Article Text

Abstract
Aim To evaluate the role of intravitreal aflibercept injection as a treatment for eyes with chronic central serous chorioretinopathy (CSCR).
Methods This prospective pilot study enrolled 12 patients with chronic CSCR who received a 6-month treatment regimen of intravitreal aflibercept. Patients were followed with monthly Early Treatment of Diabetic Retinopathy Study (ETDRS) best-corrected visual acuity (BCVA) and spectral domain optical coherence tomography (SD-OCT) with enhanced depth imaging.
Results All patients were men between 29 and 64 years (median 55). Subfoveal fluid was present on OCT for a median duration of 6 months (range 4–29 months) prior to treatment. Baseline BCVA ranged from 20/25 to 20/160 (median 20/50) with a mean of 62 (SD=13) ETDRS letters. No patients experienced serious ocular or systemic adverse events over the course of the study. Post-treatment BCVA ranged from 20/20 to 20/200 (median 20/40), with a mean of 64 (SD=16) ETDRS letters (p=0.56). At baseline, three patients (25%) had BCVA of ≥20/40 versus seven patients (58%) at the conclusion of the study. Two patients gained at least 15 ETDRS letters and no patients lost more than 15 ETDRS letters. Six of 12 patients (50%) had complete resolution of subfoveal fluid. Mean central macular thickness decreased from 400 µm (SD=104 µm) to 306 µm (SD=94 µm) (p=0.03), and mean subfoveal fluid decreased from 159 µm (SD=93 µm) to 49 µm (SD=68 µm) (p=0.02). Mean choroidal thickness decreased from 307 µm (SD=72 µm) to 263 µm (SD=63 µm) (p=0.0003).
Conclusions Intravitreal aflibercept was well tolerated over a 6-month treatment course for chronic CSCR. No change was observed in visual acuity metrics. Anatomic trends may suggest some morphological activity, but larger controlled trials are needed.
Trial registration number NCT01710332
- Choroid
- Macula
- Retina
- Treatment Medical
Statistics from Altmetric.com
Introduction
Central serous chorioretinopathy (CSCR) is a relatively common cause of visual impairment in the Western world.1 Patients can present with a variety of visual symptoms including relative central scotoma, metamorphopsia, dyschromatopsia and micropsia.2 ,3 On examination, the characteristic finding is a posterior neurosensory retinal detachment caused by leakage of fluid from the level of the retinal pigment epithelium (RPE).
The typical natural history of CSCR is complete spontaneous resolution of subretinal fluid with complete or near-complete restoration of visual acuity by 3 months after onset of symptoms. However, up to 20% of patients may have persistent serous macular detachment and vision loss past 6 months, and may be left with some degree of subjective visual impairment such as micropsia or reduced colour perception.4 ,5 If subretinal fluid has not resolved by 3 months, and the possibility of exogenous local or systemic corticosteroid use or other rare systemic diseases has been exhausted, the patient is defined as having persistent or chronic CSCR, and treatment is often considered.
There is no ‘gold standard’ for treatment of persistent CSCR, and a number of therapies have been tried with varying success rates. Focal photocoagulation to pinpoint areas of leakage on fluorescein angiography (FA) was the first treatment shown to be of some benefit for hastening resolution of CSCR.6 However, photocoagulation is destructive and can lead to symptomatic scotomas and, occasionally, formation of secondary choroidal neovascularisation. Therefore, this treatment is typically reserved for discreet extrafoveal foci of leakage seen on FA. Photodynamic therapy (PDT) more directly targets the choroidal circulation and may be used in patients with subfoveal or multifocal points of leakage. Although PDT has been used for persistent CSCR with some success, it is not Food and Drug Administration (FDA) approved for treatment of CSCR. PDT also has a number of potential side effects including photosensitivity to intravenous dye and choroidal hypoperfusion after treatment.7 ,8 Other medical treatments have also been explored, but results are inconsistent and difficult to interpret. Most recently, systemic mineralocorticoid antagonism was reported to potentially accelerate anatomic improvement in patients with CSCR, and further studies are ongoing.9 ,10
Intravitreal antivascular endothelial growth factor (anti-VEGF) medications have become mainstays of therapy in neovascular age-related macular degeneration (AMD), macular oedema secondary to retinal vascular occlusion and diabetic macular oedema. Anti-VEGF medications have a number of effects that reduce vascular leakage in these conditions, including the upregulation of tight junctions between endothelial cells and reduction of vascular fenestrations.11 Side effects of these medications are minimal when locally administered; the major ocular adverse event associated with intravitreal injections is endophthalmitis occurring in approximately 1/2000 injections.12
A study by Lim et al13 suggested that VEGF levels in the aqueous humour of patients with persistent CSCR may be elevated compared with normal eyes. Case studies of intravitreal anti-VEGF medications in patients with persistent or chronic CSCR have found improvements in visual acuity, neurosensory detachment resolutions and improvements in RPE leaks on FA.14 ,15 However, prospective studies using anti-VEGF medications for CSCR have shown mixed results.16 ,17
Aflibercept (Eylea, Regeneron Pharmaceuticals, Tarrytown, New York, USA) is an anti-VEGF medication that is FDA approved for the treatment of neovascular AMD and macular oedema secondary to central retinal vein occlusion and diabetic retinopathy. Pharmacokinetic modelling of this treatment demonstrated prolonged VEGF binding activity compared with other commonly used intravitreal treatments for neovascular AMD.18 Additionally, aflibercept inhibits the activity of subtypes VEGF-A and VEGF-B, as well as placental growth factor (PlGF).19 There are currently no published case reports or series using aflibercept in patients with CSCR. The purpose of this pilot study is to investigate the tolerability and possible role of intravitreal aflibercept injections for the treatment of chronic CSCR.
