Article Text

Abstract
Aim: The aim of the study was to describe the prevalence and visual outcomes of cataract surgery in an urban Asian population.
Methods: This was a population-based study of 3280 Singapore Malays aged 40–80 years (response rate 78.7%). Participants had a standardised interview and comprehensive ocular examination. Poor post-operative visual outcome was defined as visual acuity ⩽20/60 in operated eyes of unilateral cataract extractions or in the better-seeing eye of bilateral cataract extractions. Factors associated with poor visual outcome were assessed.
Results: Of 3280 participants, 284 (men 52.3%) had unilateral cataract extractions (age-standardised prevalence 4.7%, 95% CI 4.2% to 5.4%) and 154 persons (54%) had bilateral extractions. Older age, male sex and the presence of diabetes were significant factors associated with having had cataract surgery. Poor visual outcomes were present in 10.8% of the operated eyes using best-corrected visual acuity. Diabetic retinopathy (25.5%), glaucoma (17%), age-related macular degeneration (14.9%) and posterior capsular opacification (14.9%) were the main causes of poor visual outcome after surgery. Under-corrected refractive error accounted for 60% of patients with post-operative presenting visual acuity of ⩽20/60.
Conclusions: Five per cent of the sample of the Malay population aged 40–80 years in Singapore had cataract surgery. One in ten had post-operative best-corrected visual acuity of 20/60 or worse, largely related to concomitant retinal diseases.
Statistics from Altmetric.com
Cataract surgery is the most common and cost-effective surgical procedure performed worldwide, accounting for more than one-half of ophthalmic operations in most countries.1 2 Although data on the epidemiology of cataract surgery have been reported from developed countries in the western world3–6 and developing countries in the Indian sub-continent,7–9 less is known about the frequency, risk factors and visual outcomes of cataract surgery in other developed and developing countries in Asia. Such data are critical for public health planning and resource allocation.
Singapore is an urban city-state in south-east Asia, with a multi-ethnic Chinese, Indian and Malay resident population. We have previously reported that the annual rate of cataract surgery in Singapore was 356.4 per 100 000 persons/year, with Malays having the lowest rate (237.2 per 100 000/year) in comparison with the other two groups.10 The reasons for these ethnic/racial differences are unclear. The objective of the present study was to describe the prevalence, risk factor associations and visual outcomes of cataract surgery in the Malay population in Singapore.
METHODS
Study population
The Singapore Malay Eye Study (SiMES) was a population-based, cross-sectional epidemiological study of 3280 Malay adults, aged 40–80 years, living in Singapore. Details of the SiMES study design, sampling plan, methodology and baseline characteristics have been reported elsewhere.11 12 In brief, we performed an age-stratified random sampling of all Malay adults aged 40–80 years residing in 15 residential districts in the south-western part of Singapore. Of the 4168 eligible individuals, 3280 participated in the study (response rate 78.7%).
All examinations were conducted from August 2004 to June 2006 at the Singapore Eye Research Institute, a clinical research facility located centrally in Singapore. The study adhered to the Declaration of Helsinki.
Study procedures
At the study clinic, all participants underwent extensive and standardised examination procedures, which included visual acuity (VA) testing, slit-lamp biomicroscopy, stereoscopic fundus examination and ocular imaging (lens and retina). A detailed interviewer-administered questionnaire was used to collect relevant socio-demographic information, including marital status, education, occupation, current housing status, history of ocular and medical conditions, use of spectacles and lifestyle factors. Non-fasting serum glucose and glycosylated haemoglobin (HbA1c), were measured from venous blood samples collected from participants.
For each eye, the presenting VA (PVA), where the participant’s VA was ascertained while wearing their ‘walk-in’ optical correction (spectacles or contact lenses), if any, and best-corrected visual acuity (BCVA), where refraction was corrected by trained and certified study optometrists, were obtained. VA was measured using a logarithm of the minimum angle of resolution (LogMAR) number chart (Lighthouse International, New York, USA) at a distance of 4 m.
