Article Text

Abstract
Aims: To determine the visual outcome and prevalence of amblyogenic risk factors in children with craniosynostotic syndromes.
Methods: The case notes of 141 children seen within the craniofacial unit were reviewed and information retrieved on date of birth, age at first and last examination, cycloplegic refraction at last visit, best corrected visual acuity at last visit, horizontal ocular deviation in primary position at first visit, and alphabet pattern if any. The presence of astigmatism, its magnitude, and orientation of axis were determined.
Results: 40.3% of patients had 1 dioptre (D) of astigmatism or greater and, of these, 64% had oblique astigmatism in at least one eye. Anisometropia of 1D or more was found in 18% of patients (age matched normals 3.5%). Horizontal strabismus was found in 70% (38% exotropia, 32% esotropia). Visual outcome results showed 39.8% of patients (45 of 113) had visual acuity of 6/12 or worse in their better eye.
Conclusion: In the largest study to date a poor visual outcome was shown in children with Crouzon’s, Pfeiffer’s, Apert’s, and Saethre-Chotzen syndromes (39.8% with 6/12 or worse in the better eye) together with significant prevalence of amblyogenic risk factors.
- craniosynostosis
- amblyopia
- astigmatism
- children
Statistics from Altmetric.com
Craniosynostosis, the premature fusion of one or more of the cranial sutures, is the most common human congenital skull defect, with a prevalence of 333–476 per million births.1 It frequently occurs with other anomalies of differentiation of bone, particularly of the hands and feet.2 Over 100 syndromes with craniosynostosis have been described,3,4 and these include the autosomal dominant syndromes of Apert, Crouzon, Pfeiffer, and Saethre-Chotzen.
Although visual loss has been documented in these cases and attributed to optic neuropathy (due to chronic papilloedema), amblyopia or exposure keratopathy, or a combination of all three,5–9 there are no studies which demonstrate the degree of visual loss in syndromic craniosynostoses.
The purpose of this study was to establish the visual outcome in children with Crouzon’s, Pfeiffer’s, Apert’s, and Saethre-Chotzen syndromes, and to determine the presence of any amblyogenic factors.
METHOD
The case notes of 141 children with a confirmed diagnosis of Apert, Crouzon, Pfeiffer, and Saethre-Chotzen were reviewed retrospectively. All patients had attended the craniofacial unit at Great Ormond Street Hospital for Children between October 1979 and October 2000. The following data were extracted from the notes: date of birth, age at first and last examination, cycloplegic refraction at last visit, best corrected visual acuity at last visit, horizontal ocular deviation in primary position at first visit, and alphabet pattern.
All refraction data were looked at for right and left eyes independently, and spherical equivalent values were also calculated. In looking at visual acuity data, we looked at visual outcome in right and left eyes, but also in patients’ better and worse eyes. Visual acuity was tested by means appropriate to age and cognition and then recorded as Snellen or Snellen equivalent.
Not all sets of data for all 141 patients were suitable for use in all parts of the study. From the notes available, 92 contained all data required for all fields, 112 notes contained all age data, 113 notes contained all visual acuity data, and 139 notes contained all the refraction data needed. In recording the presence and axis of any astigmatism, it was necessary in some cases to estimate the orientation of the axis from diagrams representing the retinoscopy power-cross in the notes.
In determining the incidence of oblique as opposed to “rule obeying” astigmatism, we took horizontal axis readings of between 175 and 5 degrees inclusively and vertical axis readings between 85 and 95 degrees inclusively to be “rule obeying.” All axis readings outside these figures were considered to be oblique for the purposes of this study, in accordance with the criteria of Denis et al.10
Any child who was found to be amblyopic, either unilaterally or bilaterally, underwent at least a trial of occlusion therapy in accordance with our clinical practice.
Any patients who had undergone craniofacial or strabismus surgery before initial presentation were excluded from the study.
RESULTS
The mean age at presentation to the department of ophthalmology at Great Ormond Street Hospital for Children was 23.3 months (SD 38.3; range 0.6–278.3; median 8.9) with the mean age at last follow up being 76.3 months (SD 56.3; range 5.8 – 287.6; median 65.6).
