Article Text

Abstract
Aim The aim of the study was to investigate the correlation between the clinical manifestation and the cytomegalovirus (CMV) viral load in the aqueous humour of patients with CMV anterior uveitis.
Methods Seven patients with CMV-associated iridocyclitis and four patients with CMV-associated corneal endotheliitis were enrolled. Presence of CMV, but not other human herpes viruses, was confirmed by multiplex polymerase chain reaction (PCR). Viral load was measured using real-time PCR. Clinical manifestations were examined using a slit-lamp microscope and ophthalmoscope, applanation tonometer and specular microscope.
Results All 11 patients had unilateral recurrent anterior uveitis with high intraocular pressure and mutton fat keratic precipitates with pigmentation. Stromal oedema of the cornea was found in CMV-associated endotheliitis, but not in CMV-associated iridocyclitis patients. A significant corneal endothelium cell loss was recorded in all 11 patients with CMV-associated endotheliitis and iridocyclitis patients. High viral loads of CMV were detected in the aqueous humour of all 11 patients. A significant association was found between the corneal endothelial cell loss intensity and CMV viral load in the aqueous humour.
Conclusion There is a significant correlation between the CMV viral load and corneal endothelial cell loss in both CMV-associated iridocyclitis and corneal endotheliitis.
- Aqueous humour
- cornea
- corneal endotheliitis
- cytomegalovirus
- genetics
- infection
- inflammation iridocyclitis
- polymerase chain reaction
Statistics from Altmetric.com
- Aqueous humour
- cornea
- corneal endotheliitis
- cytomegalovirus
- genetics
- infection
- inflammation iridocyclitis
- polymerase chain reaction
Introduction
Cytomegalovirus (CMV) is a member of the human herpes virus family and is found in latent infections in the majority of the adult population. In immunocompromised hosts, the virus causes necrotising retinitis,1 but has been thought not to cause any diseases in immunocompetent hosts. However, a previous study showed local production of anti-CMV antibodies in the aqueous humour of an immunocompetent patient with iridocyclitis with elevated intraocular pressure (IOP).2 In addition, recent studies using qualitative PCR have demonstrated that genomic CMV DNA is present in the aqueous humour of immunocompetent patients with unilateral iridocyclitis3–6 as follows. Markomichelakis et al3 reported two cases of iridocyclitis with sectoral iris atrophy in which CMV was detected by PCR, and de Schryver et al4 also reported five similar cases. In the recent report by Chee et al,5 they studied if there was a relationship between the CMV viral load in the aqueous and clinical manifestation of the diseases such as either acute or chronic iridocyclitis, eg Posner–Schlossman syndrome and Fuchs heterochromic iridocyclitis. CMV genomic DNA was also detected in the aqueous humour of immunocompetent patients with another inflammatory condition of the eye, ie corneal endotheliitis, in three previous reports.7–9 Corneal endotheliitis is an inflammatory condition at the corneal endothelium in which keratic precipitates (KPs) develop together with severe stromal oedema in the cornea, whereas iridocyclitis has cells and flare in the anterior chamber with or without KPs but no stromal oedema in the cornea.
The real-time PCR made it possible to measure the viral load quantitatively. Thus, the use of this assay makes it possible to determine the clinical significance of the viral infection in the pathogenesis of human diseases. Our previous report showed a high CMV genomic DNA load in the aqueous humour in an immunocompetent patient with unilateral iridocyclitis with high IOP.6 However, the correlation between the viral load in the aqueous humour and the clinical manifestation of the disease (iridocyclitis versus corneal endotheliitis) was not investigated. Therefore, we examined if there was any correlation between the CMV viral load in the aqueous humour and the clinical manifestation of anterior inflammatory diseases associated with CMV. We showed a significant correlation between the CMV viral load in the aqueous humour and the endothelial cell damage of the cornea in patients with iridocyclitis and corneal endotheliitis associated with CMV.
