Article Text

Abstract
The ocular surface is a highly dynamic system characterised by continuous adaptive reactions to environmental, toxic, infective, traumatic and inflammatory conditions that interfere with its homeostasis. When the adaptive response is not able to cope with environmental or internal aggressions, a persisting dysfunction may develop into a self-maintaining vicious cycle, thereby developing a chronic disease. This process is not even, but characterised by cycles of worsening and improvement accompanied by morphofunctional changes of the ocular surface structure. The therapy for this condition cannot be unique and stable all along the course of the disease, but should be adapted to the modifications occurring on the ocular surface. It should be long term and dynamic, in order to be tailored on each patient's conditions. An ideal therapeutic strategy should address simultaneously the main targets: tear film quality and stability, morphofunctional changes of the epithelia, the obvious and subclinical inflammation, and the structural and functional changes of nerves.
The avoidance of schematic approaches and the customisation of the therapy, modified according to the disease presentation, will be highly desirable and will open to a patient-oriented approach, granting a more prompt and stable improvement of the ocular surface with better-tolerated therapies.
- Ocular surface
- Tears
- Conjunctiva
- Cornea
- Treatment Medical
Statistics from Altmetric.com
Introduction
The tear film, the epithelia of the cornea and conjunctiva, the lacrimal glands and the eyelids form a system working as a functional unit1 intended to protect the eye from the external environment and provide for an optimal refractive surface of the cornea through the production of an efficient tear film. Box 1 lists the components of this functional unit.
List of ocular surface system components
▸ Lids (meibomian glands, mucocutaneous junction, blinking)
▸ Cornea
▸ Limbus
▸ Conjunctiva
▸ Tear film
▸ Lacrymal glands
▸ Lacrymal drainage system
▸ Lymphatic system
▸ Nerve plexa (trigeminal, facial)
▸ Endocrine control (sex hormones)
The ocular surface system as a whole and its individual components are in a highly dynamic state, in order to meet the changing needs of the different environmental and bodily conditions. In most cases, the reaction to environmental, toxic, infective, traumatic and inflammatory conditions is very quick, effective and able to rebuild the homeostasis of the system. In other cases, when the adaptive response is not able to cope with the aggression, a persisting dysfunction may develop into a self-maintaining vicious cycle.2 In this way the ocular surface dysfunction tends to become a chronic disease. The process is not even, but is typically characterised by cycles of worsening and slight improvement.
Therefore, the therapeutic approach to this condition cannot be unique and stable all along the whole course of the disease, but should be dynamically adapted to the clinical modifications occurring on the ocular surface.
The components of the functional unit are in anatomic continuity and share feedback mechanisms, which result in simultaneous reactions to every single stimulus.
It has been suggested that the neuroanatomic integrations, mediated by the fifth and seventh nerves, play a relevant role in regulating the ocular surface homeostasis together with the input of local and systemic hormones.3 ,4 In this way, stimuli mediated by tactile sensitivity and changes of temperature and pH, together with immune driven prompts, are able to induce a quick compensation for the changes determined by external or internal events.
Sensory (trigeminal) and motor (facial) nervous connections, as well as cytokines, lymphocytes and systemic hormones, guarantee the traffic of information between the different structures, which can either maintain homeostasis or permit fast reactions to new stimuli. The continuous challenge induced by the shearing forces of blinking, air currents, low humidity and foreign bodies, as well as by microorganism attacks, is continuously counterbalanced by the remarkable adaptive abilities of the system. In response to minor stimulation, tear film turnover can increase by up to 500%,5 and corneal epithelial cells can move at rates varying from 17 mm/day to 60 mm/h, according to the ocular surface conditions.6 ,7 For example, a minor wound to the corneal epithelium causes an immediate cascade of events with nervous response resulting in a change of blinking rate, a reflex increase in tear flow, a change in the content of the tear fluid, increased epithelial movement at the corneal surface, increased limbal mitosis, conjunctival capillary dilatation and increased vessel permeability.8 ,9
A stable, duly renovated, properly composed and efficient tear film, a healthy epithelium with its secretory capabilities and an appropriate nerve traffic are mandatory for preserving the ocular surface system attitudes.
