Article Text

Abstract
Background/aims: To investigate the fluctuations of ocular blood flow parameters over 13 h in patients with primary open-angle glaucoma (POAG) and in healthy eyes, and to relate these fluctuations with variations in intraocular pressure (IOP) and mean ocular perfusion pressure (OPP).
Methods: 15 patients with POAG and 15 control subjects were included. Measurements of systemic blood pressure (SBP), fundus pulsation amplitude (FPA), choroidal blood flow (CHBF), optic nerve head blood flow (ONHBF) and IOP were performed at 08:00, 12:00, 17:00 and 21:00. OPP was calculated from IOP and SBP. The coefficient of variation (CV) was calculated for all individual parameters to assess their variability.
Results: The time response of the ocular haemodynamic variables was not different between the groups. Most of the outcome variables showed significantly larger fluctuations in patients with POAG compared with healthy controls (CV: FPA: 0.085 (SD 0.033) vs 0.054 (0.029), p = 0.012; CHBF: 0.082 (0.030) vs 0.052 (0.023), p = 0.005; ONHBF: 0.086 (0.044) vs 0.059 (0.032), p = 0.063). These changes were not associated with OPP or IOP. Changes over time correlated among the different ocular haemodynamic outcome measures in patients with POAG (r = 0.678, r = 0.557, r = 0.545; p<0.04) but not in the control subjects (r = 0.336, r = −0.227, r = −0.130; p>0.22).
Conclusion: Patients with POAG show a larger diurnal fluctuation of ocular blood flow parameters. These fluctuations appear not to be related to a higher statistical error of the applied measurement techniques in POAG patients. These data support the hypothesis that POAG is associated with vascular dysregulation.
Statistics from Altmetric.com
Primary open-angle glaucoma (POAG) is characterised by damage of nerve fibres in the optic nerve head and ganglion cell loss in the retina leading to progressive visual-field loss. The pathophysiological mechanisms underlying this disease remain unclear. For a long time elevated intraocular pressure (IOP) was considered the only important factor in the development of glaucoma and to this day remains the main therapeutic target. Nevertheless, glaucomatous damage can occur at normal IOP levels. Additional pathogenetic concepts of POAG were introduced, including abnormal ocular perfusion.1 Building on this theory, it has been assessed that POAG is associated with vascular dysregulation of optic nerve head, retina and choroid, leading to damage by ischaemia/reperfusion phenomena.2
Several studies have evaluated the role of IOP variation during the day as a risk factor for glaucoma progression,3 4 and considerable interest has been directed towards this topic in the recent years.5–7 Circadian fluctuation in ocular perfusion pressure (OPP) also appears to be an independent risk factor for POAG and normal tension glaucoma.8–10
The present study aimed to investigate whether ocular blood flow is subject to larger diurnal variation in patients with POAG compared with age-matched control subjects. We performed an unmasked comparative trial investigating fluctuations of different ocular blood flow parameters over 13 h during the day and evaluated the correlation between diurnal variations of three different ocular blood flow parameters among each other and with IOP, blood pressure and OPP.
MATERIALS AND METHODS
Subjects
The study was approved by the Ethics Committee of the Medical University of Vienna and was performed in conformity with the tenets of the Declaration of Helsinki. We included 15 patients with POAG and 15 control subjects with healthy eyes in this study after informed written consent was signed. Each subject was examined in a prestudy screening, which included physical examination and medical history, measurement of blood pressure and pulse rate, and an ophthalmic examination including visual acuity testing, measurement of IOP and slit-lamp biomicroscopy and funduscopy. Glaucoma patients were included if they featured a POAG with a medical history of IOP over 22 mm Hg, a cup/disc (C/D) ratio between 0.4 and 0.9, and mild glaucomatous defects in three recent visual field tests (Humphrey Field Analyzer, 30-2 program; Carl Zeiss Meditech, Dublin, California) with a mean deviation <10. An abnormal visual field was defined as having a glaucoma hemifield test result outside normal limits and/or a corrected pattern standard deviation with p<0.05. Patients with trabeculectomy, laser trabeculoplasty or other types of glaucoma surgery in their medical history or with signs of any other ophthalmic disease with possible vascular involvement such as diabetic retinopathy, age-related macular degeneration or retinal vein or artery occlusion were excluded. All of the patients used topical antiglaucoma therapy and had actual IOP levels below 22 mm Hg. Ten of the POAG patients also took systemic concomitant medication (table 1).
