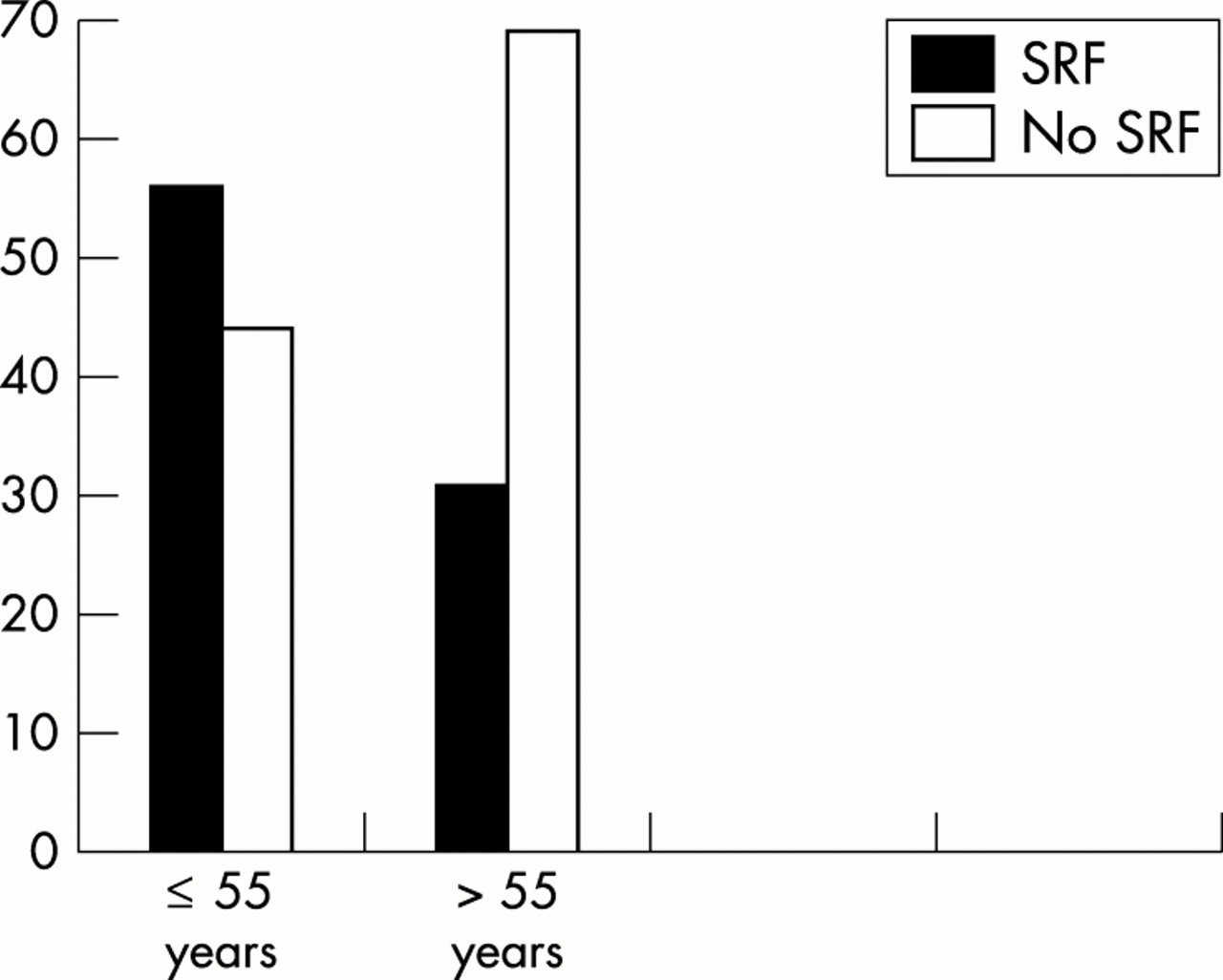
Patients were divided into two groups according to their age: group 1 with patients aged ≤ 55 years old (18 eyes) and group 2 with patients aged >55 years old (13 eyes). Mean age in the whole group of patients was 54.9 (14.0) years; for group 1 it was 44.9 (8.1) (range 27–55) and for group 2 it was 68.7 (6.4) years (range 56–79). SRF appeared in 10 of 18 eyes in group 1 (56%) and in four of 13 eyes in group 2 (31%) (p= 0.07, χ2 test) (Fig 1).