A vicious cycle developing in a chronic disease
Pathogenic events that disturb such a homeostasis, whatever their cause (infective, immune, traumatic, surgical or toxic), if not promptly neutralised by appropriate reactions of the ocular surface system, will create, with time, a vicious cycle of events leading to the development of a chronic disease. This self-stimulated loop is characterised by the presence of (1) a progressive failure of tear film stability,10–12 (2) morphofunctional changes of the epithelial structure and its secretory abilities13 and (3) the build-up of subclinic or clinically apparent inflammatory processes involving the bulbar surface as well as the lid margin and the meibomian glands (figure 1).14 As a matter of fact, any persistent epithelial damage will hinder adequate, regular and stable tear film spreading, inducing increased tear evaporation and, possibly, a hyperosmotic shift as well as an increased friction brought by the lid movements over the ocular surface epithelia. This will result in the build-up of an inflammatory cascade. Long-standing ocular surface inflammation will lead to squamous metaplasia of the conjunctiva with loss of its secretory capabilities (MUC5ac, MUC1, MUC4, MUC16, etc) and a more unstable tear film.15 ,16 In a similar way, the presence of an altered meibomian gland secretion is often associated with inflammatory changes of the lid conjunctiva and increased bacterial growth with gland colonisation. With time, especially during the night, when the cleaning ability of the tear fluid is decreased, inflammatory cytokines and bacterial exotoxins will make a patch transferring pro-inflammatory agents from the lid to the bulbar ocular surface. The consequent ocular surface inflammation will begin the vicious cycle, leading to improper tear composition and stability with further inflammation. In this way, a meibomian dysfunction will slowly change into a more diffuse ocular surface dysfunction with tear film disease and metaplastic changes of the conjunctiva. Moreover, a dysfunction of the aqueous phase production will prevent, with time, the normal and efficient spreading of the lipid layer of the film changing the pathogenic pathway of the disease into a mixed form causing further damage and symptoms. The increased inflammatory status can also extend to the lid margin structures, which will enter the disease and become a reservoir of inflammation for the entire system. Up to a certain level, these cascades of events may undergo cyclic changes of worsening and improvement, depending on the ability of the neuroanatomic, immuno and secretory structures to respond to the different environmental and bodily conditions occurring with time. When the reacting ability of the ocular surface system is impaired, as a consequence of external or internal conditions,2 the pathological changes stabilise and cannot be easily reversed. All the described events indicate that the changes of clinical presentations, occurring during the evolution of dry eye, are multifactorial as is dry eye itself.

Tear film instability, epithelial disease and ocular surface inflammation, associated or not to nerve and meibomian gland dysfunction, are the main pathogenic factor of every ocular surface dysfunction. An appropriated therapy should be simultaneously addressed towards all these factors. Priority of target should be defined according to the severity of the clinical presentation and then modified along with the changes in the clinical course. Access the article online to view this figure in colour.
The tear film instability or imbalance, increasing water loss by evaporation, will cause local or diffuse hyperosmolarity of the tear film and, therefore, a stress on the epithelial cells of the cornea and conjunctiva, stimulating the epithelium and the resident inflammatory cells.17 ,18 Corneal and conjunctival cell damage, induced by apoptosis and inflammation consequent to direct mechanical, osmotic or toxic stresses, will stimulate the reflex neurosensory arc, possibly triggering the neurogenic lacrimal gland inflammation and subsequent neurosensory block, with impairment of tear fluid secretion. Inflammatory cytokine release, matrix metalloproteinases activation and inflammatory involvement of the conjunctival epithelium will result in tear film instability and water loss.18 The consequence of this is a lack of efficiency of the tear film to maintain the ocular surface homeostasis, resulting in morphofunctional changes of the ocular surface structures. In the conjunctival mucosa, a goblet cell loss, directly related to the chronic inflammation, and the epithelial cell apoptosis and metaplasia, subsequent to tear film hyperosmolarity and chronic epithelial damage, will result in further tear film instability or imbalance.19 On the other hand, conjunctival flora changes, and the resulting breach of the ocular surface structure, caused by specific diseases or from tear film abnormalities, may trigger the release of endotoxins, lipopolysaccharides and/or lipase, causing activation of the innate immune response through toll-like receptor stimulation20 ,21 and the consequent cascade of events: eyelid inflammation, meibomian gland dysfunction (MGD) and lipidic changes, as well as morphological and functional modifications of ocular surface epithelium, directly jeopardising tear film stability and favouring tear water evaporation.22
Decreased tear production, increased evaporation or altered lid integrity will slow down tear fluid clearance, resulting in further permanence and build-up of toxic and pro-inflammatory agents in the tear film.