Clinical assessment of lens status and the presence of aphakia or pseudophakia were determined with a slit-lamp. Any cataract surgery was defined as the absence, in at least one eye, of the crystalline lens. The presence or absence, and the clarity, of the posterior lens capsule, was determined in aphakic and pseudophakic eyes.
Definition and causes of poor visual outcome
Poor visual outcome in eyes with cataract surgery was defined by a PVA of 20/60 or worse, or BCVA of 20/60 or worse, in the operated eye in unilateral cataract extraction or the better-seeing eye in bilateral extractions. Primary causes of poor visual outcome were determined by the study ophthalmologists, based on standard clinical criteria, according to definitions specified in the study protocol and if necessary, from ocular imaging data (lens and retinal).12 Under-corrected refractive error in the operated eye was defined as an improvement of at least 0.2 LogMAR (two lines equivalent) in the BCVA compared with the PVA. Glaucoma was diagnosed using the International Society of Geographic and Epidemiological Ophthalmology (ISGEO) classification.13 Age-related macular degeneration (AMD) was graded from retinal photographs using the Wisconsin Age-related Maculopathy grading system.14 Diabetic retinopathy was graded from retinal photographs according to a modification of the Arlie House classification system as used in the Early Treatment Diabetic Retinopathy Study (ETDRS).15
Statistical analysis
The rates of cataract surgery in our population sample were estimated and age-standardised to the Malay population from the 2000 Singapore Census, using a direct standardisation method. The prevalence and causes of poor visual outcome, as defined by PVA and BCVA, were calculated for all cataract-operated eyes. Anderson’s behavioural model was used to evaluate factors associated with cataract surgery.16 This model suggests that people’s use of health services is a function of their predisposition to use services, of enabling factors that facilitate or impede use, and of need factors for services, as perceived by people or as evaluated by health professionals. Predisposing variables include age and sex. The enabling variables include education, income, smoking and housing status. The need variables include occupation, diabetes, hypertension and living alone. Logistic regression analysis was performed to assess the predictors of poor visual outcomes following cataract surgery. Statistical analysis was performed using the statistical software SPSS v13 (SPSS Inc., Chicago, IL, USA). A p value <0.05 indicated statistical significance.
RESULTS
Of the 3280 participants, we excluded nine subjects who did not have visual acuity data and 13 subjects who declined slit-lamp examination or had missing lens data, leaving 3258 subjects for this analysis.
There were 284 subjects (8.7%) with cataract extraction in at least one eye (10 with aphakia and 274 with pseudophakia) and 154 subjects (4.7%) with bilateral extractions (four with aphakia and 150 with pseudophakia). Table 1 shows the age- and sex-adjusted prevalence of cataract surgery. Rates of any cataract surgery and bilateral cataract surgeries increased with age, with prevalence increasing from 0.2% in those aged 40–49 years of age to 23.3% in those aged ⩾70 years (test for trend p<0.001). The crude prevalence rates were slightly higher for men (9.4%) than for women (8.1%), but this difference was not significant.
Table 2 presents the factors associated with cataract surgery. Multivariable-adjusted analysis showed that older age (adjusted odd ratio (OR) per 10 years increase in age 2.7, 95% CI 2.2 to 3.3), male sex (adjusted OR 1.6, 95% CI 1.0 to 2.5) and the presence of diabetes (adjusted OR 2.4, 95% CI 1.8 to 3.1) were significantly associated with a high likelihood of having undergone cataract surgery, after adjusting for education, occupation, smoking status, diabetes and hypertension.