Materials and methods
Subjects
Between 2006 and 2008, 11 patients with CMV-associated inflammation in the anterior segment of the eye, ie seven patients with CMV-associated iridocyclitis and four patients with CMV-associated corneal endotheliitis, were enrolled. These patients were from Tokyo Medical and Dental University Hospital (Tokyo, Japan), Miyata Eye Hospital (Miyakonojo, Miyazaki, Japan) and Kyoto Prefectural University Hospital (Kyoto, Japan). Diagnosis was made based on clinical manifestations and the qualitative detection of the CMV genomic DNA in the aqueous humour by the multiplex PCR. The viral load in the aqueous humour was further measured quantitatively by the real-time PCR.
An aliquot of 0.1 ml of the aqueous humour was aspirated with a 30G needle after disinfection and processed for PCR. Anti-viral therapy was not given before the PCR assay, but topical corticosteroids were given by local ophthalmologists to treat intense anterior uveitis. The interval between the disease onset and the aqueous humour sampling varied among the patients.
Polymerase chain reaction
The aqueous humour samples were centrifuged at 1000 g for 5 min and used for multiplex PCR and real-time PCR.10 11 Multiplex PCR was designed to qualitatively measure the genomic DNA of eight human herpes viruses: herpes simplex virus type 1 (HSV-1) and type 2 (HSV-2), varicella zoster virus (VZV), Epstein–Barr virus (EBV), CMV, and human herpes virus type 6 (HHV-6), type 7 (HHV-7) and type 8 (HHV-8). DNA was extracted from the aqueous humour samples using a DNA minikit (Qiagen, Valencia, California, USA). Multiplex PCR was performed using LightCycler (Roche, Basle, Switzerland). The primers of the glycoprotein gene sequences for CMV were TACCCCTATCGCGTG TGTTC (forward) and ATAGGAGGCGCCACGTATTC (reverse). The probes used included 3′-fluorescein isothiocyanate: TCGTCGTAGCTACGCTTACAT and LcRed705-5′: ACACCACTTATCTGCTGGGCAGC. Specific primers for the virus were used in conjunction with Accuprim Taq (Invitrogen, Carlsbad, California, USA). PCR amplification conditions used in the current study have been reported previously.12
Real-time PCR was only performed for the HHV, with multiplex PCR used to detect the genomic DNA. Amplitaq Gold, with a Real-Time PCR 7300 system (ABI, Foster City, California, USA), was used to perform the procedure. The forward and reverse primers of immediate early (IE)-1 were CATGAAGGTCTTTGCCCAGTAC and GGCCAAAGTGTAGGCTACAATAG, respectively. FAM-TGGCCCGTAGGTCATCCACACTAGG-TAMRA was used as the probe. The PCR amplification conditions used in the current study were previously reported by Sugita et al.11 When more than 50 copies per tube (5×103/ml) were observed, the value of the sample's viral copy number was considered to be significant.
Clinical evaluation
Clinical manifestations of the eye were determined by a slit-lamp microscopic and ophthalmoscopic examination. Each patient underwent best corrected visual acuity (BCVA) measurement using a Japanese standard decimal visual acuity chart (Landolt ring chart) after treatment. Anterior chamber flare was measured by a laser flare photometer (FC-1000; Kowa Electronics, Nagoya, Japan). A photograph of the central cornea using a specular microscope (NONCON ROBO FA-3509; Konan Medical, Nishinomiya, Japan) was used for evaluation of the corneal endothelial cells. In cases of corneal endotheliitis, intense corneal oedema disturbed the measurements of the corneal endothelium, and we measured corneal endothelial cell counts after the inflammation was reduced by the treatment.
Evaluation of corneal endothelial cell loss
The relationship between the CMV viral load in the aqueous humour and the intensity of the corneal endothelial cell loss was assessed. The corneal endothelial cell loss was determined according to the following formula:
Statistical analysis
Statistical analysis was performed using the Mann–Whitney U test. Statistical significance was set at p<0.05. Linear regression analysis was performed using the Spearman's correlation coefficient by rank test.