It is nowadays clear that several factors can singularly contribute, as starting points, for the development of the ocular surface changes associated to what we call a tear dysfunctional syndrome,2 ,23 which, with time, will establish a self-maintaining process.
The clinical presentation of ocular surface dysfunction: ‘you will never walk alone’
Similar ocular surface alterations can be shown in clinical entities of different aetiopathogenesis.24 For example, a patient with long-standing Sjögren's syndrome will probably show a very thin or absent tear meniscus, with lissamine green staining of the exposed bulbar conjunctiva and cornea, associated or not to MGD. In this case, an appropriate therapeutic strategy should consider: to restore the tear film volume and to control the inflammatory processes leading to or caused by the epithelial and nerve damage. The control of inflammation should pass not only through the use and the modulation of anti-inflammatory agents, but also through the improvement of tear clearance, the protection of the epithelium from the hyperosmotic and traumatic agents and the control of MGD. If available, any therapy addressing nerve health, such as nerve growth factors, autoserum eye drops or vitamin-enriched eye drops formulations, should also be considered.25 ,26
In the case of a patient with primary MGD, it is possible to detect not only an altered quality of the meibum, which may be associated with obvious or non-obvious meibomian gland obstruction, but also a decreased tear film stability and volume, staining of cornea and conjunctiva, incomplete blinking and chronic inflammatory changes of the mucocutaneous junction. Apart from a strict control of MGD, an appropriate therapeutic approach should consider the improvement of the tear film in terms of quantity, lipids spreading, stability and turnover together with a dynamic long-term management of inflammation.
In the case of a patient with a postcataract surgery ocular surface dysfunction, the multiple possible origins of the condition, such as lid margin inflammation, lid tension and their congruity with the bulbar surface, regularity of the surface at the level of the surgical incisions, topical therapy-related toxicity to ocular surface epithelia and the resulting tear instability, should be considered and addressed.
The importance of a complete and precise clinical evaluation
All the previously described conditions should be considered as not stable throughout the whole course of the disease but as developing clinical entities.
The assessment of the actual ocular surface conditions, with the valuation of the degree of involvement of each structure, is mandatory for a successful treatment. In its most simple approach, it should consider: lid characteristics, tear meniscus as indicator of tear volume, break-up time as indicator of tear film stability, fluorescein-stained tear clearance time as indicator of the level of risk of inflammation and epithelial staining as expression of damage and inflammatory involvement.27
Staging ocular surface dysfunction: the diagnostic effort
The tear film-related ocular surface dysfunction has been recently classified into stages by the Delphi Panel and the Dry Eye workshops.23 ,2 On the basis of these classifications, a therapeutic scheme has been provided with suggestions of treatments for each stage of the disease.
Unfortunately, the clinical presentation of many patients does not completely fit into those stages. For instance, a patient with severe, recalcitrant, extensive staining of the conjuntiva in the absence of corneal staining can often be more severe than a patient with MGD, and small area of staining in the lower part of the cornea, which will probably disappear just by treating the meibomian dysfunction.