Poor visual outcome following cataract surgery was found in 26.8% (n = 117 eyes) of operated eyes as defined by PVA, and in 10.8% (n = 47 eyes) as defined by BCVA. Of the 63 participants with poor visual outcomes following cataract surgery, 23 (16 women) wore spectacles (either single vision lenses, bifocals or progressive lenses) at the time of examination. Table 3 summarises the main causes of poor visual outcomes following cataract surgery as defined by PVA and BCVA, respectively. The primary causes of poor visual outcomes following cataract surgery defined by BCVA were co-existing ocular conditions, including diabetic retinopathy (25.5%), glaucoma (17.0%), posterior capsular opacification (14.9%) and AMD (14.9 %). Under-corrected refractive error accounted for 59.5% of patients with poor outcomes as defined by PVA. Comparison of the leading causes of poor visual outcome between aphakic (nine eyes) and pseudophakic eyes (107 eyes), based on best-corrected visual acuity, showed that the leading causes in aphakic eyes were trauma-related (corneal scar and retinal detachment) (28.6%), glaucoma (14.3%) and AMD (14.3%) while in pseudophakic eyes, they were diabetic retinopathy (30%), posterior capsular opacification (17.5%) and glaucoma (17.5%).
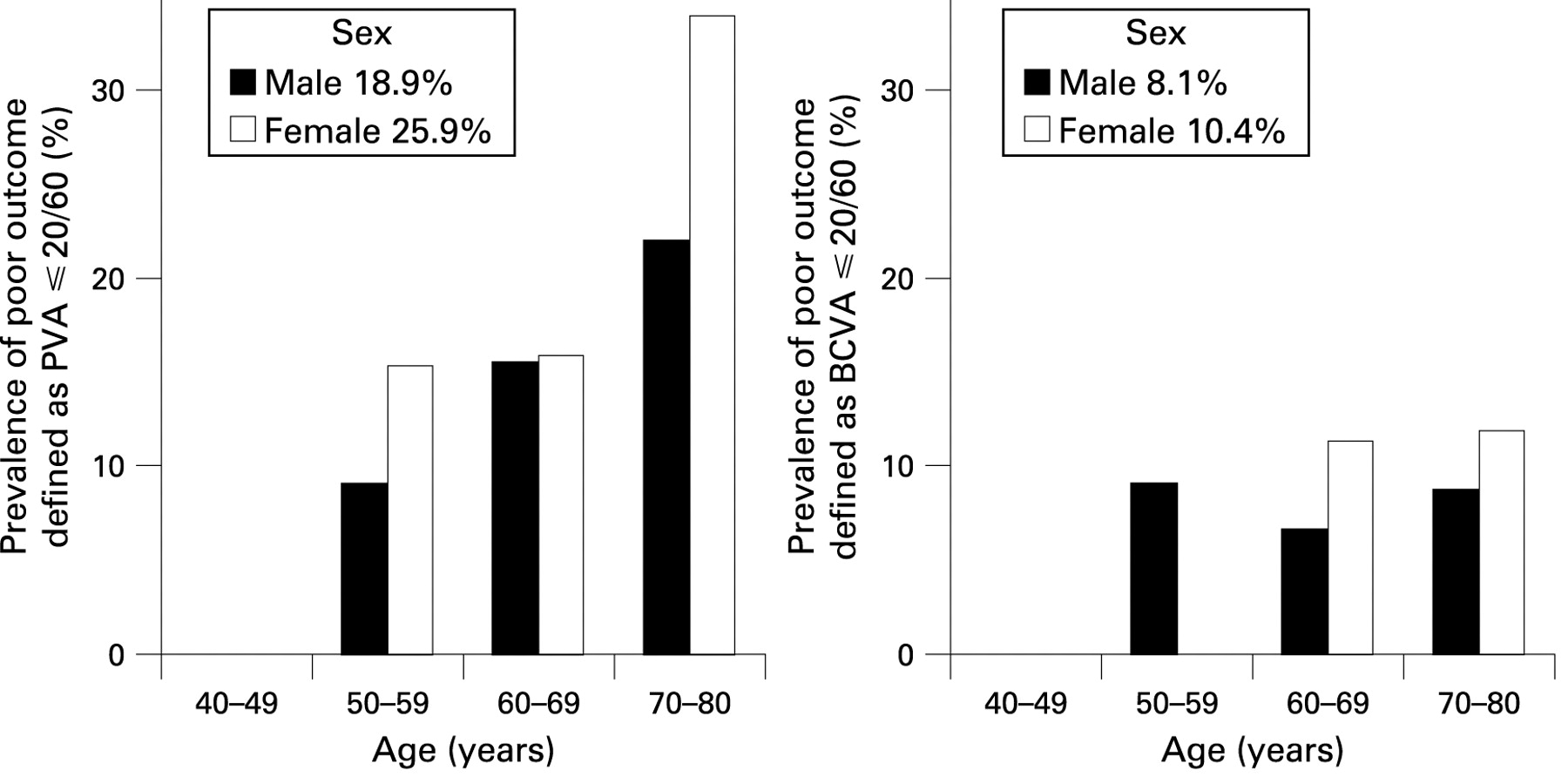
Fig 1 illustrates the prevalence of poor outcomes by age and sex, and by PVA and BCVA. Women were more likely to have poor outcomes than men (25.9 % of women vs 18.9% of men as defined by PVA, and 10.4% of women vs 8.1% of men as defined by BCVA; p = 0.05). Older women (>70 years old) were more likely to have under-corrected refractive errors after surgery. Apart from age (adjusted OR for per year increase in age 1.07, 95% CI 1.02 to 1.12, p = 0.007), we did not find any socioeconomic characteristics or systemic conditions associated with poor visual outcomes following cataract surgery.
{kind=link}
DISCUSSION
This study provides epidemiological data on the prevalence and outcomes of cataract surgery in an urban Malay population aged 40–80 years residing in Singapore. First, we have shown that the standardised prevalence of any cataract extraction (weighted to the Singapore Malay adult population census in 2000) was 4.7%. Table 4 summarises the prevalence, determinants and outcomes of cataract surgery reported by different population-based studies elsewhere. The prevalence rates seen in SiMES are comparable with the rates reported in the Tanjong Pagar Study (5.1%) in a Chinese sample of similar age in Singapore,17 in the Beaver Dam Study5 (7.0%) and in the Blue Mountains Eye Study6 (6.0%). Second, we found that increasing age, male sex and the presence of diabetes were significantly associated with having cataract surgery. Third, we showed that 10.8% of Malays who had undergone cataract surgery had poor visual outcome based on BCVA, due to co-existing ocular conditions such as diabetic retinopathy and glaucoma.