A total of 40.3% of patients had 1 dioptre (D) of astigmatism or greater in either their left or right eyes (see Fig 1). Within the individual syndromes, these figures break down in right and left eyes, respectively, to 31.7% and 28.6% for Saethre-Chotzen (mean 30.2), 50.0% and 54.8% for Apert’s (mean 52.4), 46.7% and 40.0% for Crouzon’s (mean 43.4), and 42.1% and 47.4 % for Pfeiffer’s syndrome (mean 44.8).

Overall incidence of astigmatism in the craniosynostotic syndromes.
Within the groups of patients who exhibited astigmatism of any magnitude, 64% had oblique astigmatism in at least one eye, which is equivalent to 48.5% of the overall population studied.
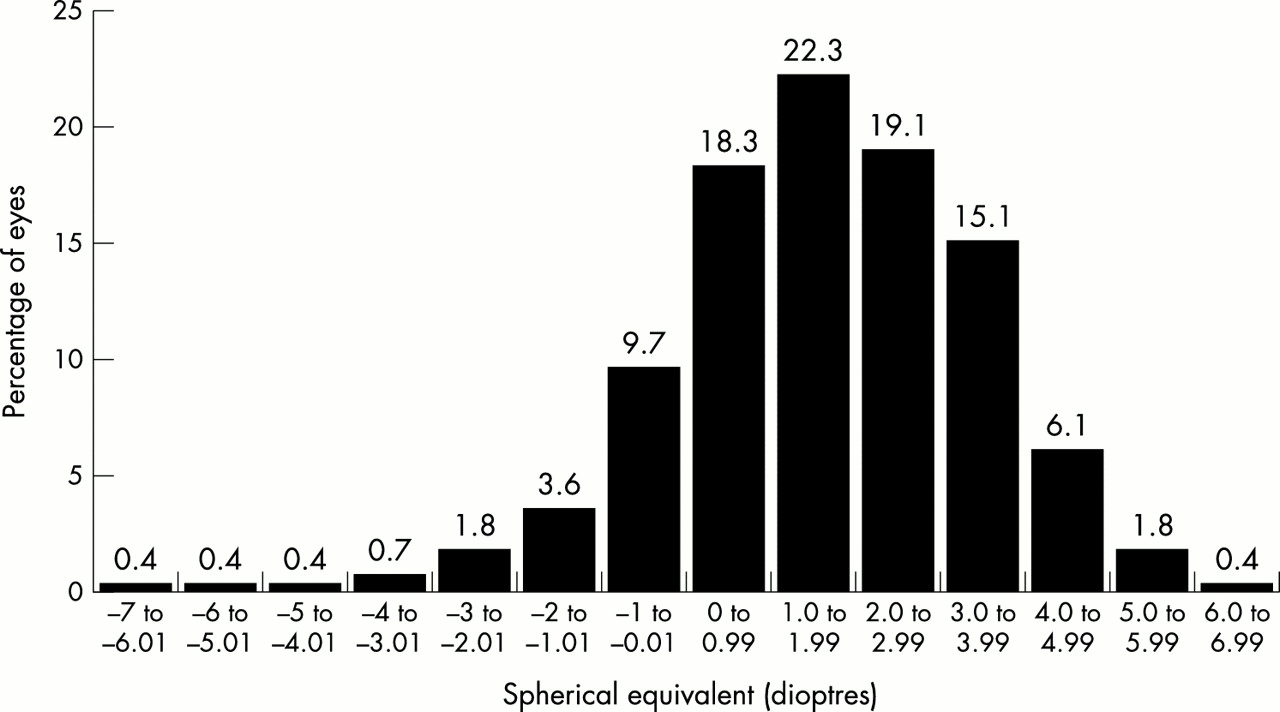
Spherical equivalents follow a normal distribution with a mean and mode between +1 and +2 dioptres (see Fig 2). If the differences between spherical equivalents for individual patients are examined, 18% of patients are shown to have more than 1 dioptre of anisometropia (see Fig 3).