Results
Clinical manifestations
Nine men and two women ranging in age from 23 to 71 years (mean age 60.6 years) were enrolled in the study. No abnormalities were found in the systemic investigations and laboratory tests. Serology examinations for human immunodeficiency virus were all negative. None of the patients had any history of eye surgery prior to the onset of uveitis. Clinical findings of the CMV-associated iridocyclitis patients (n=7) and corneal endotheliitis patients (n=4) are shown in table 1. A unilateral mild anterior uveitis with high IOP was noted in all 11 patients. There were no significant differences between the iridocyclitis and corneal endotheliitis groups in the cells and flare values in the anterior chamber, nor were there any differences noted for the elevated levels of IOP, KPs, gonioscopic findings and iris atrophy. Stromal oedema of the cornea was seen in all corneal endotheliitis but not in iridocyclitis patients. While the stromal oedema was diffuse in three out of the four patients, it was localised at upper cornea in one of the corneal endotheliitis patients. Representative cases for iridocyclitis and corneal endotheliitis are shown in figures 1 and 2, respectively. As for the IOP elevation, all 11 eyes required anti-glaucoma medications, with two eyes (cases 1 and 2) requiring trabeculectomy. With regard to the iris atrophy, no sectorial iris atrophy was seen in all 11 eyes, although four eyes (two each in the iridocyclitis and the corneal endotheliitis groups, respectively) presented diffuse iris atrophy.
Clinical findings in patients with CMV anterior uveitis

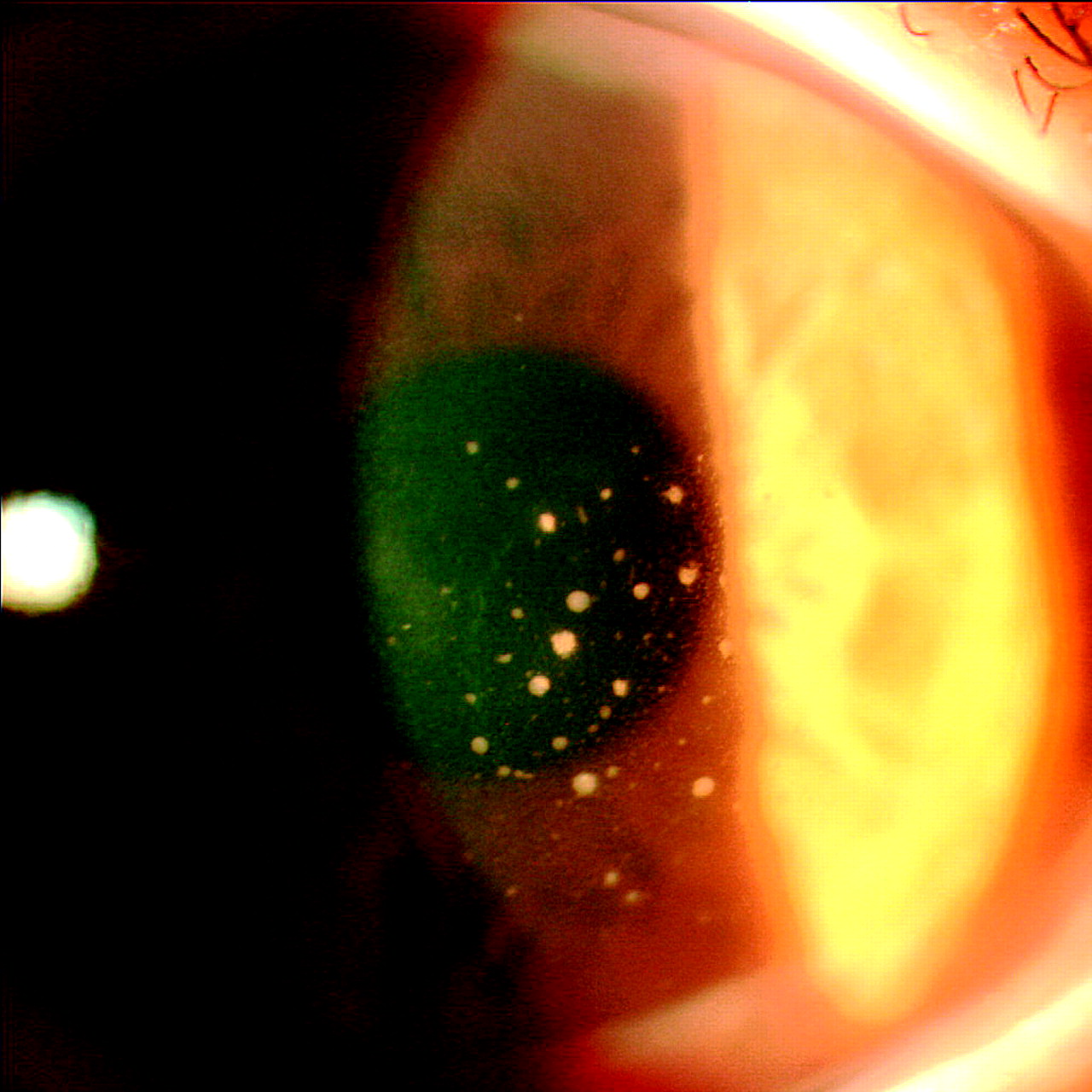
Case 4: Slit-lamp microscopy photo with cytomegalovirus-associated iridocyclitis. Mutton fat keratic precipitates with some pigmentation were scattered within the central area of the cornea. There was mild inflammation found within the anterior chamber.

Case 8: Slit-lamp microscopy photo with cytomegalovirus-associated corneal endotheliitis. Diffuse corneal stromal oedema with folds in Descemet's membrane was observed.
Systemic valganciclovir therapy (1800 mg/day for longer than 3 weeks) in conjunction with topical corticosteroids and anti-glaucoma agents effectively controlled the inflammation in the anterior segment of the eye as well as the high IOP.
Corneal endothelial cell loss
Specular microscopic examination revealed significant corneal endothelial cell loss (≥35%) in all 11 patients (table 2). Severe corneal endothelial cell loss larger than 70% was recorded in more than one-half of the endotheliitis group eyes. In contrast, this severe cell loss was observed in one of the seven patients with iridocyclitis.