In this sample of Singapore Malays, the prevalence rates of unilateral and bilateral cataract surgeries tripled for each decade of age. After adjusting for age, education, occupation, hypertension and smoking, men were more likely to have had cataract surgery than women. Our findings are in contrast to those reported by previous studies in Singapore,10 which found that women had higher rates of surgery than men, but similar to reports from India8 18 and Nepal.9 Malay women may have had less access to eye health services than men, or may have left their impaired vision to a relatively severe stage before seeking cataract surgery. A better understanding of factors influencing the decision to take up cataract surgery services in men and women would be useful to address this gap between the sexes.
Diabetes was an independent factor strongly associated with cataract surgery. This finding is consistent with the Tanjong Pagar Study, in which diabetes was the only independent risk factor associated with cataract surgery.17 In the Beaver Dam Study, subjects diagnosed with diabetes were more likely to have cataract surgery within 5 years compared with those with normal glucose levels.5 In a case–control study in France, diabetes, smoking and lower socioeconomic status were found to be associated with cataract surgery.21 Diabetes is a known risk factor for cortical and posterior subcapsular cataract.17 22 With an increasing prevalence of diabetes in Asian countries, an increasing demand for cataract surgery is likely.
We did not find any association between socioeconomic indicators and cataract surgery, suggesting that demand for cataract surgery is largely driven by need factors, determined by the patient’s decision. From a public health perspective, healthcare service, including cataract surgery, is easily accessible and affordable in Singapore, with service provision throughout the country to all sectors of the population. Cataract surgery can be paid for by Medisave, a government-administered medical savings programme available to all Singapore citizens, and to permanent residents and their families, covering up to 80% of medical procedures costs in both the public and private sectors.