Inclusion criteria for the age-matched control subjects were overall normal medical and physical findings, and definite normal ophthalmic findings. The subjects were matched with the POAG patients with regard to their IOP levels. Nine of the 15 control subjects took systemic concomitant medication (table 1). Participants with treated systemic hypertension were not excluded from the study because of the high prevalence of this condition in elderly people. Individuals with diabetes mellitus or uncontrolled severe systemic hypertension with values above 170 mm Hg systolic blood pressure (SBP) or 100 mm Hg diastolic blood pressure (DBP) were excluded from both groups. All subjects had to have ametropia of less than 3 dioptres and were asked to refrain from alcohol and caffeine for at least 24 h before the study day.
All measurements were performed on the same eye at 08:00, 12:00, 17:00 and 21:00 in a darkened room in a seated position after a resting time of at least 10 min to stabilise haemodynamic conditions. Stabilisation was verified with repeated blood pressure measurements.
Measurement of fundus pulsation amplitude by laser interferometry
Ocular fundus pulsation amplitude (FPA) was measured by laser interferometry. This technique, which enables estimation of the pulsatile component of choroidal blood flow (CHBF), has been described by Schmetterer et al.11 Briefly, the eye is illuminated along the optical axis by a coherent laser beam with a wavelength of 783 nm. The laser light is reflected at the front surfaces of the cornea and the retina. The resulting two re-emitted light waves produce concentric interference fringes, which change their pattern synchronously with pulsation. From the detected interferogram distance changes between corneal and retinal surface during the cardiac cycle can be calculated. The maximum change in corneoretinal distance during one cardiac cycle is called FPA. In the present study FPA was measured in the fovea by asking the subjects to fixate the laser point directly.
Measurement of choroidal and optic nerve head blood flow
We used laser Doppler flowmetry (LDF) to measure CHBF and optic nerve head blood flow (ONHBF). The principles of LDF have been described in detail by Bonner and Nossal.12 In brief, vascularised tissue is illuminated by a beam of coherent laser light. Scattering on moving red blood cells (RBCs) in tissue capillaries leads to a frequency shift of the scattered light, according to the optical Doppler effect. In contrast static scatterers in tissue do not change light frequency but lead to a randomisation of light directions impinging on erythrocytes. This light diffusion in tissue leads to a broadening and shifting of the spectrum of scattered light, from which the parameters mean RBC velocity, mean blood volume and mean blood flow can be calculated in relative units. In the present study we used a fundus camera-based LDF system (LDV-5000, Oculix, Arbaz, Switzerland), which has been described in detail previously.13 14 Coherent light with a wavelength of 670 nm was directed to the fovea to assess subfoveal CHBF and to the intact neuroretinal rim of the optic nerve to assess ONHBF. In all four measurements the same spots were investigated for 2 min on average, depending on the individual fixation skills.
Measurement of IOP and systemic haemodynamics
IOP was measured with a slit-lamp mounted Goldmann applanation tonometer (Haag-Streit, Bern, Switzerland) after instillation of two drops of oxybuprocainhydrochloride combined with sodium fluorescein. SBP, DBP and mean arterial blood pressure (MAP) were measured on the upper arm by an automated oscillometric device (HP-CMS patient monitor, Hewlett Packard, Palo Alto, California). Pulse rate was automatically recorded by the same unit from a finger pulse oxymetric device. The mean OPP was calculated as 2/3×MAP–IOP.