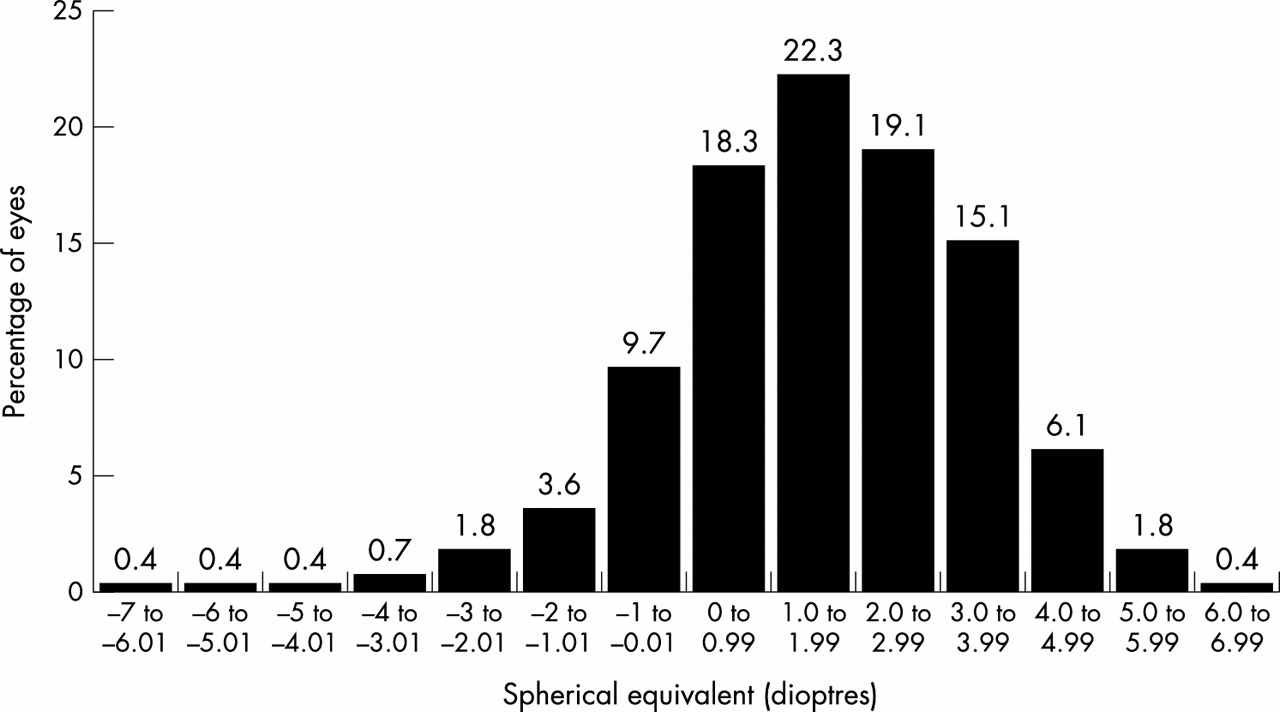
Spherical equivalents for craniosynostotic syndromes. Percentages of eyes.
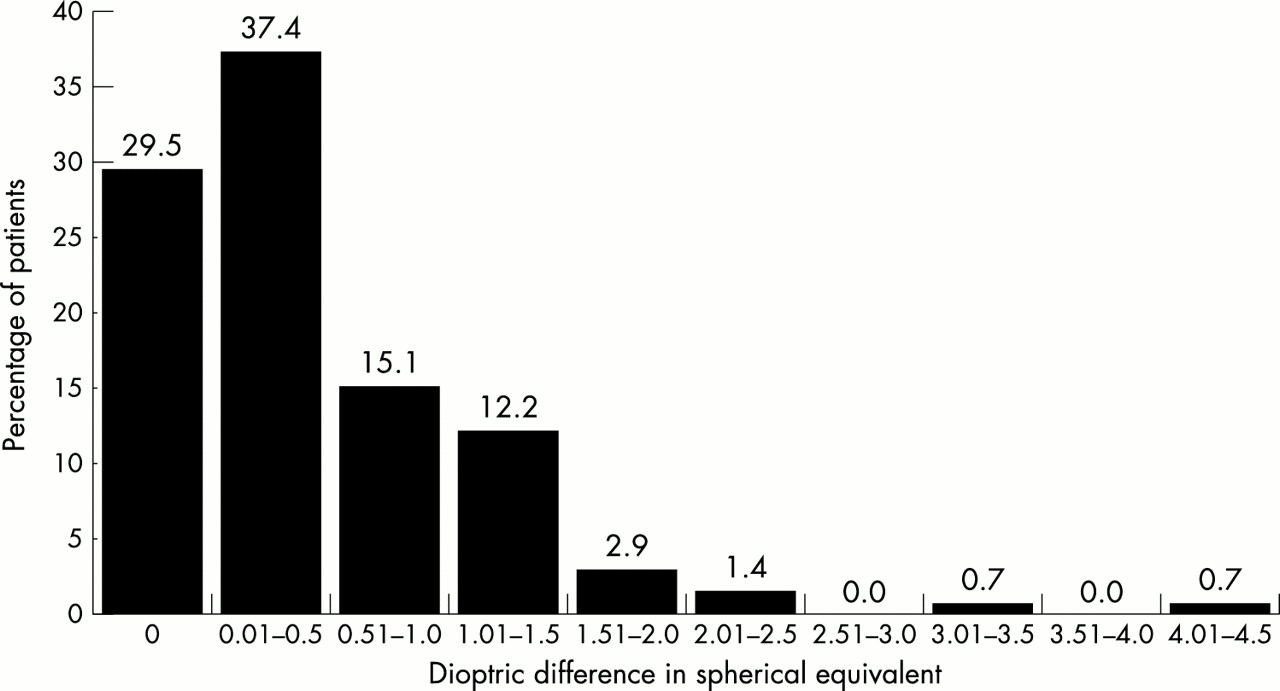
Difference in equivalents for the craniosynostotic syndromes.
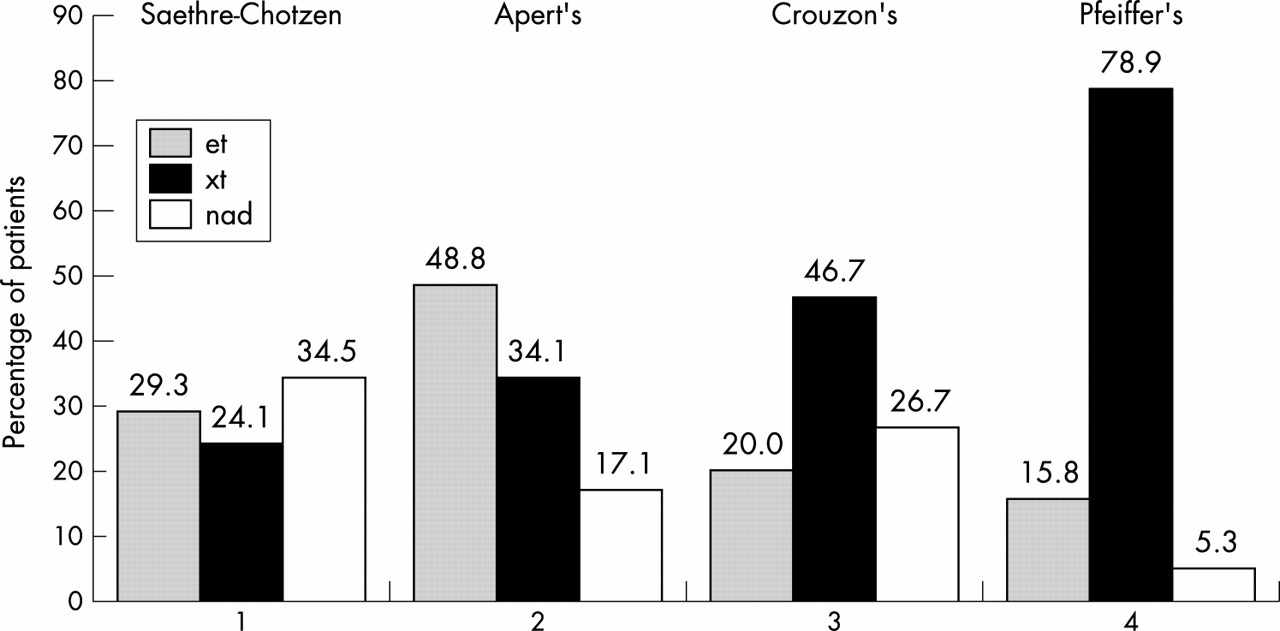
Overall, 38% of patients presented with an exotropia in primary position, 32% with esotropia, 24% were straight in the primary position, and 6% were noted to have a vertical deviation only. By syndrome, Apert presented with more esotropia than exotropia, while the reverse was true for Crouzon and Pfeiffer. There was no significant difference in the incidence of either esotropia or exotropia in Saethre-Chotzen syndrome (see Fig 4).