Appearance of subretinal fibrosis (SRF) in relation to the age group. The appearance of SRF is less frequent in patients over 55.
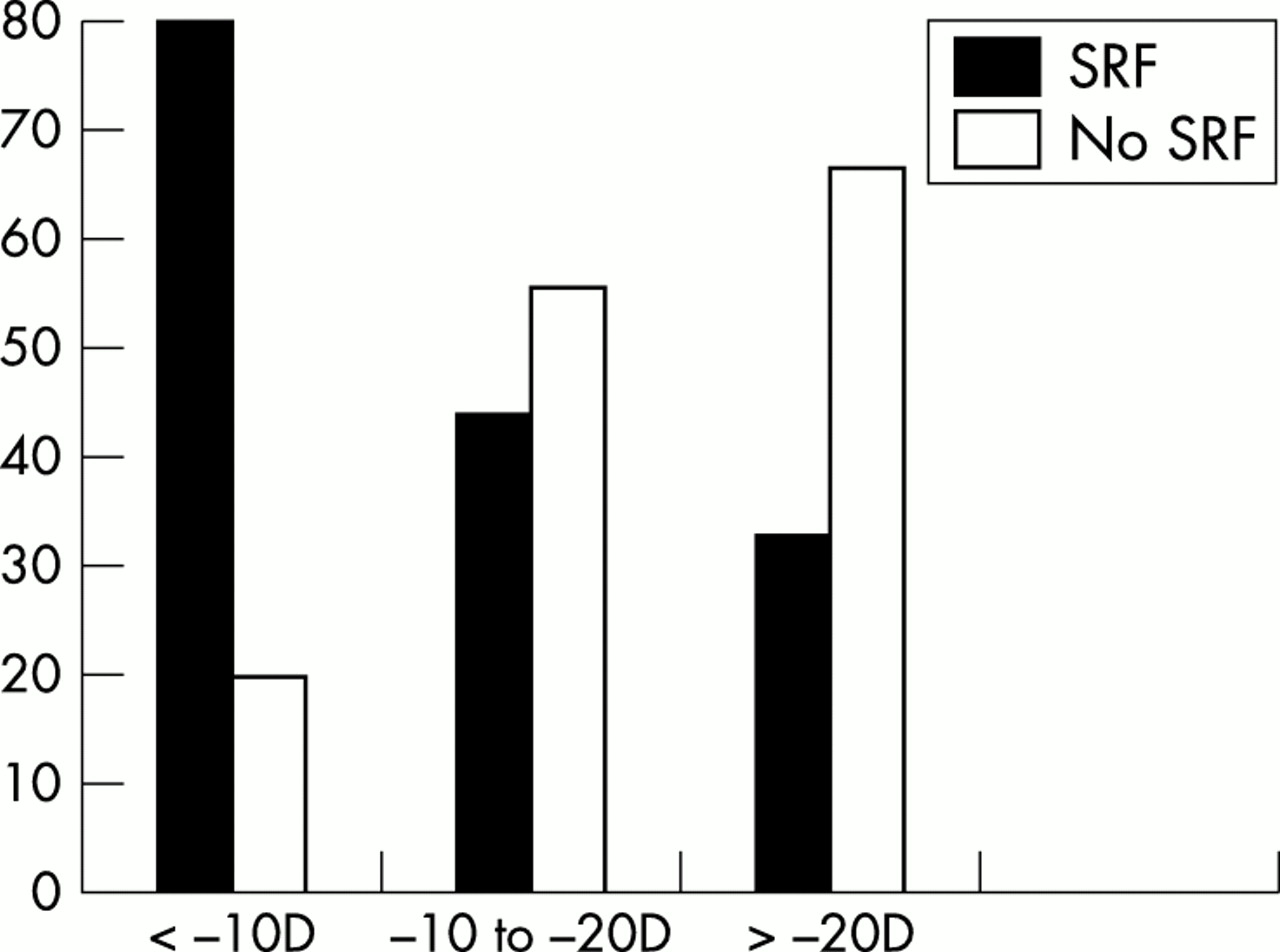
In five cases SE was unknown because of previous refractive surgery. Mean SE was −14.1 (5.3) dioptres (D) (range −4 to −28). SRF appeared in four of five eyes (80%) with a SE ≤ −10 D, in nine of 21 eyes (44%) with SE higher than −11 D (p= 0.003, χ2 test) (Fig 2).

Appearance of subretinal fibrosis (SRF) in relation to the spherical equivalent. SRF appears more frequently in myopic patients with SE under −10 D.