Data analysis
The sample size calculation was based on our previously obtained data.15 16 Using a two-sided alpha error of 5% and a power of 80%, differences in variability of 25% were detectable between groups using the present sample size. For the assessment of variability of all individual parameters, the coefficients of variation (CV) were calculated using the four consecutive measurements. In addition, a mixed effects model was used, including both fixed and random effects (intercept). Finally, correlations between the changes over baseline of ocular haemodynamic outcome measures were analysed with linear regression by the use of univariate modelling. All statistical analyses were done with the Statistica software package (Release 4.5, StatSoft, Tulsa, Oklahoma). Data are presented as means (SD). A two-tailed p<0.05 was considered the level of significance.
RESULTS
The baseline characteristics of both groups are presented in table 2.
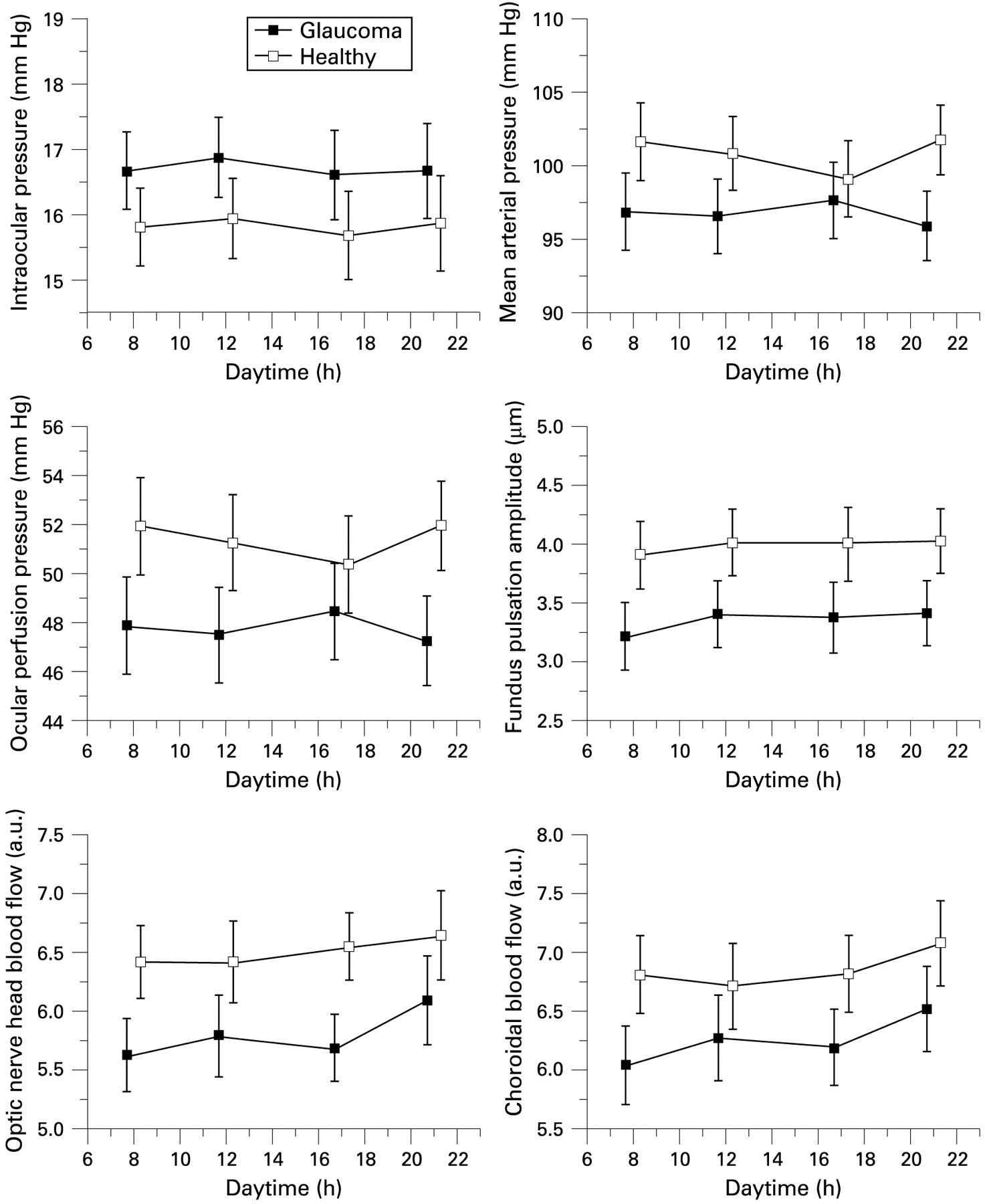