Furthermore, the clinical picture of the disease can change with time, from one level of staging to another and vice versa, just because of the modifications of lifestyle, environmental28 ,29 and health conditions. In this way, also the staging of the disease across the different clinical evaluations can vary. This variability, if not regarded, will decrease the consistency between the clinical features and the suggested therapeutic approach, which should consider: (1) the clinical expression of the three main factors common to any ocular surface disease (tear film instability, epithelial damage and inflammation) and (2) all the single recognisable causative factors acting on the ocular surface. So, it is important to achieve a proper diagnostic assessment that is able to pick up the alterations of the different ocular surface components as well as the level of their impairment. For this reason, in a therapeutic perspective, it is not sufficient just to make a generic diagnosis of dry eye, but it is much more important to define the clinical staging of the pathological changes in the different structures of the ocular surface system. Such modifications can be encountered whatever be the underlying aetiopathogenic mechanism, and their full recognition is of utmost importance, since several studies have shown that systemic and topic treatments are able to modify the morphofunctional alterations occurring in the course of ocular surface dysfunction.30–39
The ocular surface changes as a guide for an appropriate therapy
Even if the simultaneous presence of tear instability, epithelial disease and inflammatory cascades activation is always there in all the long-standing ocular surface diseases, tear dysfunction syndromes represent a ‘laboratory’ for the search of an appropriate therapeutic approach to the ocular surface system diseases.
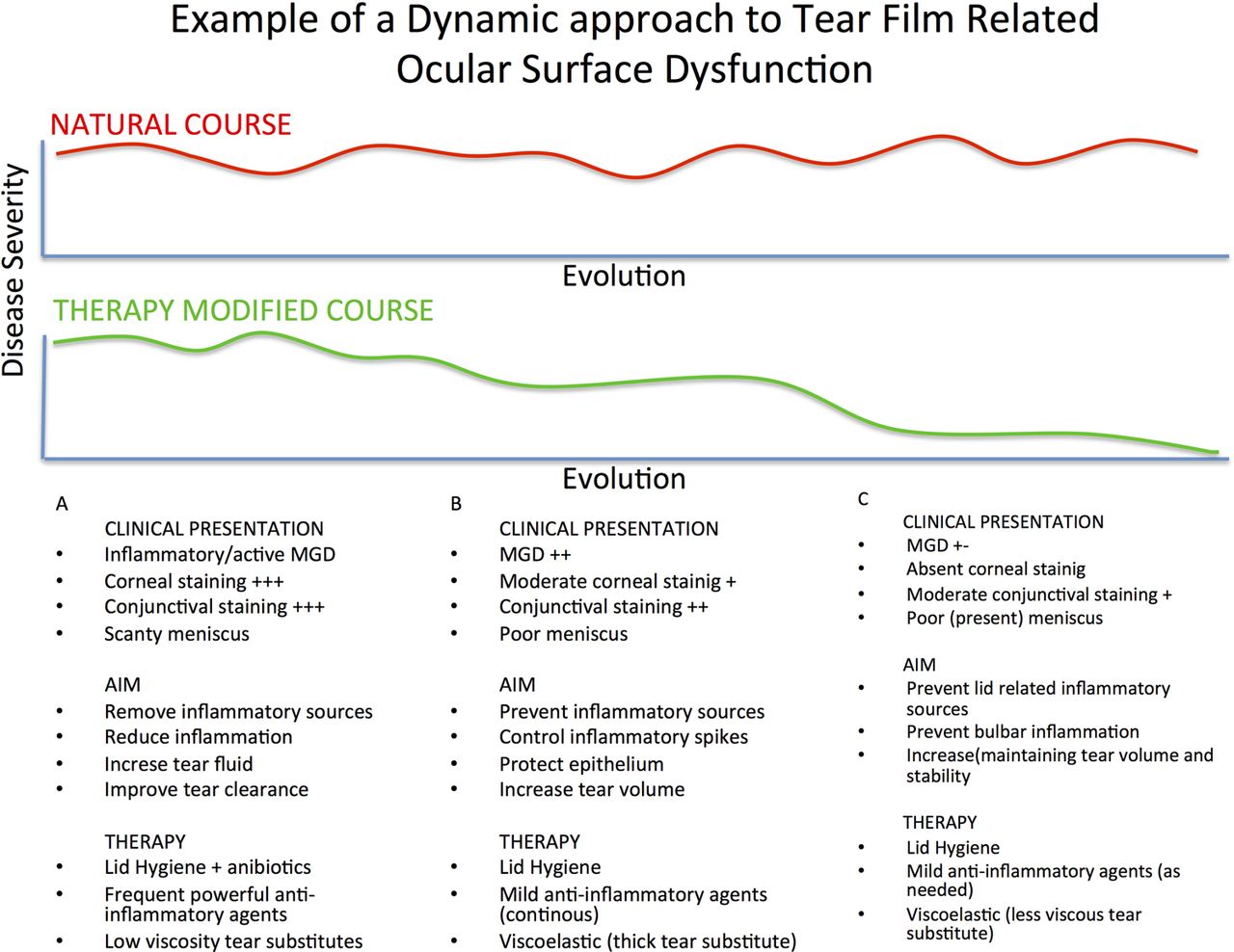
The therapeutic strategy adopted for treating ocular surface dysfunctions should be built on the basis of the clinical observations and should consider, as primary targets, the most clinically relevant signs (figure 2). Therefore, a single-action therapy will not be sufficient for an effective correction of ocular surface dysfunctions and the therapy should be changed along the course of the disease, as the clinical presentations will progressively change as a result of both the development of the disease and/or of the applied therapy. Furthermore, as already described by Bron et al,24 the neuroimmunoendocrine regulation of the ocular surface system accounts for possible variations of the phenotype of dry eye, even along the course of the disease. At this evolution concur genetic, environmental and bodily conditions also as a consequence of the therapy used.40 These factors and the evolution that they may induce on the clinical course of the disease should be taken into account, in order to establish the appropriate therapeutic adjustments. Therefore, a proper assessment of the actual clinical condition and the need of a timely and precisely oriented therapeutic approach to the changing ocular surface conditions are of the