Article Text

Abstract
Background/aim: The Republic of Ireland has a centralised database of all registered, blind people in the country. The last study of the national blind register was undertaken in 1996. The current study sought, firstly, to investigate and identify any recent changes in the register composition. Secondly, there is concern that many eligible people are not appropriately registered. To examine this further, registration levels among patients attending an Irish outpatient ophthalmology clinic were determined.
Methods: Criteria for blind registration in Ireland are (1) a best corrected visual acuity of 6/60 or less in the better eye, or (2) a visual field subtending an angle of 20 degrees or less. The National Council for the Blind in Ireland (NCBI) is the sole custodian of a national registration database recording all eligible, registered people. This computerised database was analysed to provide information on the demographics and blind registration condition of those on the register in 2003. This information was compared with the results of the 1996 study. To assess the accuracy of the current register, the registration status of eligible patients attending the outpatient clinic of a busy, tertiary referral ophthalmology department, over a 9 week period, was studied.
Results: 6862 adults were registered as blind on the NCBI register in Ireland in 2003, representing an increase of 37% since 1996. The leading causes of registration were age related macular degeneration (ARMD) (25%), glaucoma (12%), and retinitis pigmentosa (7%). Comparing the 1996 and 2003 data, dramatic increases in the numbers registered caused by ARMD (from 812 to 1729 people, a 113% increase) and diabetic retinopathy (DR) (from 147 people to 323 people, a 120% increase) were found. The numbers registered as a result of glaucoma were relatively stable (795 in 1996 and 811 in 2003). A substantial drop, of 53%, was noted in the number of people registered as a result of cataracts, from 561 people to 261. Of the 672 new cases registered in 2003, ARMD accounted for 44%, glaucoma 13%, and DR 7%. Over the 9 week study period 75 patients, out of a total 2320 patients who attended the outpatient department, fulfilled the blind registration criteria. It was found that 21% (16 of 75) of the eligible clinic outpatients had not been appropriately registered.
Conclusion: An overall increase in adult blind registration of 37% in the Republic of Ireland was found between 1996 and 2003. There were large increases in registered blindness as a result of ARMD (113%) and DR (120%). A notable decrease in registration as a result of cataracts was discovered. Vigilance by clinicians is necessary to ensure that eligible patients are registered.
- ARMD, age related macular degeneration
- DR, diabetic retinopathy
- NCBI, National Council for the Blind in Ireland
- blind registration
- Ireland
- ARMD, age related macular degeneration
- DR, diabetic retinopathy
- NCBI, National Council for the Blind in Ireland
- blind registration
- Ireland
Statistics from Altmetric.com
- ARMD, age related macular degeneration
- DR, diabetic retinopathy
- NCBI, National Council for the Blind in Ireland
- blind registration
- Ireland
- ARMD, age related macular degeneration
- DR, diabetic retinopathy
- NCBI, National Council for the Blind in Ireland
- blind registration
- Ireland
The World Health Organization (WHO), which estimated in 2002 that there were 37 million blind people worldwide, encourages all countries to monitor the magnitude and causes of visual impairment in order to scrutinise and eliminate avoidable blindness.1 Uniquely in Europe, the Republic of Ireland has a centralised, national database of registered, blind people in the country. In Ireland, in order to be deemed legally “blind,” an individual must be shown by an ophthalmologist to have a (1) visual acuity of 6/60 or less in the better eye or (2) a visual field restricted to 20 degrees or less. Eligible patients should be registered blind with the NCBI by the assessing ophthalmologist. It should be noted that there is no “partial sight” registration available in Ireland. Although registration is entirely voluntary, it confers significant practical and monetary benefits.
The last study of the national register was performed in 1996.2 It showed that 5002 adults (aged 16 years and over) were registered blind in the country at that time. The most common causes of blindness in 1996 were macular degeneration and glaucoma, each responsible for 16% of registrations, and cataract, which accounted for 11% of those on the register. This study wished to assess the impact of an ageing population and medical advances on the numbers of adults registered blind and their reasons for registration.
