Article Text

Abstract
Purpose To measure the dimensions of aqueous outflow structures and to investigate associations with intraocular pressure (IOP) and ocular biometry parameters in an older British population.
Method Fifty-two participants from the European Prospective Investigation of Cancer-Norfolk eye study underwent imaging using the Heidelberg Spectralis optical coherence tomographer with an anterior segment module. Pseudophakic participants and those known or suspected to have glaucoma were excluded, leaving 46 participants for analysis. Schwalbe's line (SL), scleral spur (SS), Schlemm's canal (SC) diameter and the trabecular meshwork cross-sectional area (TM cross-sectional area (CSA)) were identified and traced using ImageJ software. IOP was measured using the Ocular Response Analyser. Ocular biometry was measured by partial coherence interferometry.
Results The mean (SD) subject age was 65.7 years (5.6). The SL and SS were identifiable in all nasal and temporal scans. The mean SL–SS distance was 800 μm (104) nasally and 808 μm (102) temporally. Repeatability of SS–SL, SS–SC, SC and TM CSA was good to excellent, and reproducibility fair to good. Nasal SL–SS distance was inversely associated with anterior chamber depth (ACD) (p=0.007, −116 μm per mm ACD, R2=0.18). Multiple linear regression showed nasal TM CSA was significantly associated with age and IOP (age: p=0.025, 0.007 mm2 per decade of age; IOP: p=0.029, −0.0012 mm2 per mm Hg, R2=0.23).
Conclusions Aqueous outflow structures can be measured by optical coherence tomography, and their dimensions vary significantly with ocular biometric characteristics and IOP. Further investigation is required to determine associations between outflow structure sizes in different populations and pathologies, including ocular hypertension and glaucoma.
- Angle
- Epidemiology
- Intraocular pressure
- Imaging
- Glaucoma
Statistics from Altmetric.com
Introduction
Intraocular pressure (IOP) remains the most important modifiable risk factor for glaucoma and its modulation has been shown to influence both glaucoma onset1 and progression.2–4 Increased outflow resistance was proposed as the cause of elevated IOP by Leber in 1873,5 yet the underlying pathophysiology of this characteristic still remains unclear.6 In humans, the majority (65–90%) of the aqueous humour drains through the trabecular (conventional outflow) route that comprises the trabecular meshwork (TM), Schlemm's canal (SC) and the collector channels and aqueous veins. Anterior segment optical coherence tomography (OCT) allows rapid in vivo non-contact qualitative and quantitative assessment of the human anterior chamber, and recent improvements in scan resolution have enabled the identification of aqueous outflow structures including the TM and SC.7–10 Scan resolution is determined by the wavelength of the light source, with shorter wavelengths providing higher resolution images; this is, however, at the expense of depth penetration. Spaide et al11 described the technique of enhanced depth imaging (EDI) for the Spectralis OCT equipment (Heidelberg Engineering, Heidelberg, Germany), which increases the imaging sensitivity of deeper structures, and EDI is now built into the Spectralis OCT software. The Spectralis OCT with the anterior segment module has a scan beam of 870 nm in central wavelength with digital axial resolution of 3.9 μm and a transverse resolution of 10 μm for anterior segment imaging.12
The aim of this study was to provide normative values of aqueous outflow structure dimensions and to determine whether these are associated with other ocular biometric parameters and IOP in a sub group of the EPIC-Norfolk eye study.
Method
EPIC (European Prospective Investigation of Cancer) is a pan-European study that started in 1989 with the primary aim of investigating the relationship between diet and cancer risk.13 The EPIC-Norfolk cohort was broadened to include additional endpoints and exposures. The EPIC-Norfolk cohort was recruited in 1993–1997 and comprised 25 633 predominantly white European participants aged between 40 and 79 years old. The third health check (HC3) examination was between 2006 and 2011, with the objective of investigating various physical and ocular characteristics of participants who were now aged 48–91 years. The HC3 was reviewed and approved by the East Norfolk and Waverney NHS Research Governance Committee (2005EC07L) and the Norfolk Research Ethics Committee (05/Q0101/191) and was performed in accordance with the principles of the Declaration of Helsinki. All participants gave written, informed consent.