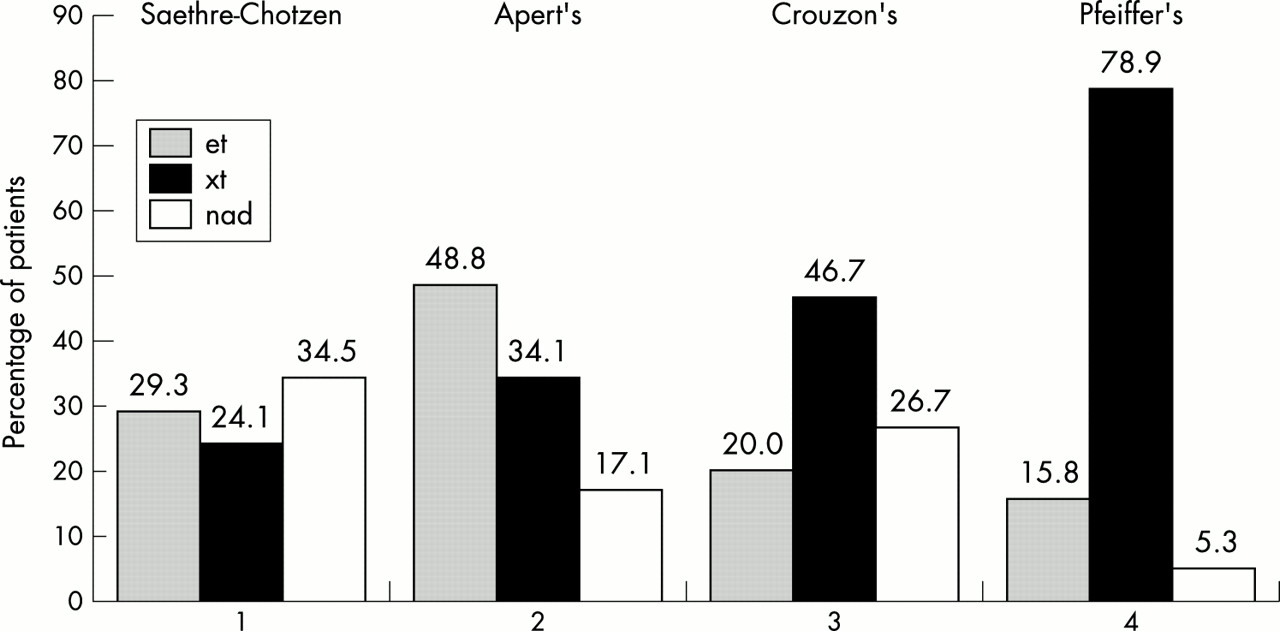
Strabismus in primary position at initial presentation for the craniosynostotic syndromes.
A total of 62 of the 141 patients (44.0%) were noted to have an alphabet pattern, of which 95% showed a “V” pattern as opposed to an “A” (Saethre-Chotzen 75%, Pfeiffer 93%, Apert 97%, and Crouzon 100%).
In all, 52% of eyes (118 of 226) had Snellen (or equivalent) visual acuities of 6/12 or worse (46% of right eyes (52/113) and 58.4% of left eyes (66/113)). Furthermore, 39.8% of patients (45 of 113) had visual acuity of 6/12 or worse in their better eye, while 64.6% of patients (73 of 113) had 6/12 or worse in at least one of their eyes (see Fig 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Overall visual acuities in the craniosynostotic syndromes.
DISCUSSION
The syndromic craniosynostoses are rare. Nevertheless, there are over 100 described syndromic synostoses, the most common of which include Pfeiffer, Crouzon, Apert, and Saethre-Chotzen.3,4 It is therefore these syndromes that we have chosen to review in this study.