Although registers provide a valuable source of information regarding blindness, unfortunately, not all those who are eligible are indeed registered. Previous studies have examined the registration rates in an English hospital setting.3–5 They found that 45–60% of eligible patients attending clinics were not registered. The situation regarding registration in Irish clinics was unknown before this study.
METHODS
Information recorded on the NCBI register includes patient demographics and blind registration condition. The database is “live” and only records the details of those currently on the register. The 2003 data were reclassified in accordance with the previous 1996 study, as regards age groupings and diagnostic categories. The differences between the data from 1996 and 2003 were then analysed.
An additional study based at the Mater Hospital, which has a busy tertiary referral ophthalmology department, was performed. Clinics were attended for a 9 week period between January and March 2004. The registration status of all eligible patients was ascertained. Patient demographics, blind registration condition, and reasons for non-registration were recorded. The patient’s primary ophthalmic disease was classified as being permanent requiring ongoing treatment, permanent not requiring ongoing treatment, or temporary. This classification followed that used by Bunce et al.5
RESULTS
The number of people on the blind register increased from 5002 in 1996 to 6862 in 2003 (table 1). Substantial changes in the reasons for registration were also noted over the past 7 years. The leading causes of registration were age related macular degeneration (ARMD) (25%), glaucoma (12%), and retinitis pigmentosa (7%). Comparing the 1996 and 2003 data, dramatic increases in the numbers registered caused by ARMD (from 812 to 1729 people, a 113% increase) and diabetic retinopathy (DR) (from 147 to 323 people, a 120% increase) were found (fig 1). The numbers registered as a result of glaucoma were relatively stable (795 in 1996 and 811 in 2003). A substantial drop, of 53%, was noted in the number of people registered as a result of cataracts, from 561 people to 261.
Prevalence of blindness among adults on the Irish blind register

Prevalence of blindness among Irish adults on the Irish Blind Register.
In terms of the numbers registered/100 000 adults, overall there was an increase in blind registration from 178/100 000 adults to 227/100 000 adults in Ireland between 1996 and 2003 (table 1). ARMD was responsible for blind registration in 29/100 000 adults in 1996; by 2003 this had increased to 57/100 000 adults. Likewise, DR as a cause of blind registration increased from 5/100 000 adults to 11/100 000 adults. Glaucoma showed a minimal decrease as a cause of registered blindness from 28/100 000 adults in 1996 to 27/100 000 adults in 2003. Cataract, as a cause of blind registration, decreased substantially from 20/100 000 adults in 1996 to 9/100 000 adults in 2003.
In all, 56.4% of those on the blind register were over 65 years of age. While the number of over-65s in the country has increased by 5% between 1996 and 2002 (from 413 882 to 436 001 according to census figures from those years), the number of such people on the register has increased by 36%.6,7 In particular, the number of registrees of 80 years and over has increased by 55% over the last 7 years.
The most common indications for new registrations in 2003 (n = 672) were macular degeneration (44.2%, 9.8/100 000 adults), glaucoma (13.2%, 2.9/100 000 adults), and DR (7.0%, 1.6/100 000 adults) (table 2, fig 2); 75% of the new referrals were aged 65 years and over and 61% were female.