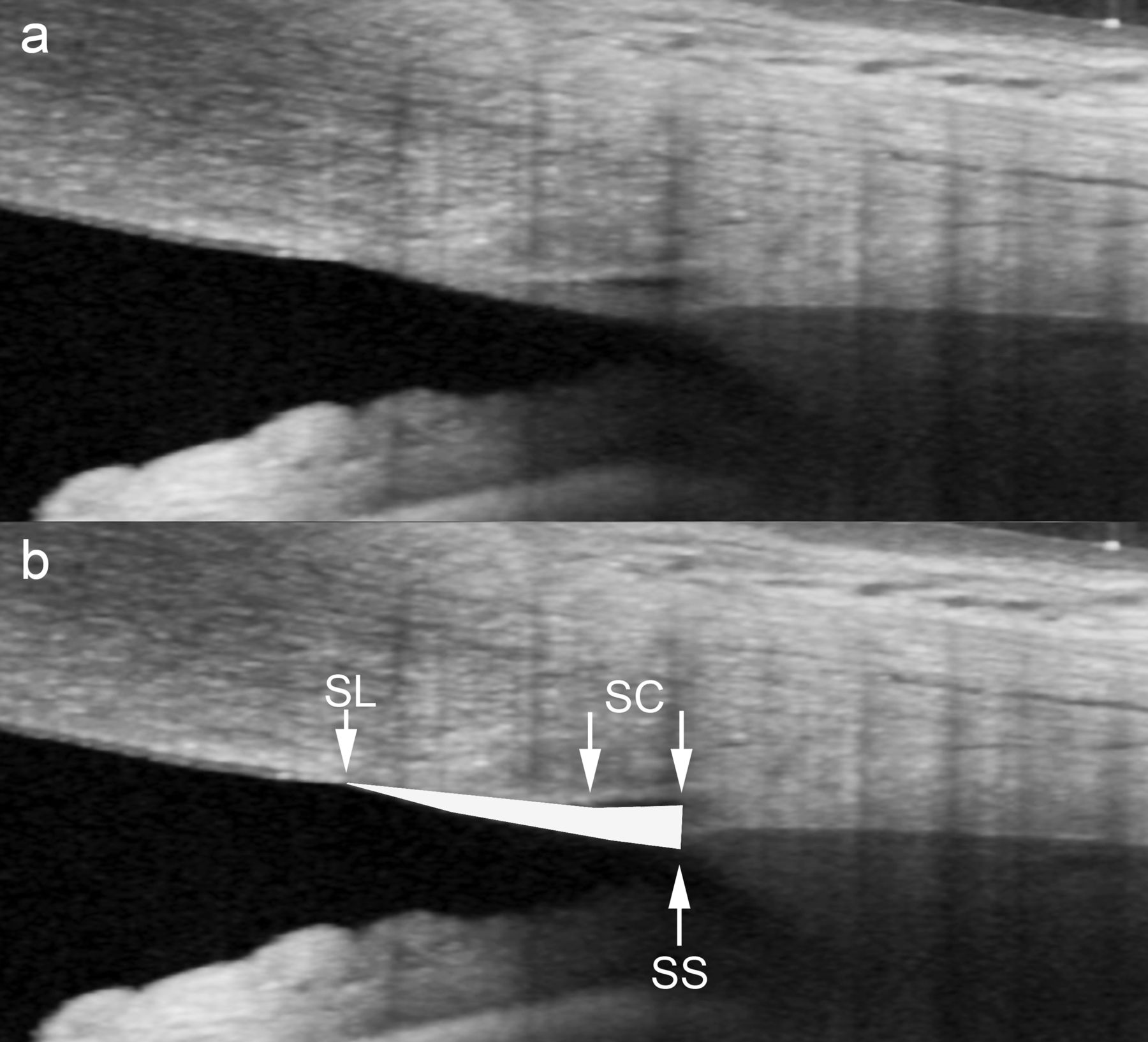
A detailed health examination was performed by nurses following standard operating procedures. All clinical examinations were performed on consecutive participants attending HC3 over a 3-week period in November–December 2011. A stadiometer was used to record the participants’ height to the nearest 0.1 cm and weight was measured to the nearest 0.1 kg using a body composition analyser (Tanita model TBF 300s, Chasmors Ltd, London, UK). IOP was measured three times using the non-contact Ocular Response Analyser (ORA, Reichert Inc, Depew, New York, USA), and the mean Goldmann-correlated IOP was calculated. Ocular biometry was measured by non-contact partial coherence inferometry using the Zeiss IOLMaster Optical Biometer (Carl Zeiss Meditech Ltd, Welwyn Garden City, UK). Five measurements of axial length (AL) and anterior chamber depth (ACD, anterior corneal surface to anterior lens surface), and three measurements of central keratometry were made to calculate the mean values. Refractive error was measured using an autorefractor (Humphrey model 500, Humphrey Instruments, San Leandro, California, USA) and subjects classified as hyperopic (+1.0 dioptres (D) or more) or myopic (−1.0 or more). Systolic and diastolic blood pressure (BP) was taken from the right arm with the participant seated for 5 min. Ocular perfusion pressure was calculated as two-thirds of the mean arterial pressure minus IOP (mean arterial pressure was calculated from diastolic BP plus one third of the difference between systolic and diastolic BP). OCT imaging was performed in all cases by the same investigator (AD) in standardised scotopic (<1.0 lux) conditions using Spectralis OCT equipment with an anterior