Mean CNV diameter at baseline was 1692 (783) μm. SRF appeared in two of 15 eyes (13%) with CNV ≤1500 μm, and in 12 of 16 (75%) with CNV >1500 μm (p=0.0001, χ2 test) (Fig 3).

Relation between subretinal fibrosis (SRF) and initial size of choroidal neovascularisation (CNV). SRF appears more frequently in patients with CNV greater than 1500 μm.
Chorioretinal atrophy was graded as M1-M2 in 19 eyes (61%) and as M3-M4 in 12 eyes (39%). SRF appeared in nine eyes with M1-M2 atrophy (47%) and in five eyes with M3-M4 atrophy (42%) (p= 0.41, χ2 test).
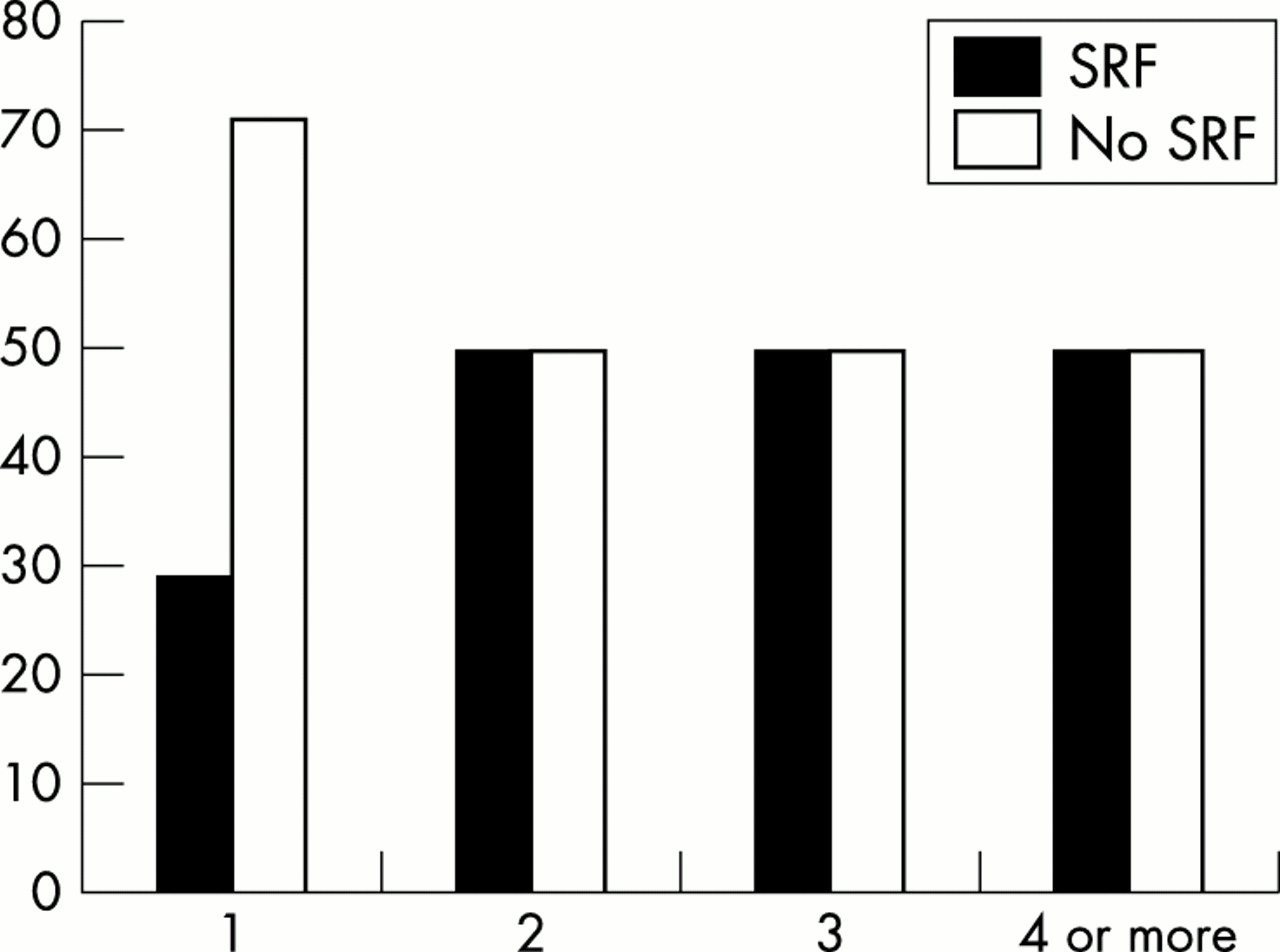
In seven eyes (22%) CNV was closed after only one session of PDT; meanwhile eight eyes (26%) needed two sessions, four eyes (13%) needed three sessions, and 12 eyes (39%) needed four or more sessions. SRF appeared in two cases (29%) among the eyes which needed only one session of PDT, in four cases (50%) of those which needed two sessions, in two cases (50%) of those which needed three sessions, and in six cases (50%) of those which needed four or more sessions (p= 0.61, χ2 test) (Fig 4).