Incidence of blindness among adults on the Irish register in 2003
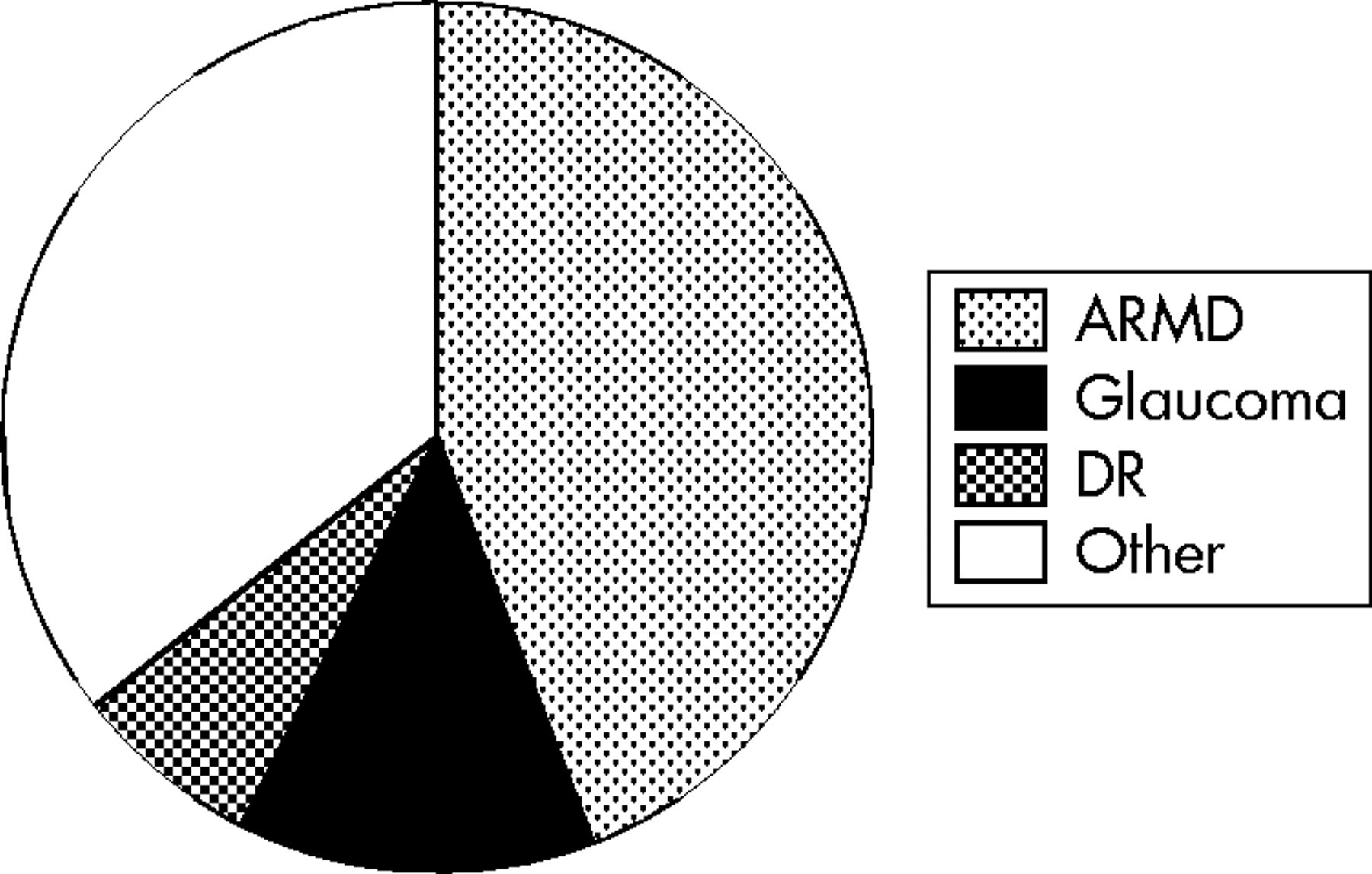
Incidence of blindness among Irish adults on the Irish Register 2003 (n = 672).
In all, 75 (3.2%) of the 2320 patients attending the outpatient clinic during the study period were identified as fulfilling the blind registration criteria. The majority of registerable patients were female (n = 43, 57%); 53 patients (71%) were aged 65 years and over. Only five patients (6.7%) were eligible for registration based on their visual fields alone.
A total 32 (43%) of the 75 people eligible for registration were already registered as blind (fig 3). Reasons for non-registration among the remaining 43 patients (57%) were (a) patient was new to the clinic or was an existing patient with recent visual deterioration: 19 patients (25%); (b) patient had not been made aware that they were eligible for registration and/or had not been registered by their ophthalmologist with the NCBI: 16 patients (21%); (c) patient was undergoing treatment with good prognosis: 7 patients (9%); (d) patient had refused registration: 1 patient (1%). Therefore, only 16 patients (21%) had no reasonable grounds for not being registered.