segment module. Images were acquired at the 3 o'clock and 9 o'clock positions of the right eye with 30° abduction and 30° adduction, respectively, using fixed distance fixation targets. Eight-mm line scans were performed with EDI and automatic real time image averaging modes activated (40 B-scans averaged). All scans were processed by Heidelberg Spectralis OCT software V.5.3, which automatically corrects for curvature of the anterior ocular surface. B-scan images were imported into ImageJ (V.1.45s, National Institutes of Health, USA; http://rsb.info.nih.gov/ij/index.html) to enable measurement. Contrast adjustment and bi-thresholding were subjectively adjusted to optimise identification of these structures if required. TM cross-sectional area (CSA) was calculated using an automated ImageJ area function. Schwalbe's line (SL) was defined as the site of termination of the monolayer corneal endothelium/Descemet's membrane. We defined the scleral spur (SS) as the end point of the curved interface between the ciliary body and the sclera/TM based on previous studies.14 SS to SC was defined as the distance between SS and the most posterior part of SC. SC diameter was defined as the distance between the most posterior and anterior part of SC directly adjacent to the TM (see figure 1B). TM CSA was drawn freehand depicting an area bounded by the SL, SS, SC posterior, SC anterior and SL (see figure 1). Data on pseudophakic participants and those known or suspected to have glaucoma were excluded from analysis.

(A) A typical scan image acquired using the Spectralis anterior segment module. (B) The location of Schwalbe's line, the scleral spur and Schlemm's canal and the trabecular meshwork cross-sectional area demarcation (fill).