Appearance of subretinal fibrosis (SRF) in relation to the number of photodynamic therapy (PDT) sessions required to close the choroidal neovascularisation. SRF is less frequent in patients with only one session of PDT.
Among the eyes with CNV ≤1500 μm, four eyes needed one session of PDT, three eyes needed two sessions, two eyes needed three sessions, and six eyes needed four or more sessions. Among the eyes with CNV >1500 μm, three eyes needed one session of PDT, five eyes needed two sessions, two eyes needed three sessions and six eyes needed four or more sessions.
A reactivation of the CNV was observed in eight eyes (26%). SRF appeared in four eyes (50%) of these, and in 10 eyes (43%) of those without reactivation (p= 0.41, χ2 test). Reactivation of the CNV appeared only in one eye with previous SRF (7%), and in seven eyes without previous SRF (41%).
BCVA at baseline was 0.17 (SD 0.15) (range 0.02–0.4) among patients who later developed SRF, and 0.25 (0.18) (range 0.02–0.6) among those who did not develop SRF. Final BCVA was 0.21 (0.17) (range 0.02–0.5) among patients who developed SRF, and 0.29 (0.19) (range 0.08–0.8) among those who did not develop SRF (p=0.45 for the group of SRF, and p=0.42 for the group without SRF, Student’s t test for paired data) (Fig 5).

Appearance of subretinal fibrosis (SRF) in relation to the visual outcome after treatment and 1 year follow up. SRF appears more frequently in patients with lower visual acuity.
In terms of improvement or loss of BCVA, the changes in BCVA are described in Table 1.
Evolution of best corrected visual acuity at the end of follow up in terms of ETDRS lines won or lost
BCVA at the end of follow up was <0.1 in six eyes (19%), 0.1 to 0.2 in nine eyes (29%) and >0.2 in 16 eyes (52%). SRF appeared in five eyes (83%) with BCVA <0.1, three eyes (33%) with BCVA 0.1 to 0.2 and six eyes (38%) with BCVA >0.2 (p= 0.0001, χ2 test) (Fig 5).
Case report
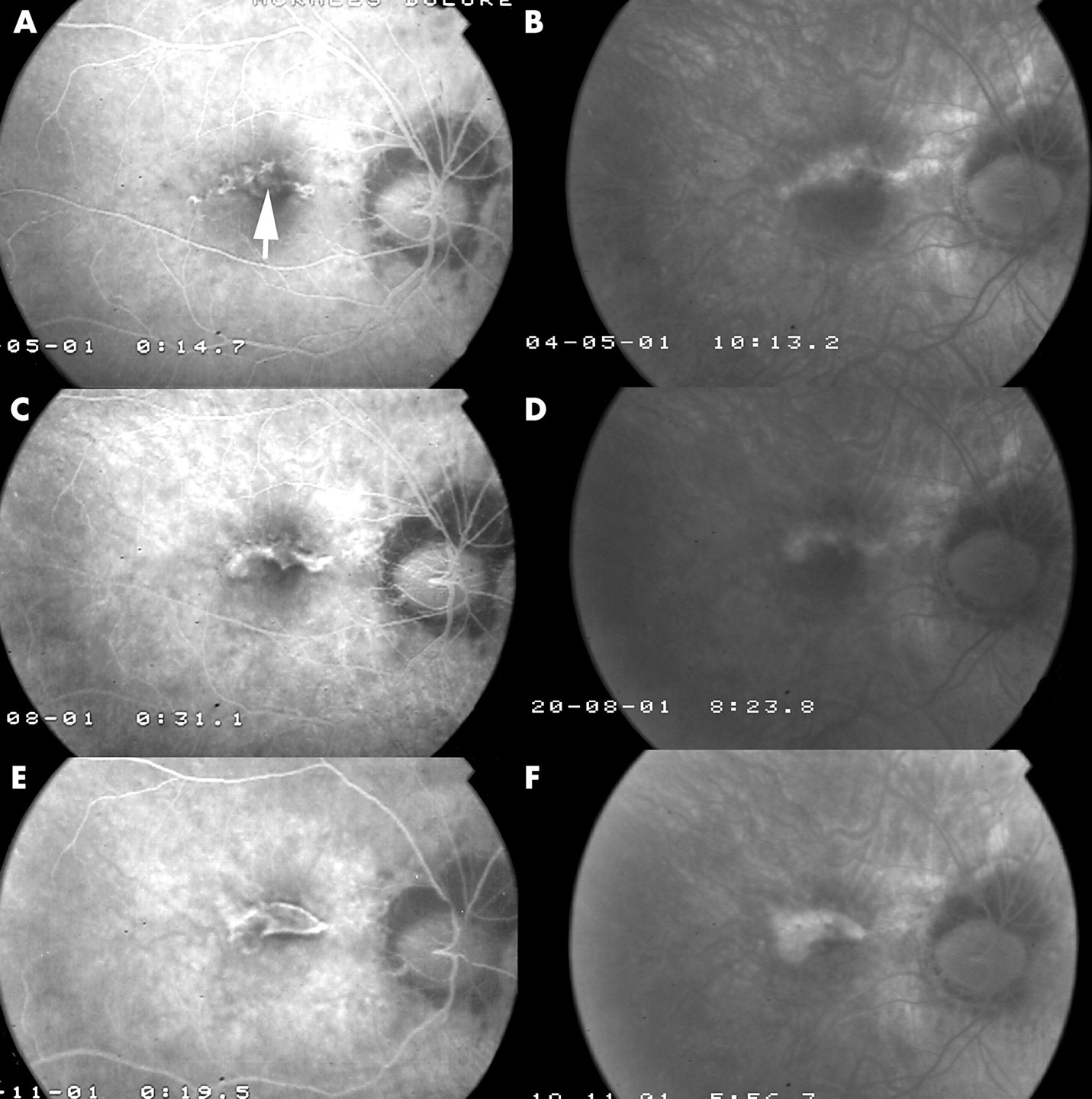
A 51 year old woman with a spherical equivalent of −8 D who had undergone successful LASIK 3 years earlier and previous BCVA visual acuity of 0.8, attended with a decreased BCVA of 0.4 in her right eye. She presented a M2 degree of chorioretinal atrophy. Fluorescein angiography was performed, which showed a subfoveal CNV (arrow, Fig 6A, B). PDT was performed and after 3 months BCVA was 0.3, and a complete closure of the CNV with SRF was observed (Fig 6C, D). At month 6 BCVA had decreased to 0.125 with a total closure of the CNV and an important fibrotic response (Fig 6E, F). No changes in visual acuity were noticed at months 9 and 12.