Registration status among eligible clinic outpatients.
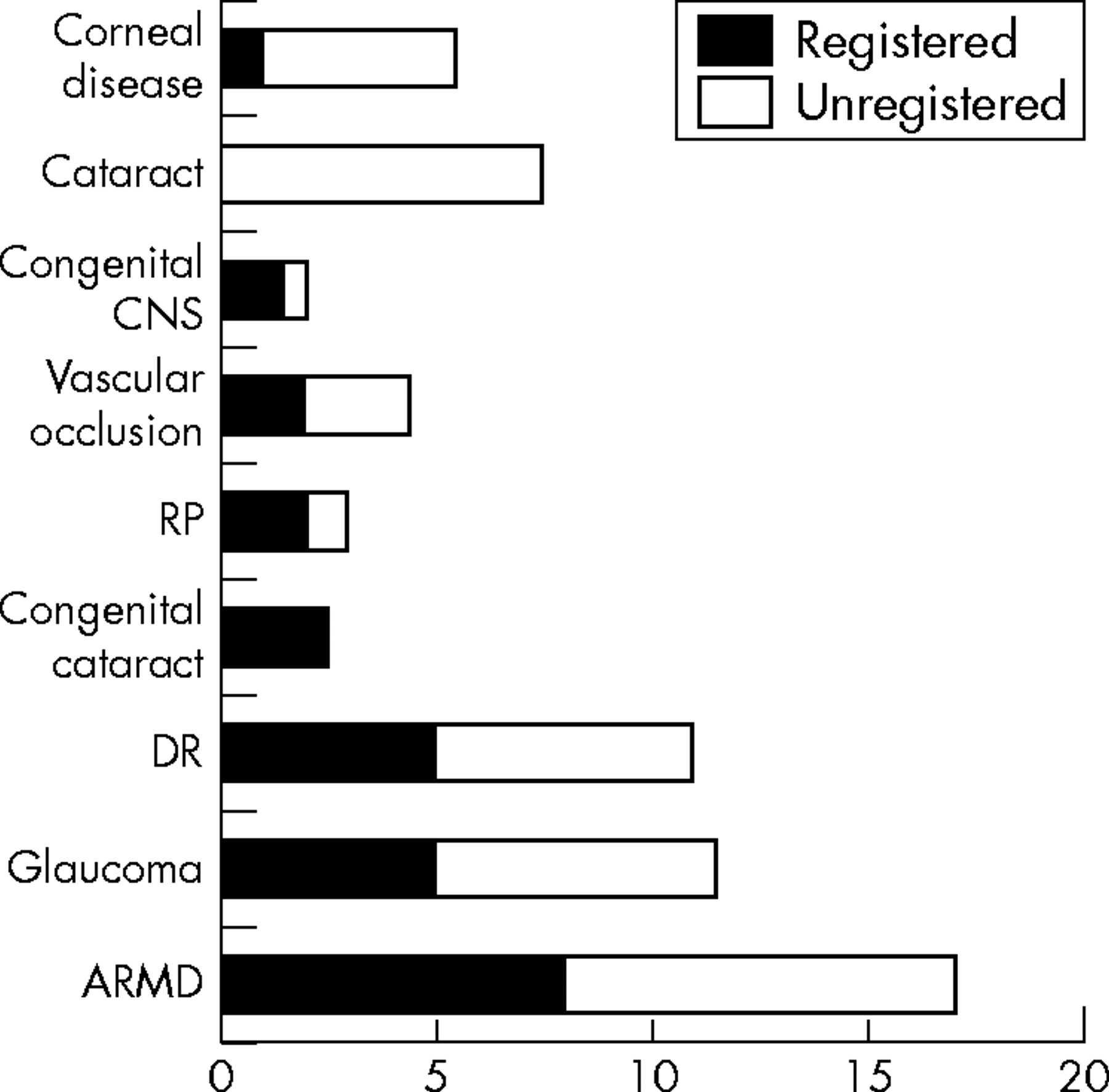
When examining risk factors for non-registration (n = 43), it was found that those over 65 years were more likely to be unregistered (p<0.01, χ2 test) (table 3). This occurred even though only 11% (eight of 53) had a reversible cause of blindness. It was also found that those with temporary conditions—for example, cataracts, were, appropriately, less likely to be registered (p<0.001). Sex and ongoing treatment were not found to contribute to non-registration. It was found that those with congenital cataracts were more likely to be registered (p<0.05) and those with corneal disease and cataracts were less likely to be registered (p<0.05, p<0.001) (fig 4). This was in keeping with the likelihood of visual recovery in these conditions. No other condition was linked with an increase or decrease in likelihood of registration.