Crouzon’s and Apert’s syndromes both occur with a frequency of approximately 15–16 per million births. Apert’s accounts for about 4.5% of all cases of craniosynostosis. The exact incidence of Pfeiffer’s syndrome is unknown, but is estimated to be between 16 and 40 per million births.5
Characteristically, Apert’s syndrome has craniosynostosis associated with midface hypoplasia and severe symmetric syndactyly of the hands and feet. Crouzon’s shows orbital proptosis, hypertelorism and maxillary hypoplasia, while children with Pfeiffer’s syndrome have broad thumbs and toes. Saethre-Chotzen syndrome has a broader spectrum of manifestations including flat forehead, ptosis, and milder syndactyly.
Astigmatism in unicoronal synostosis has previously been reported,10,11 and there is also one previous report of astigmatism in Apert’s, Crouzon’s, and a mixture of other craniofacial synostoses.12 However, the authors do not identify the ages of patients when their visual acuity and refraction were recorded, which is pertinent as it is a well established fact that young infants have high levels of astigmatism which regress with time because of emmetropisation.6 The authors further conclude that the major reason for loss of vision in their group, and craniosynostosis overall, was amblyopia alone, as there was absence of structural and neurological abnormalities. However, recent work has shown that even in the absence of any signs of raised intracranial pressure (ICP) or optic nerve changes, the visually evoked potential (VEP) may be pathologically degraded in craniosynostosis.13,14 This is also our personal experience even when the amblyogenic factors are accounted for, and so we feel that in the absence of electrodiagnostic testing of such children, it is not possible to attribute all the visual loss to amblyopia alone.
Within our study, we interpreted 1D of astigmatism as clinically significant, in keeping both with our clinical practice and also with previous reports that consider less than 1D of astigmatism to be normal.6,15 For the mean ages of the groups, which range from 27.1 months (2 years 3 months) to 96.1 months (8.0 years), there are variable statistics in the literature as to the prevalence of astigmatism in the normal population. This ranges from 2.3% to 30% at 2–3 years old16,17 and 6% to 18% at 8 years of age.18,19 However, even if we use the higher figures for the purpose of comparison with the results from our study, our finding of 40.3% prevalence of 1D or greater astigmatism in the syndromic craniosynostoses, with a range from 28.6% to 54.8%, is higher than the values expected in age matched normal children. The astigmatism is likely to be the result of several factors including corneal distortion secondary to exposure keratopathy, ptosis, and even the shape of the orbits.
In comparing the proportional incidence of oblique v regular astigmatism, we used the criteria of Denis et al11 to define “rule obeying” astigmatism as having axes 175–5 degrees for the horizontal, and 85–95 degrees for the vertical, with all axes outside this range being classified as oblique. The prevalence of oblique astigmatism in at least one eye of 48.5% (64% of patients with astigmatism) of patients within our group is again higher than the figures quoted in the literature for the normal population, which varies from 0% to 40% for ages ranging from 1.5 to 12 years of age.19–21
These findings have important implications with regard to the risk of the development of meridional amblyopia, as previous studies have identified both large amounts of astigmatism and oblique astigmatism as high risk factors for amblyopia in the normal population.22,23
Although it is our clinical practice to treat anisometropia of 1D or greater, we have quoted figures for greater than 1D so as to enable a more accurate comparison with the “normal” figures available in the literature. The spherical equivalents in this group have a normal distribution around a mean of +1D to +2D, which is considered to be normal for children between neonatal age and 10 years old.24,25 However, with 18% of our group having more than 1D of anisometropia compared to an incidence of 3.5% for normal children between 4 and 12 years old,26 the possible contribution of anisometropia to the development of amblyopia cannot be disregarded.
The presence of strabismus in the primary position is also another amblyogenic risk factor. To the best of our knowledge, there has only been one previous report of the higher prevalence of esotropia in Apert’s syndrome,27 which we have again shown in this study. Although we only recorded 6% of patients to have vertical deviation in the primary position we feel that this is probably a gross underestimation of the true value because these children can be very difficult to examine, and in the presence of a horizontal deviation a small vertical component can be very difficult to accurately detect and measure. Alphabet pattern analysis in this group of patients confirmed that the majority of these patients will display a V exotropia pattern, which in itself is a well established fact.28
In assessing the practical visual outcome for these patients, we wanted to know what proportion of these patients would not reach the visual standard for driving in the United Kingdom. We used corrected Snellen 6/10 acuity as a representation of the basic legal requirement for an individual to be allowed to drive in the United Kingdom.29 However, as this is not a standard level of acuity tested, we looked at the numbers of eyes and patients in our group that did not reach this standard of vision: 39.8% of patients had 6/12 acuity or worse in their better eye, and an even larger 64.6% had 6/12 or worse in at least one eye, which suggests that visual morbidity is significant in these children.