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) and (B) Early and late fluorescein angiogram frames at baseline show subfoveal choroidal neovascularisation (CNV) (arrow). Best corrected visual acuity (BCVA) was 0.4. (C) and (D) After one session of PDT a fibrotic scar has taken the place of the CNV. BCVA was 0.3. (E) and (F) Early and late frames of angiogram after 6 months: the scar has grown bigger and visual acuity has decreased to 0.125.
DISCUSSION
SRF has been described after closure of macular CNV in myopic eyes, both spontaneously3 and after photocoagulation.9 What initially could be considered as a manifestation of the closure of the CNV, may turn into a possible serious complication, threatening visual outcome of these patients.
The purpose of the different therapeutic approaches which have been tried on myopic maculopathy, such as thermal laser photocoagulation,10,11 radiotherapy,5 surgery,12–16 and more recently PDT,6,7 is to reduce the exudation from the CNV and at the same time to produce a minimal scar so that visual acuity remains unaffected. Direct laser photocoagulation is subsequently no longer advisable for the treatment of subfoveal CNV in highly myopic eyes since it causes full thickness lesions of scar/atrophy in the retina which will later grow an average 109.2%.17 Surgical removal of the CNV causes minimal SRF but often induces loss in retinal pigment epithelium (RPE) cells. Radiotherapy has also been advocated for the treatment of myopic CNV without significant ocular or systemic adverse side effects, but the risk of malignancy in younger patients makes it unsuitable for this purpose.5 Verteporfin PDT has been approved for treating myopic CNV after the good results achieved by the VIP study and confirmed by our group.6,7
SRF has been previously described after PDT in highly myopic eyes,6,7 though it had been described as a good result meaning an absence of leakage and the closure of the CNV. Yet the appearance of SRF could be related to a worse visual prognosis. It may also be associated with an enlargement of the scar and a decrease in BCVA, as in the reported case.