Risk factors for registration/non-registration among clinic patients
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Causative condition among registered and unregistered outpatients.
DISCUSSION
The number of adults registered blind in the Republic of Ireland has increased by over 37% since 1996. In contrast, the population of the country increased by approximately 8% between 1996 and 2002.6,7 Currently, the overall prevalence of blind registration in the population is 227/100 000 adults. The annual incidence of 22/100 000 adults is lower than in a recent Scottish study (combined incidence 31/100 000 adults for blind and partial sight registration), possibly as a result of the lack of “partial sight” registration in this country.8
As expected, blind registration increases sharply with age; 56% of those on the Irish register are over 65 years of age and 75% of new registrations in 2003 were aged over 65 years. People 65 years and over account for 77% of the newly registered in Scotland and 76% of those in Germany.8,9 As stated previously, there has been a disproportionate increase in the number of elderly on the register over the last 7 years. Owing to the short time period involved, most of this increase is likely to represent increased registration rather than increasing levels of disease.
Macular degeneration has increased dramatically in overall prevalence as a cause of blindness. It is the leading prevalent (25.2%, 57/100 000 adults) and incident (44.2%, 10/100 000 adults) cause of blindness in Ireland in 2003. Increasing levels of macular degeneration have also been noted in Scotland, Denmark, Germany, and Northern Ireland, where it now accounts for between 50–70% of new registrations.8,9,10,11,12 Evans and Wormald examined this trend in England and concluded that, even allowing for an increasingly aged population, registration attributable to macular degeneration has increased in the order of 30% over recent years.13 The reason for this is as yet unclear. It is also unclear what proportion of the increase in ARMD is caused by “wet” or “dry” forms of the disease.14 Recent advances in treatment of certain types of “wet” ARMD make this an important issue and the Irish registration form has recently been modified to record the different types of macular degeneration resulting in blindness.
Glaucoma accounted for 15.9% (28/100 000 adults) of overall blind registration in 1996 and for 11.8% (27/100 000 adults) in 2003. It accounted for 13.2% (2.9/100 000 adults) of newly registered blindness in 2003. In comparison, glaucoma accounts for 14% of the newly registered blind in both Scotland and Israel.8,15 The trend towards a small reduction in the numbers being registered as a result of glaucoma has also been noted in Denmark and Germany.10,11 The possible reasons for this reduction include earlier detection and intervention and newer, possibly better, treatment.