utmost importance. For instance, in a hyposecretory dry eye, the tear volume, especially the clearance of tear film content should be increased in order to clean the pro-inflammatory agents from the ocular surface. Also, the presence of an active, patent meibomian gland inflammation should be addressed aggressively, as a first step, because the inflammation can be quickly transferred to the bulbar structures and tear film. When inflammation has slowed down, epithelial damage and corneal and conjunctival conditions should be further re-addressed, by using a more viscous and long-lasting tear substitute, while the anti-inflammatory topical therapy should be tapered in terms of strength and frequency. Of course, lid hygiene should be performed and continued regularly.

{kind=link}
{kind=link}
Example of a possible strategy of the therapeutic approach to the ocular surface disease in a patient with tear deficiency and active meibomian gland dysfunction. The upper diagram represents the natural course of the disease with the typical variations with time, in absence of therapy. The lower diagram represents the variations of the clinical presentations induced by dynamic adaptation of the therapy along the course of the disease. (A) The clinical presentation, aim of the therapy and therapeutic modalities at presentation. (B) The clinical presentation has been modified by the efficacy of the therapy; the aim of the therapy is then changed accordingly and a new therapy is prescribed. (C) The clinical presentation is further modified so also the aim of the therapy is shifted towards maintenance of the ocular surface homeostasis and a new milder, long-term maintenance treatment is prescribed. Access the article online to view this figure in colour.
In the same way, since a punctate keratitis will greatly interfere with the ability of maintaining and spreading an efficient tear film over the cornea, the correction of the epithelial damage, by means of anti-inflammatory drugs and highly viscous tear substitutes will allow, once reached the epithelial correction, to use less powerful and risky anti-inflammatory drugs and more fluid and better accepted tear substitutes. Therefore, in a patient showing extensive punctuate corneal damage and conjunctival staining, as it is clear that a long-lasting fluid adhesion is not possible over such a damaged epithelium, the epithelial structural changes should be addressed first. For example, in filamentary keratitis, the use of tear substitutes alone is usually not satisfactory as the accurate removal of the mucoepithelial filaments is mandatory, with the temporary use of silicon hydrogel bandage contact lenses or a semi-compressive patching, associated with anti-inflammatory agents. Then, as the surface has improved, tear substitutes, which appeared not really effective before, can be usefully applied. Similarly, punctum plugs could be temporarily effective for recovering ocular surface damages related to the lack of fluid, but their removal should be considered when the surface has improved, due to the increased risk of inflammation linked to poor tear clearance.