Virological analysis and corneal endothelial cell findings in patients with CMV anterior uveitis
There were several patients (cases 1, 8, 10 and 11; see table 2) with corneal endothelial cell counts <700 cells/mm2. Among the patients, three cases had a low visual acuity between 0.3 and 0.6. However, one patient had a good visual acuity of 1.5.
PCR analysis of the aqueous humour samples
Multiplex PCR analyses confirmed the presence of CMV genomic DNA, but none of the other human herpes viruses (HSV-1, HSV-2, VZV, EBV, HHV-6, HHV-7 or HHV-8) in all 11 of the patients (table 2).
Quantitative real-time PCR detected significant viral loads of CMV genomic DNA in the aqueous humour of all 11 patients, with values ranging from 5.4×103 to 5.9×106 copies/ml (table 2). The mean values for the CMV viral load in the iridocyclitis and corneal endotheliitis groups were 9.4×105 and 1.2×106 copies/ml, respectively. The differences in CMV viral load between the two groups were not significant (p=0.571).
The corneal endothelial cell damage intensity was correlated to the CMV viral load in the aqueous humour. Results of the linear regression analysis demonstrated a positive correlation between the CMV viral load and the corneal endothelial cell loss (Spearman's correlation coefficient by rank test, r=0.664; p=0.036; figure 3).

{kind=link}
{kind=link}
{kind=link}
Correlation between cytomegalovirus (CMV) viral load and corneal endothelial cell damage. The CMV viral load was plotted on a logarithmic graph versus the corneal endothelial cell loss (%). The scatter plot shows significant correlation between the CMV viral load and the corneal endothelial cell loss (Spearman's correlation coefficient by rank test, r=0.664; p=0.036).
However, there was no correlation between the interval from the disease onset to the aqueous sampling and the viral load in the aqueous humour (Spearman's correlation coefficient by rank test, r=0.445; p=0.159). Furthermore, the interval from the disease onset to the sampling was not correlated with the corneal endothelial cell damage intensity (Spearman's correlation coefficient by rank test, r=0.373; p=0.239). In addition, there was also no correlation between the viral load and many other ocular findings, such as cells and flare in the anterior chamber, types of KPs, gonioscopic findings, IOP and post-treatment BCVA.