In this study we have not considered a control group, since the data published by the VIP1 study proved the good results of PDT in treating highly myopic CNV, and we did not consider it ethically admissible to leave patients untreated.7
The occurrence of SRF may be variable depending on the association of different circumstances, such as age younger than 55 years (near significance, p=0.07, χ2 test), SE lower than −10 D, and the size of the CNV >1500 μm. We have found no association between the number of PDT sessions, the degree of chorioretinal atrophy, sex, or reactivation of CNV after closure.
Patients were divided in two groups by age in order to differentiate the possible influence of age related macular degeneration.18 Since degenerative changes at the posterior pole worsen with age19 the possibility of a strong fibrotic reaction could be expected to be lower in older patients, as has happened in our study. A higher occurrence of SRF, though not statistically significant, was observed in the group of patients aged 55 or less, probably related to the higher fibrotic reaction which usually appears in younger patients. This difference could be related to the age related systemic vascular atrophy.
Higher degrees of chorioretinal atrophy are related, according to Avila, to less aggressive forms of CNV (type V1) with a lesser degree of fluorescein leakage. Avila reported a more aggressive behaviour of CNV in patients with less atrophic fundus.3 We have found a need for a greater number of sessions of treatment in patients with less atrophic fundus, probably due to a healthier choriocapillary bed which could contribute to the reopening of the CNV after treatment, though there was no significant difference in the production of SRF.
CNV in our study has appeared most frequently among patients with spherical equivalent (SE) between −11 D and −20 D (58%). The mean SE was similar to those published in other series.7 SRF has been found to be more frequent among eyes with SE ≤ −10 D, though there was no relation with the degree of chorioretinal atrophy. Though it has been proposed that the mechanical stretching within the posterior pole in highly myopic eyes may play a part in the production and following expansion of macular SRF after laser treatments19 we have found it to be higher in patients with a SE less than −10 D.
We have found a clear relation between the size of the CNV at baseline and the production of SRF after PDT. Hampton reported an inverse relation between BCVA and the size of the neovascular complex.20 In our study CNVs larger than 1500 μm in diameter at baseline seem to have a greater risk of developing SRF. It can be assumed that greater CNVs could be associated with greater leakage of cicatricial components from the blood stream and thus develop greater scars when they close.
Among eight cases of reactivation of CNV, only one case happened in an eye with SRF, and seven in eyes without SRF, though three of these later developed SRF. This finding could suggest that SRF might have a certain role of protection against reactivation of CNV, owing to the development of a scar that would inhibit the further growth of vessels under the retina.
The relation of SRF to the number of PDT sessions could be the manifestation of subclinical laser damage, as described for thermal laser photocoagulation.21 This phenomenon has been described by some authors to be independent of the wavelength of the laser.22 The number of sessions of PDT required does not seem to be related, as it might be primarily thought, to the original size of the CNV.
BCVA has shown improvement after PDT treatment in cases which later developed SRF, though this was not statistically significant. Yet the presence of SRF was more frequent in the eyes which showed a lower final BCVA.
Among other therapeutic approaches only foveal translocation has shown good results in terms of BCVA and lack of SRF.15 Yet, this technique is not only difficult to perform, making it unavailable for most of patients, but also presents a number of complications such as retinal detachments, epiretinal membranes, and macular holes.23
In spite of the good results in terms of BCVA and CNV closure in highly myopic patients treated with verteporfin PDT, especially in patients under 56 years of age, and with lower degrees of chorioretinal atrophy, it must be borne in mind that SRF may appear. This has been found to appear more often in patients aged under 56 years, with SE equal or less than −10 D, and eyes with CNV greater than 1500 μm.
The appearance of SRF after PDT in highly myopic CNV does not always imply a loss of BCVA from baseline, though its presence is more frequent in eyes with lower BCVA. Owing to the short time that elapsed since PDT has been approved in the treatment of subfoveal CNV in highly myopic patients, the final visual outcome of eyes with SRF is not predictable. Longer follow up studies are required in order to determinate its influence on their anatomical and visual outcome.