The same dynamic therapeutic procedure may be used in many other conditions requiring the use of tear substitutes. Sometimes, at presentation, dilution of the tear fluid is necessary to remove the toxic pro-inflammatory factors from the ocular surface; then, a more viscoelastic tear substitute has to be preferred in order to improve the lubrication problems and the correlated symptoms. In the same way, a thicker mucoadhesive tear substitute should be used in cases requiring special epithelial protection even if it is sometimes not so well tolerated by the patient. This will be changed into a less viscous preparation, vision-wise better accepted, when epithelial improvement has been obtained.
Because of the multifactorial characteristics of the disease, the therapeutic approach has to be multiple and long standing, with the possible risks of toxicity and deleterious impact on the quality of life of the patients, resulting in a poor compliance and outcome. Hence, a clinically guided, dynamic therapeutic strategy should be designed and applied.
Conclusions
The existing therapeutic schemes for the treatment of ocular surface dysfunction (Delphi panel, DEWS, MGD Workshop) suggest a number of therapeutic tools indicated for each stage of ocular surface dysfunction. They do not explain how to use the therapies proposed for the treatment of the several stages. It is mandatory to consider the actual status of each ocular surface structure in order to adapt the proper therapeutic intervention, which must be modified as the ocular surface condition changes. In this way, there is not one fixed therapeutic scheme useful for the disease in all the phases of its evolution or even a scheme useful for every single stage of the disease but, rather, an approach considering the changes occurring in every single ocular surface structure, in order to address them specifically. The therapy that could be adapted to the patient's conditions at one stage of the disease should be probably changed as long as the disease develops.
Therefore, the concept of dynamic therapy for ocular surface dysfunctions can fit as an integration of the existing proposed approaches.
The ocular surface dysfunctions are chronic diseases, with an uneven course, characterised by alternating phases of improvement and worsening, which are accompanied by morphofunctional changes of the ocular surface structures. Therefore, the therapy should be long term and dynamic, in order to be tailored on the modifications of the clinical presentation. An ideal therapeutic strategy should address simultaneously the main targets: tear film quality and stability, morphofunctional changes of the epithelia, the obvious and subclinical inflammation as well as the ocular surface nerve structural and functional changes.
An effective therapy for ocular surface dysfunction will modify the anatomic substrate so that, when the aimed outcomes are reached, the therapy itself should be remodelled accordingly. A dynamic approach, to be effective, implies the necessity of a better knowledge and understanding of the characteristics of the single preparations prescribed, in order to achieve the expected goals and to avoid therapeutic failures.
Also, it should be kept in mind that any long-term therapy has an intrinsic risk of toxicity: active principles and their formulations, preservatives, too high frequency of instillation, could be the source of unexpected adverse events, which might complicate the clinical feature leading to diagnostic misinterpretations and therapeutic mistakes.
Box 2 summarises the key points for a dynamic treatment of ocular surface dysfunctions.
Milestones for a dynamic therapeutic approach to ocular surface dysfunctions
▸ Ocular surface dysfunctions are chronic diseases
▸ Therapy should be long term and aimed at the recovery of ocular surface homeostasis
▸ Ocular surface diseases are multifactorial, all the factors should be addressed by the therapy
▸ The ocular surface is a system: therapy should address simultaneously tear film changes, epithelial disease, clinical and subclinical inflammation and nerve changes
▸ Avoid schematic treatments
▸ Adapt the therapy to the current clinical presentation
▸ Therapy should be modified according to the changes of the anatomic substrate induced also by an ongoing treatment
▸ Long-term therapy, if not well modulated, is at risk of inducing side effects
The avoidance of schematic approaches to ocular surface dysfunctions is highly desirable. This means that the proposal of therapeutic protocols specific for each stage of ocular surface dysfunction should be considered only as a general indication of possible intervention that should be always adapted to the changes occurring in every single ocular surface structure, in order to address them specifically. The customisation of the therapy, tailored on the current clinical presentation of the patient and modified according to the evolution of the disease, will warrant a more prompt and stable improvement of the ocular surface with bettertolerated treatments.
Acknowledgments
The authors thank Dr Sebastiano Giuffrida of Bausch & Lomb for its support to the development of the concept of a Dynamic Therapy for ocular surface disease.
References
Footnotes
-
Contributors Both authors equally contributed to the manuscript.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.