Scan images were measured by two observers who had previously assessed 20 sample images together to ensure a similar understanding of the anatomical landmarks. All subsequent measurements were performed independently and without reference to those assessed previously. Observer 1 had significant experience with the Spectralis OCT with anterior segment module from a previous pilot study, Observer 2 had no previous experience of the Spectralis OCT unit, but had interpreted images from other anterior segment OCT devices. For intraobserver repeatability, Observer one repeated all measurements 2 weeks later. As all OCT measurements are subject to observer variability, intraobserver and interobserver variability was assessed with the coefficient of repeatability and 95% limits of agreement15 and intraclass correlation coefficients (ICC). Outflow structure dimensions were compared by linear regression and t-tests using the average of Observer 1's initial and repeat values. Normality assumptions for all OCT parameters were checked. Interobserver agreement was calculated by comparing Observer 1's initial values to Observer 2's values. Agreement of categorical variables was determined using Kappa statistics and percent agreement.16 All statistical analyses were performed using SPSS Statistics V.19 or GraphPad Prism V.5.
Results
Fifty-two participants underwent Spectralis anterior segment OCT imaging. All participants were of white European descent. Six participants were excluded from analysis due to pseudophakia (n=3) and treatment for glaucoma (n=3). The locations of the SL and SS were identifiable in all 46 nasal and 46 temporal scans (100%). Participant demographics, and biometric and aqueous outflow structure values are shown in table 1.
European Prospective Investigation of Cancer-Norfolk Eye Study participant demographic, biometric and aqueous outflow structure parameters with mean, SD, 95% CI and range
Table 2 shows the intraobserver measurement error15 (within subject SDs) and coefficients of repeatability15 (the difference between intraobserver measurements for 95% pairs of observations) for SL–SS, SS–SC, SC diameter and TM CSA for both nasal and temporal scans. ICC scores with lower 95% CIs in parentheses are also shown for comparison. Table 2 also shows the interobserver limits of agreement15 (with values as a percentage of the mean in italics), bias (with SD, and the bias value as a percentage of mean in italics) and ICC with lower 95% CIs in parentheses. Bland–Altman plots15 are shown in figure 3 (see online supplementary web-only data). Overall, we found repeatability to be good to excellent and reproducibility to be fair to good.
Intraobserver measurement error, coefficient of repeatability (and as a percentage of the range of measured values, shown in italics) and intraclass correlation coefficients (with lower 95% CI in brackets); and interobserver limits of agreement (and as a percentage of the range of measured values, shown in italics), bias and intraclass correlation coefficients (with lower 95% CI shown in brackets)
Repeatability/reproducibility:
SC was identifiable (allowing SL–SC length, SC diameter and TM CSA to be calculated) in 40/46 (87%) nasal scans and 39/46 (85%) temporal scans (Observer 1's initial and repeat readings) and 40/46 (87%) nasal and temporal scans (Observer 2). The κ values for judgment of a measurable SC for the intraobserver measurements were 0.81 nasal and 1.00 temporal. For interobserver measurements, the κ values were 1.00 for nasal and 0.73 for temporal; both of these suggest at least good agreement.
Analysis of outflow structure dimensions with biometry and IOP:
Linear regression showed that nasal SL–SS distance was significantly associated with ACD (p=0.007, −116 μm per mm ACD, R2=0.18; see figure 2A). There was no association with any other parameter, including AL and IOP, even with ACD in the model. Temporal SL–SS distance was not associated with ACD or any other parameter, except for AL, where it almost reached statistical significance (p=0.053, 31 μm per mm AL, R2=0.08, see figure 2B). This became statistically significant with ACD in the model (p=0.014, 48 μm per mm AL, R2=0.16).

{kind=link}
{kind=link}
Linear regressions of nasal and temporal aqueous outflow structure dimensions (Schwalbe's line to scleral spur distance, scleral spur to Schlemm's canal (SC) distance, SC diameter and trabecular meshwork cross-sectional area compared to demographic and biometric parameters including age, anterior chamber depth, axial length and intraocular pressure. Corresponding p-values for the regression lines, 95% CIs and R2 values are shown.