In 1996 cataract was the third most common cause for blind registration in Ireland at 11.2% (20/100 000 adults). The prevalence of cataract as a cause of blindness has now fallen to 3.8% (9/100 000 adults). Correspondingly, there has been a 49% increase in the number of cataract operation performed in this country between 1994 and 2001.16 Cataracts are uncommon as a cause of new blindness, accounting for only 1.2% (0.3/100 000 adults) of new registrations in 2003. In both the previous Irish register study in 1996 and the recent west of Scotland study it was found that, of the few people still being registered with cataracts, most had other contributing causes for their visual loss and/or were unwilling/unfit to undergo surgery.2,8
Diabetic retinopathy as a cause of blindness is showing a worrying increase. While it only accounts for 4.7% (11/100 000 adults) of those on the register, this represents a large increase since 1996. In 1996 it was the 11th most prevalent cause of blind registration (5/100 000 adults), it is now the fifth. It is the third most common cause for new registrations at 6.3% (2/100 000 adults). This is similar to Scotland with a rate of 7.0%.8 However, this is substantially less than Germany, Northern Ireland, and Israel with rates of 17.3%, 10%, and 12.2% respectively.9,12,15 It is also a condition that now affects young people; it is the second most common cause of new registration among working adults (16–64 years) with an incident rate of 11.3% (7/100 000 working aged adults) in Ireland. Hopefully, screening for sight threatening DR should reduce the numbers of people registering over the coming years.17
The most recent study examining blind registration rates among eligible outpatients in England was conducted in the general clinics of a single specialty hospital in 2003.3 Overall, 7% of their patients were eligible for registration. This is similar to previous English studies where 6–8% of the clinic population were eligible for registration.4,5 However, in the present study only 3% of patients were eligible for registration. This difference is probably the result of the lack of partial sight registration in this country. This is also the reason that Bunce et al found 17% of patients to be eligible for registration based on visual field loss alone, whereas in Ireland only 7% of eligible patients were in this category.5 As in the present study, where 57% of eligible people were not registered, previous English studies have found that 45–52% of patients were not registered.
The patient group in Ireland was similar to that in England with more women eligible than men and the majority of potential registrees aged 65 years and over. The most common conditions causing blindness among the Irish outpatient group were ARMD, glaucoma, DR, and cataract. In contrast, in a recently published paper from an English outpatient clinic, glaucoma was found to be the most common reason for registration, followed by ARMD, retinitis pigmentosa, cataract, and diabetic eye disease.3 Again, this difference is probably accounted for by the lack of partial sight registration in this country.
Patients in the present study were divided into three groups; those with permanent conditions not requiring ongoing treatment (51%), permanent conditions requiring ongoing treatment (31%), and reversible conditions (19%). This is similar to Bunce et al who found figures of 50%, 37%, and 13%, respectively.5
The leading causes for non-registration in the study conducted by Robinson et al were “no obvious cause” at 39% of cases, the patient was undergoing treatment with good prognosis in 27% of cases, and in 14% of cases the patient was new to the service or had recent visual loss.4 In contrast, in this study, of the 43 unregistered patients, 45% were new to the service or had recent visual loss, 37% were not aware they could be registered (this group probably equates with the “no obvious cause” group in the Robinson study), and 16% were undergoing treatment with a good prognosis. It is possible, therefore, that in Ireland, patients present at a later stage in the disease process and are suitable for registration at the time they initially come to the attention of the ophthalmology services.
When we examined non-registration among Irish clinic patients we found that those over 65 years of age were significantly more likely not to be registered (p<0.01). This was not seen by either Bunce or Robinson.4,5 Irish patients with temporary causes of blindness (for example, cataract) were also, appropriately, more likely not to be registered (p<0.001). This was also seen in all previous English studies. However, Robinson and Bunce also found that patients with permanent diseases who were undergoing active treatment were more likely to be unregistered—that is, active treatment hindered registration. This was not found in the Irish patient group. Bunce et al showed that those patients eligible for registration based on visual field loss alone were three times less likely to be registered.5 This was not found in the present study, presumably owing to the stricter visual field criteria for registration in this country.
CONCLUSION
In summary, a large (37%) increase was noted in blind registration in Ireland between 1996 and 2003. ARMD accounts for 25% of the overall prevalence figures and 40% of new cases in 2003. This emphasises the importance of ongoing research into the pathogenesis and potential therapies for ARMD. Glaucoma and DR, both potentially avoidable causes of visual loss, are still causing substantial numbers of adults in this country to be registered blind. Early detection and treatment are essential to arrest the development of visual impairment in these conditions. Finally, clinicians must be constantly vigilant in recognising and certifying patients eligible for blind registration.
REFERENCES
Linked Articles
- BJO at a glance