Discussion
The present study analysed ocular manifestations and CMV viral loads in the aqueous humour of patients with CMV-associated iridocyclitis and corneal endotheliitis. Our major findings included: (1) presence of significant corneal endothelial cell loss in both corneal endotheliitis and iridocyclitis tested eyes; and (2) a significant correlation between corneal endothelial cell loss and CMV viral load in the aqueous humour.
Even though it has been demonstrated that viral infections play a significant role in many inflammatory diseases, a qualitative PCR method that is capable of determining the pathological role of these viral infections has yet to be elucidated. If the presence of viral DNA in an affected disease site could be proven, the quantitative determination and correlation with the clinical manifestations of the viral infection could lead to a much deeper understanding of the role of the virus as a pathogenic disease candidate. For example, we have previously reported on two intraocular inflammatory disorders: one involving uveitis associated with human T-cell leukaemia virus type 1 (HTLV-1)13 14 and the other involving anterior uveitis associated with VZV.14 In HTLV-1 uveitis, a significantly higher HTLV-1 viral load was detected in the peripheral blood mononuclear cells of the patients compared with asymptomatic HTLV-1 carriers.13 This viral load was significantly correlated with the vitreous inflammation of the disease.14 In our report on anterior uveitis associated with VZV, we demonstrated there was a high VZV viral load within the patient's aqueous humour. Furthermore, there was a significant correlation between the viral load and the intensity of the iris atrophy in these patients.15
Although we found that there was a positive correlation between the corneal endothelial cell loss and the CMV viral load in the aqueous humour, there was no correlation between the viral load and many other ocular signs such as cells and flare in the anterior chamber, types of KPs, gonioscopic findings, IOP, post-treatment visual acuity and the interval from the disease onset to the aqueous sampling. These patients had been treated with topical corticosteroids (eg betamethasone) and anti-glaucoma agents (eg timolol and latanoprost) before they were referred to us by local ophthalmologists. These treatments are known to reduce the intensity of anterior uveitis, IOP and other ocular manifestations, but have no effect on recovering the corneal endothelial cell damage, because the corneal endothelial cell damage is barely reversible.
The cells and flare in the anterior chamber were mild in all 11 patients. A possible explanation why the intensity of the inflammatory reaction in the anterior chamber was so mild in this disease might be related to the involvement of the anterior chamber-associated immune deviation (ACAID).16 17 In an experimental rabbit corneal endotheliitis model, eyes inoculated with inactivated HSV-1 prior to an active HSV-1 infection exhibited less severe inflammatory reactions and corneal endotheliitis. In addition, they also developed an immune deviation to HSV-1.18 Although CMV-related ACAID has not been previously reported, real-time PCR in the present study demonstrated that CMV genomic DNA was present at high levels within the anterior chamber of the patients. Therefore, it may be that ACAID in response to CMV occurs in the eye, resulting in a relatively mild inflammatory reaction.
While our results showed CMV infection in the anterior segment of the eye caused inflammation and corneal endothelial cells loss in immunocompetent hosts, our study cannot answer many other questions. For example, why does CMV cause intraocular inflammation in immunocompetent hosts? Where does the CMV that is detected in the aqueous humour come from? And how is CMV able to cause inflammatory disorder only within the anterior segment of the eye? One possible explanation why our patients developed CMV anterior uveitis is that all our patients had been given topical corticosteroids for a long period of time. This may have contributed to induce local immunosuppressive condition in the anterior segment of the eye and resulted in reactivation of CMV.8 Further clinical and experimental investigations are necessary to clarify these important questions.
In conclusion, significant corneal endothelial cell damage was detected in all CMV-associated iridocyclitis- and corneal endotheliitis-tested eyes. In addition, a significant correlation was found between corneal endothelial cell loss and the CMV viral load in the aqueous humour.
References
Footnotes
Competing interests None.
Ethics approval This study was conducted with the approval of the Institutional Ethics Committee of Tokyo Medical and Dental University.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.