We found that one in four surgical eyes had poor visual outcome among older Malays, and women tended to have poorer visual outcomes after surgery than men. More than one-half (60%) of these eyes with poor presenting visual outcome did not have adequate correction for refractive error. The magnitude of under-corrected refractive error among persons following cataract surgery in our sample was similar to that found in the Los Angeles Latino Eye Study (LALES),3 where it was estimated that 20% of participants with any visual impairment following cataract surgery could achieve good visual acuity with refractive correction. In our study sample, 15.1% (64 out of 423 eyes) of all pseudophakic eyes had some residual refractive error, i.e. a PVA of worse than 20/60. Similar findings were also observed in other Asian countries.8 9 18 With advances in microsurgery and intraocular lens technology, it is increasingly important for surgeons to aim for procedures that minimise residual refractive error and thereby reduce the need for post-operative refractive correction.
The main causes of poor visual outcome after refractive correction were diabetic retinopathy (25.5%), glaucoma (17%), posterior capsular opacification (14.9%) and AMD (14.9%). Previous studies in Singapore reported lower prevalence of diabetes,23 diabetic retinopathy24 and acute symptomatic angle closure25 26 in Malays compared with other ethnic groups. Thus, the fact that diabetic retinopathy and glaucoma accounted for 42% of visual impairment after cataract surgery in our study sample is of great concern. This is in contrast to studies from the west, where AMD appears to be the leading cause of poor visual outcome following cataract surgery.3 4 The public health impact of the rising prevalence of diabetes and diabetic retinopathy on cataract surgery service demand and outcomes, as reflected by our data, will be relevant for planning healthcare strategies in Singapore and other developing Asian economies.
According to the 2000 Singapore census, our study sample is fairly representative of the Singapore population in terms of age distribution, housing type and socioeconomic status. Causes of poor visual outcome were determined by a single ophthalmologist during clinical eye examinations, and this may have been a relatively subjective judgment. We do not have information on the time since cataract surgery or whether the participants had surgical complications. Hence, we cannot comment on the influence of surgical complications on the post-operative visual outcomes.
The strengths of our study include a large sample size, high response rate (79%) and the use of standardised protocols based on those of the Tanjong Pagar Study17 and the Blue Mountains Eye Study.6 This is the first population-based study on the prevalence and outcomes of cataract surgery in the third largest Asian ethnic group, the Malays. There are nearly 300 million Malays living predominantly in cities and urban areas of Malaysia, Singapore, Indonesia and other south-east Asian countries. With an estimated worldwide doubling of the older sector of the population by 2020, the prevalence of cataract, visual morbidity and the demand for cataract surgery will be formidable. Using VA as an indicator, it is estimated that the number of cataract surgeries will increase fivefold if the VA threshold for surgery is reduced from 20/200 to less than 20/40.27 The advances in keratorefractive surgeries in recent years have increased public awareness and the pursuit of uncorrected super-vision of better than 6/6. This may translate into a reduced visual acuity threshold and an even greater demand for cataract surgery. Public health strategies are clearly needed to tackle the unprecedented demand for cataract surgery. Our population-based prevalence data provides valuable information to health policy planners on the need, uptake and outcomes of these services.
In summary, in this population-based sample of Singapore Malays, we found that one in 20 had cataract surgery (4.7%). Under-corrected refractive error and diabetic retinopathy were the two major causes of poor visual outcomes, emphasising the need to monitor refractive status, to have regular follow-ups and to manage patients with diabetes after cataract surgery.
REFERENCES
Footnotes
Funding: This study was supported by the National Medical Research Council Grants No 0796/2003, 0863/2004 and CSI/0002/2005, and Biomedical Research Council Grant No 501/1/25-5, with additional support from the Singapore Tissue Network and the Ministry of Health, Singapore.
Competing interests: None declared.
Ethics approval: Ethics approval was obtained from the Singapore Eye Research Institute Institutional Review Board.
Patient consent: Obtained.
Linked Articles
- At a glance