Univariate linear regressions showed that the nasal SS–SC distance was significantly associated with ACD only (p=0.024, 41 μm per mm ACD, R2=0.15, see figure 2C), although there was a positive association with age that did not reach statistical significance (p=0.072, 21 μm per decade of age, R2=0.08). Multiple linear regression showed that only ACD and age were associated with nasal SS–SC distance (ACD: 42 μm SS–SC per mm ACD, p=0.013; age: 25 μm per decade of age, p=0.032; overall R2=0.27). In addition, temporal SS–SC distance was significantly associated with ACD (p=0.034, 41 μm per mm ACD, R2=0.14) but not age (see figure 2D).
Regression of nasal and temporal SC diameter showed a non-significant trend for reducing size with IOP (figure 2E, nasal: p=0.081, −6 μm per mm Hg, R2=0.08; temporal: p=0.13).
Nasal TM CSA was significantly associated with age (p=0.027, 0.008 mm2 per decade of age, R2=0.12; see figure 2F) and inversely associated with IOP (p=0.023, −0.0013 mm2 per mm Hg, R2=0.13; see figure 2G) on univariate linear regression. Multiple linear regression showed that nasal TM CSA was significantly associated with age and IOP (age: p=0.025, 0.007 mm2 per decade of age; IOP: p=0.029, −0.0012 mm2 per mm Hg, R2=0.23). Temporal TM CSA was not associated with age or IOP, but was associated with ACD (p=0.023, 0.0189 mm2 per mm ACD, R2=0.16; see figure 2H).
No association between any aqueous outflow dimensions and sex, refractive error (hyperopia or myopia), systolic or diastolic BP, height, weight or mean keratometry were identified. Ocular perfusion pressure showed a positive trend with increasing nasal TM CSA (p=0.083, 0.005 mm2 TM CSA per 10mm Hg ocular perfusion pressure, R2=0.08).
Discussion
Nasal TM CSA was significantly greater in older subjects and was inversely related to IOP. There is little histological data in humans for comparison; however, Alvarado et al17 showed that TM CSA tended to be greater in older subjects (p=0.087). We are not aware of other studies reporting an association between TM CSA and function, although a UBM study by Stegman et al18 in 1986 reported that TM length (SS–SL distance) was significantly less in patients with juvenile primary open angle glaucoma when compared to healthy controls.
We found that nasal SL–SS distance was inversely related to ACD (p=0.007). This was unexpected, as one would assume that in a larger anterior segment, all components would be proportionately larger. Possible explanations would include the finding that mean IOP is higher in myopia compared to emmetropia,19 that myopia onset in childhood may be related to restricted equatorial growth20 or that as anterior chamber circumference is greater in larger eyes, a narrower SL–SS distance is required for the equivalent internal TM area. We found no significant association between temporal SL–SS distance and ACD; however, SL–SS did show an increasing trend with increasing AL (p=0.053). Differences between nasal and temporal quadrant findings are difficult to explain and are probably due to the relatively small number of participants. However it is also plausible that quadrant differences may be related to different rates of embryological development and/or growth changes of the eye between the nasal and temporal sides. Nasal and temporal SS–SC distance significantly increased with increasing ACD. This suggests that TM cross-sectional shape differs between eyes with ACD, although overall TM CSA does not.
Until recently, there were almost no data on in vivo human trabecular outflow pathway dimensions and, to date, there are no values from population-based studies for comparison. Last year, Cheung et al10 reported that using a modified Cirrus spectral domain OCT, the SL could be identified in 95% scans and the SS could be identified in 85% scans. They also found no difference in SL–SS distance between subjects with open angles compared to closed angles. A recent study by Usui et al9 using the SS-1000 Casia OCT reported that the SS could be identified in all subjects but the SL was only identifiable in 32% subjects. They also found no difference in TM length, TM area or SC diameter between nasal and temporal measurements, or any association with age, refractive error, AL or ACD. As seen in table 3, our values for SL–SS are consistent with those reported by Tun et al,21 but are higher than those reported by Stegman18 and by Usui.9 Our TM CSA values were consistent with those reported by Usui.