There were no significant differences between the groups except for horizontal and vertical C/D ratios which were significantly higher in the glaucoma patients (ANOVA). The averaged diurnal measurements of both groups are shown in fig 1. None of the measured parameters showed any significant changes in either of the study groups during the period of observation. Comparison of the two groups failed to show any differences in the mean values of all outcome parameters, although haemodynamic parameters were slightly lower in glaucoma patients (p value range: 0.101–0.351). The mean IOP was between 16.6 and 16.9 mm Hg in POAG patients and between 15.7 and 15.9 mm Hg in control subjects.
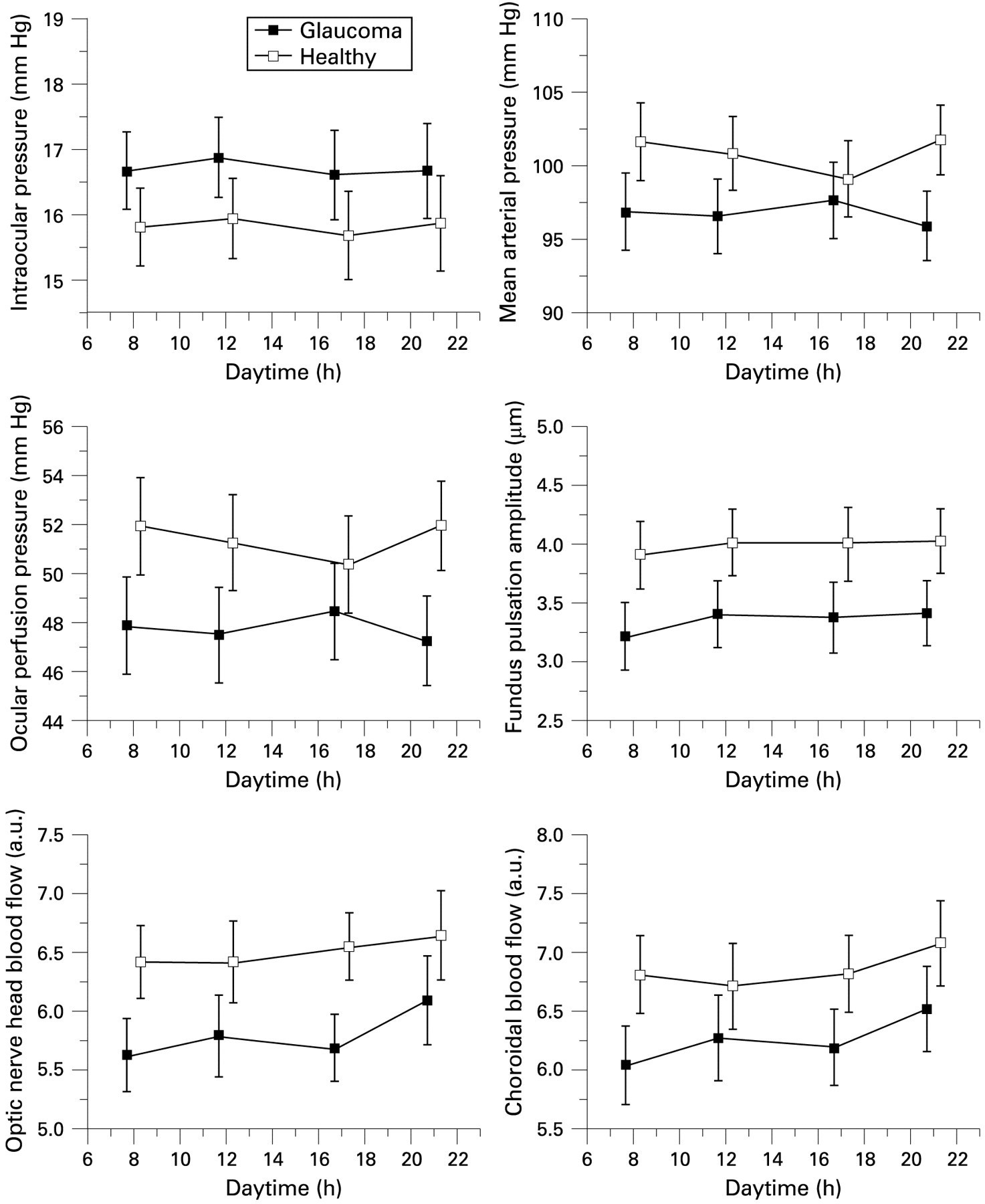
Diurnal fluctuation of measurements from 08:00, 12:00, 17:00 and 21:00. Group mean values (SD), glaucoma patients represented by black squares, healthy controls by empty squares. There is no significant change of parameters and no significant difference between groups.
After calculation of the CVs from the four measurements, we found a significantly larger diurnal variability of the ocular blood flow parameters FPA (0.085 (SD 0.033) vs 0.054 (0.029), p = 0.012 between groups) and CHBF (0.082 (0.030) vs 0.052 (0.023), p = 0.005) in patients with POAG as compared with healthy controls (fig 2). Variations of ONHBF (0.086 (0.044) vs 0.059 (0.032), p = 0.063) and IOP (0.079 (0.032) vs 0.061 (0.021), p = 0,083) tended to be higher in the glaucoma patients. The CV for OPP (0.043 (0.017) vs 0.057 (0.029), p = 0.103) was not significantly different between groups. There was a difference in MAP variation with a higher variability in healthy controls (0.025 (0.009) vs 0.040 (0.023), p = 0.023).

Coefficient of variation (CV) of intraocular pressure (IOP), mean arterial pressure (MAP), ocular perfusion pressure (OPP), fundus pulsation amplitude (FPA), optic nerve head blood flow (ONHBF) and choroidal blood flow (CHBF) calculated from four measurements over the study period. Data are presented as means (SD). *A mixed effects model was used to detect significant differences between the groups, p<0.05.
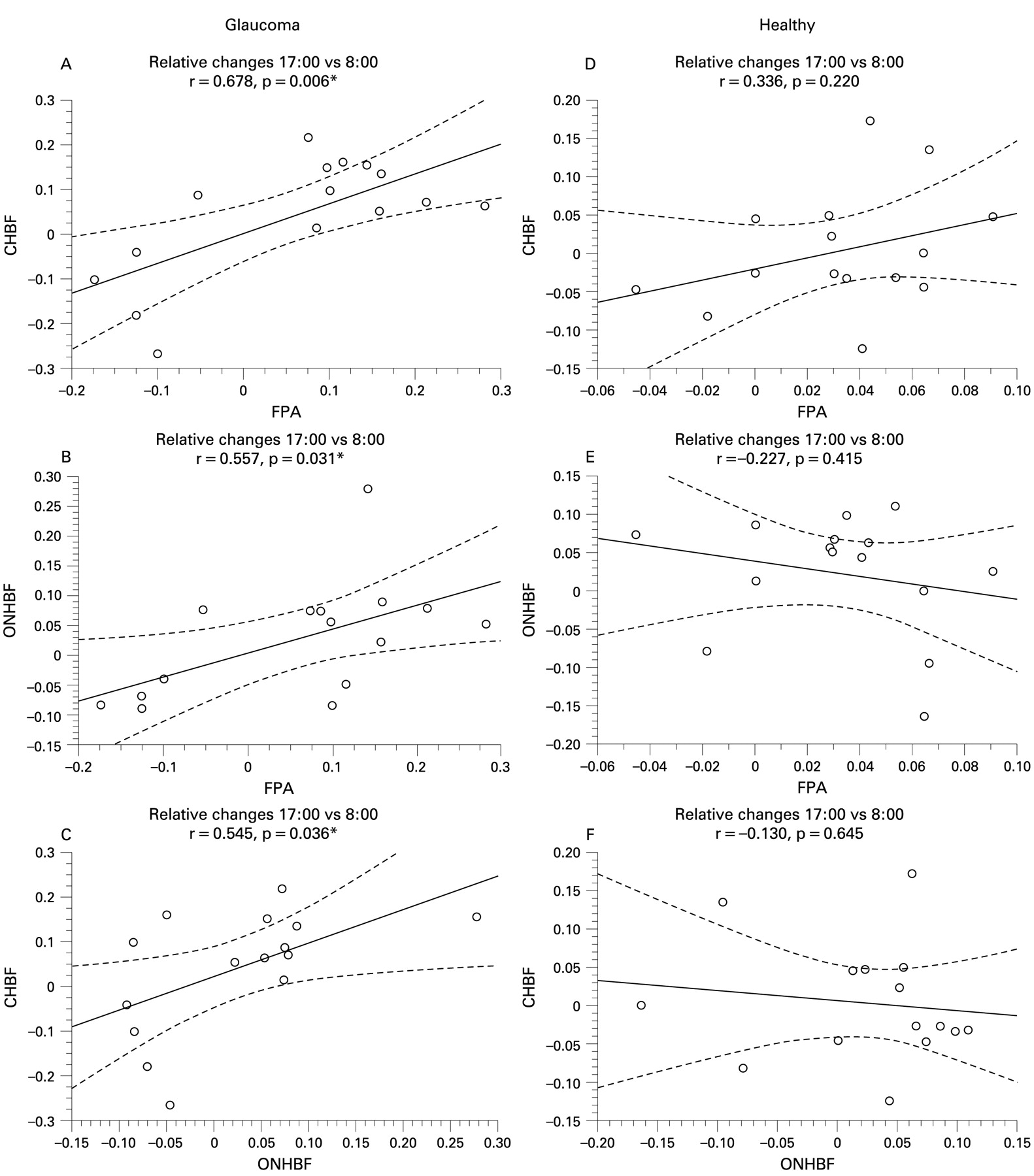
Additionally we performed a correlation analysis between the changes over time of measured and calculated parameters. Here we present data for the relative changes at 17:00 over 08:00. Data for the other times are comparable (data not shown). This analysis reveals that the changes of all measured ocular blood flow parameters in both groups were not associated with fluctuations of IOP (POAG: r<0.055, healthy: r<0.356) or OPP (POAG: r<−0.048, healthy: r<0.119). In patients with POAG we found consistent and significant correlations between the changes over time of CHBF and FPA (r = 0.678, p = 0.006), between ONHBF and FPA (r = 0.557, p = 0.031) and between CHBF and ONHBF (r = 0.545, p = 0.036) (fig 3). These correlations were not found in healthy controls.
{kind=link}
{kind=link}
{kind=link}
Linear correlations between the changes over time of choroidal blood flow (CHBF) and fundus pulsation amplitude (FPA), of optic nerve head blood flow (ONHBF) and FPA and of CHBF and ONHBF in glaucoma patients (A–C) and control subjects (D–F). Relative changes over baseline 17:00 versus 08:00. Solid lines: linear correlations, dashed lines: 95% CI. *Significant correlations.