Although the potential influence of refractive development on the incidence of amblyogenic refractive factors cannot be disregarded, we did not look at refractive error at presentation as we were interested in the outcome/end data and, ultimately, refractive errors at presentation will not have a direct correlation with the outcome results.
It is not possible from this study to determine what proportion of the visual loss demonstrated was from amblyopia or optic neuropathy, or indeed a combination of the two, but it does draw attention to the fact that the visual loss is likely to be multifactorial. Amblyopia is amenable to occlusion or penalisation therapy, but the sooner amblyopia is discovered the greater the opportunity to treat it. The mean age at presentation to the department of ophthalmology at Great Ormond Street Hospital for Children was 23.3 months (SD 38.8). This may be attributable to the following reasons. Firstly, as Great Ormond Street Hospital for Children is a tertiary referral centre, the patients may have been seen earlier by a local ophthalmologist. Secondly, their general systemic condition may have prevented earlier attendance. Thirdly, the craniofacial surgeons may not have perceived there to be an ophthalmic problem since their main concern, quite rightly, is visual loss caused by raised intracranial pressure. Consequently, the early referral of such children, regardless of the presence of any ophthalmic symptoms/signs, is something that should be encouraged.
In undertaking this study, and in particular because of its retrospective nature, there were a number of difficulties encountered. Not all sets of data for all 141 patients were suitable for use in all parts of the study. Overall, 92 patients’ notes contained all data required for all fields, 112 notes contained all age data, 112 notes contained all visual acuity data, and 139 notes contained all the refraction data needed. However, the syndromic craniosynostoses as a group are rare, and although we have displayed all results as a percentage of each subset studied, we feel that the numbers within each group are sufficiently large given the rarity of the conditions being discussed.
Vision testing was by methods appropriate to age and cognitive abilities of the individual children, the majority being based on uncrowded tests and thus themselves providing another potential source of underestimation of the true incidence of amblyopia. Occlusion therapy or at least a trial of occlusion therapy was recorded for all children noted to be amblyopic, but it was not consistently noted if it was stopped for non-compliance or lack of visual improvement.
In retrieving refraction data from the notes, it was necessary in some cases to interpret the axes from retinoscopy power-cross drawings, where the axes had not been clearly labelled. In general this resulted in more “regular” axes than “oblique,” and may in fact have diluted the true incidence of oblique astigmatism found in this study.
Children with syndromic craniosynostoses have multiple problems that can include breathing difficulties, speech difficulties, and developmental delay, which can make them very difficult to examine.5,30 The presence of exposure keratopathy, no matter how mild, can make them photophobic and intolerant of any examination light, including that of a retinoscope. Despite this it is still usually possible to refract them in an outpatient setting if the examiner is prepared to be patient and flexible in technique. Adequate cycloplegia is an absolute must and, as we have shown a high incidence of astigmatism and consequent risk of visual impairment, it is essential that the ophthalmologist consider an examination under anaesthetic if adequate assessment is not possible in the outpatient clinic despite several attempts.
In the largest study of its kind to date (to the best of our knowledge) of syndromic craniosynostosis visual outcome we have demonstrated a poor visual outcome with an acuity of 6/12 Snellen or worse in the better eye in 39.8% of cases, while 64.6% of cases had this level of vision or worse in either eye. The increased risk of amblyopia in these children compared to published age matched normals has been demonstrated by showing significant astigmatism (40.3%), oblique astigmatism (48.5%), and strabismus (75.9%).
We have also shown a higher incidence of esotropia in Apert’s syndrome, which to the best of our knowledge has only been reported once before.
We have not determined exactly how much optic neuropathy may have contributed to the final vision in some cases, but we have shown that the visual loss is likely to be multifactorial. The effect of amblyopia must be recognised early to allow maximal chances for visual rehabilitation.