Comparison of studies reporting in vivo measures of the human trabecular meshwork (TM) and Schlemm's canal (SC)
In the present study, the observers were confident that the SC could be identified in up to 87% of scans. Usui et al9 reported that the SC was observable in 90% cases, while Kagemann et al8 identified the SC in 100% of normal subjects. Kagemann et al8 also found the nasal SC area to be significantly larger than the temporal SC area, consistent with the results of the present study where nasal SC diameter was found to be significantly greater than temporal SC diameter (p=0.001).
There are many differences in study methodology between the present study and those previously describing in vivo outflow structure dimensions. Usui et al9 defined TM length as the meridional AL between the SS and the anterior endpoint of the TM, which itself was defined as the point of intersection of the SC line and Descemet's membrane (rather than the SL). In the present study, the SS was defined as the end point of the curved interface between the ciliary body and the sclera/TM based on previous studies.14 All participants in the present study were of white European descent from a community cohort study, whereas the others were from hospital-based cohorts.
The primary limitation of the present study is the small number of participants. This study was designed to be a pilot study providing initial quantitative parameters on aqueous outflow pathway structure dimensions. As the EPIC-Norfolk third health check ended in December 2011, it was not possible to image additional participants. In the present study, IOP was measured using the ORA, despite the accepted gold standard technique for measuring IOP being Goldmann applanation tonometry (GAT). However, there is good agreement between GAT and ORA Goldmann-correlated IOP,23 and the repeatability of ORA IOP measurements is comparable to that of GAT.24 Relative to posterior segment OCT imaging, anterior segment OCT imaging and analysis is still in its infancy, and its features differ markedly between software versions and manufacturers. Consequently, assumptions have to be made when using commercially available machines. Automatic image dewarping, in particular, may affect measurements; however, this is unlikely to be significant, as the aqueous outflow structures we have investigated are in the initial refractive plane and imaging was performed close to perpendicular to the ocular surface over their location. Another limitation relates to the fact that the TM and SC are only part of the aqueous outflow pathway, and distal outflow structures such as collector channels and intrascleral vasculature are currently poorly resolved on commercially available OCT imaging devices, so that no quantitative or qualitative analysis is possible. Imaging of these distal outflow structures has been reported in vivo using a customised OCT unit by Kagemann et al.8 Additionally, aqueous outflow structure dimensions may vary by location, and our values were from line scans at the horizontal meridians rather than composite values derived from volume scans. Finally, it must be remembered that SL–SS distance is an incomplete description of TM length, as it effectively excludes the posterior portion behind the spur limited by the spur, chamber angle and the meshwork insertion of the ciliary muscle.25
This study shows that aqueous outflow structures can be measured non-invasively in living participants and, despite small participant study numbers, their dimensions vary significantly with ocular biometric characteristics and IOP. Further investigation is required to determine the associations between aqueous outflow structure sizes in different populations and pathologies including ocular hypertension and glaucoma.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figure
Footnotes
-
Contributors ACD designed the study, undertook the statistical analysis and data interpretation, and wrote the first draft. DFG-H, DCB, YJ, SH, ND, K-TK and PJF were involved in the conception and design of the study. YJ, PJF and DFG-H were also involved in the analysis and interpretation of the data. All authors were responsible for revising the article for important intellectual content and approval of the final version.
-
Funding Supported by Grant G0401527 from the Medical Research Council, UK and Grant 262 from Research into Ageing, UK. PJF was also supported by the Richard Desmond Charitable Trust (via Fight for Sight, grant 1956). ACD, DFG-H & PJF were supported by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Moorfields Eye Hospital NHS Foundation Trust and University College London Institute of Ophthalmology. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
-
Competing interests None.
-
Ethics approval The East Norfolk and Waverney NHS Research Governance Committee (2005EC07L) and the Norfolk Research Ethics Committee (05/Q0101/191).
-
Provenance and peer review Not commissioned; externally peer reviewed.