DISCUSSION
The results of four measurements in 13 h indicate a larger variability of ocular blood flow parameters in patients with POAG compared with control subjects. In addition, the variations of three different measurement techniques for ocular blood flow correlated only in glaucoma patients but not in controls. In principle a larger fluctuation of ocular blood flow parameters in patients with glaucoma may arise from two different phenomena. On the one hand it may be a result of reduced reproducibility due to problems like target fixation. On the other hand a larger fluctuation may arise from a truly larger variability of ocular blood flow as a consequence of instable perfusion. Our correlation analysis supports the latter hypothesis. Considering that we did not observe larger fluctuations of IOP, MAP or OPP in glaucoma, we cannot determine the reason for this larger variability.
Diurnal changes of ocular blood flow in healthy and glaucomatous eyes have been assessed in few studies only. In a previous study we assessed the 12 h reproducibility of CHBF parameters in healthy subjects including FPA and LDF.15 The CVs were in the same order as in the current report. In keeping with our present findings, Claridge and Smith did not find any significant diurnal variation of pulsatile ocular blood flow (POBF) in patients with POAG, patients with ocular hypertension and normotensive control subjects during 21 h.17 Harris et al also did not observe any changes of ophthalmic arterial haemodynamics in four colour Doppler imaging measurements during the night.18 Interestingly enough, Okuno et al found a significant decrease in optic nerve head perfusion but not of choroid-retina perfusion at 21:00 versus 09:00 in patients with normal tension glaucoma using laser speckle measurements.19 Although we did not find any significant reduction in ONHBF over time, their conclusion of a larger variability of optic nerve head perfusion in glaucoma patients fits well with the results of our present study. Comparing the results of these studies the differences in study populations need, however, to be taken into account.
As mentioned before, circadian fluctuation in OPP has been identified as a risk factor for glaucoma.8–10 We could not find any significant difference in absolute OPP or OPP fluctuation between glaucoma patients and healthy controls. However, the present study indicates that even with comparable IOP and OPP there is still a difference in the stability of ocular perfusion between healthy and glaucomatous eyes.
Several studies have presented data of reduced blood flow in the optic nerve head of glaucoma patients using LDF20 or scanning LDF.21 22 This could not be observed in the present study, although all blood flow parameters tended to be lower in glaucoma patients. A larger sample size may have been required to find such a difference, but our sample size calculation was not based on this aim. Also, LDF has some limitations in assessing ONHBF which have been discussed previously.23 Another limitation of this study is the large number of participants who used systemic medication. However, the pharmacological agents taken by the participants in this trial stem from many different classes, and the few vasoactive substances may have little implication on the results of this study.24 The use of topical antiglaucomatous therapy represents another factor that could have an influence on the findings of our study. Several studies have investigated the influence of different topical glaucoma therapy on ocular blood flow, but the effects are generally considered small.24 Only two treatment regimen included dorzolamide, which may indeed affect ocular perfusion.25 However, we cannot completely rule out possible effects of medication used by the participants, particularly on diurnal blood flow variability. On the other hand, the fact that the study groups were well matched for IOP and OPP by the use of medication allows for a comparison of the variation of blood flow parameters independent from elevated IOP values in POAG.
We did not measure blood flow parameters during the night, because such measurements cannot be done without awakening the patient. During the night hours, variability in ocular blood flow may well be higher than during the day, and the differences between glaucoma patients and healthy controls may exceed the relatively subtle differences observed in the present study. In addition, we have only chosen four fixed time points in the present study, because the measurements were exhausting for older participants.
In conclusion, the results from this study indicate that patients with POAG have a larger diurnal fluctuation of ocular blood flow. Since we observed correlations between these fluctuations as assessed with different methods, this does not appear to be related to higher statistical errors in patients. Our results are therefore compatible with the idea that glaucoma has characteristics of a low-grade ischaemic disease with dysfunctional regulation of ocular microcirculation. Both circadian IOP fluctuation and larger ocular blood flow fluctuation may well contribute to the disease process, although these hypotheses need to be confirmed in large-scale clinical outcome trials.
REFERENCES
Footnotes
Competing interests: None.
Ethics approval: Ethics approval was provided by the Ethics Committee of the Medical University of Vienna.
Linked Articles
- At a glance