Methods
This prospective, open-label, single-centre, randomised, investigator sponsored clinical study was approved by the institutional review board of the Wills Eye Hospital and was conducted in accordance with the tenets of the Declaration of Helsinki. Informed consent was obtained from each participant prior to enrolment. This study was registered at clinicaltrials.gov as NCT01710332 on 16 October 2012.
Study population
This study enrolled patients over a 6-month recruitment period (November 2012 to May 2013). Criteria for inclusion included: (1) age ≥18 years, (2) ability to provide informed consent, (3) persistent CSCR demonstrated by subfoveal fluid (SFF) on optical coherence tomography (OCT) for greater than 3 months, (4) active leakage on FA at the time of enrolment, (5) evidence of hyperpermeability and abnormal dilation of choroidal vasculature on indocyanine green angiography (ICGA) and (6) best-corrected visual acuity (BCVA) between 20/25 and 20/320. Only one eye for each patient was included in patients with bilateral CSCR.
Exclusion criteria for the study were: (1) concurrent progressive retinal or substantial ocular disease in the study eye, (2) prior treatment for CSCR in the study eye (anti-VEGF, PDT or laser) within 3 months prior to enrolment, (3) presence of choroidal neovascularisation or polypoidal choroidal vasculopathy on enrolment imaging, (4) history of intraocular surgery except uncomplicated cataract surgery >3 months prior to enrolment, (5) prior treatment with systemic anti-VEGF agents or steroid agents within the preceding 12 months, (6) uncontrolled glaucoma, (7) history of cerebrovascular accident or myocardial infarction and (8) pregnancy.
Study visits and imaging
At screening, past ocular and medical histories were recorded and vital signs were measured. The occurrence of adverse events was assessed at each visit. Baseline and monthly ophthalmic examinations included BCVA, applanation tonometry, and anterior segment and dilated fundus examinations by a member of the Retina Service of Wills Eye Hospital. Technicians performed: (1) monthly BCVA using the Early Treatment of Diabetic Retinopathy Study (ETDRS) at 4 m, (2) monthly spectral domain OCT (SD-OCT) including enhanced depth imaging (Heidelberg Engineering, Heidelberg, Germany) and (3) FA, ICGA and fundus autofluorescence (Heidelberg Engineering, Heidelberg, Germany) at baseline and month 6 (closeout visit).
Central macular thickness (CMT) was automatically calculated by the Heidelberg software. Retinal boundaries were adjusted if there was misalignment of the computer algorithm. SFF height was determined by a masked observer (JDP) using the digital calliper function to measure distance from the hyper-reflective RPE to the photoreceptor outer segments on a b-scan through the foveal centre point. Choroidal thickness was determined by a masked observer (JDP) using the digital calliper to measure distance from the inner border of the choroido–scleral interface to the hyper-reflective RPE. This task was performed on an enhanced depth imaging (EDI) b-scan through the foveal centre point where the choroido–scleral junction was clearly defined.
Study treatment
Patients were randomised to two groups: intravitreal injections of aflibercept 2.0 mg/0.05 mL at month 0, 1, 2, 3, 4 and 5 (group 1, n=6) or intravitreal injections of aflibercept 2.0 mg/0.05 mL at month 0, 1, 2 and 4 (group 2, n=6). Treatment was withheld for intraocular pressure greater than 30 mm Hg, ocular surface infection, intraocular inflammation, vitreous haemorrhage, endophthalmitis, new retinal detachment or macular hole.
Outcome measures and statistical analysis
The outcome measures were: (1) the occurrence of ocular or systemic adverse events, (2) mean change from baseline in ETDRS letter score, (3) percentage of eyes with 20/40 or better vision, (4) percentage of eyes with ≥15-letter gain from baseline, (5) percentage of eyes with <15-letter loss from baseline, (6) mean change in CMT, (7) mean change in SFF manually measured by a masked observer (JDP), (8) percentage of eyes with complete resolution of macular fluid on OCT, (9) mean change in subfoveal choroidal thickness as measured via enhanced depth imaging and (10) percentage of eyes with absence of leakage on FA. Quantitative variables were compared at baseline visit versus 6 months using two-tailed paired t test.
Results
Patients
A total of 12 patients were enrolled. Baseline characteristics are detailed in table 1. All patients were men between the ages of 29 and 64 years (median 55). No patients had systemic steroid exposure or treatment for CSCR within 6 months prior to enrolment. SFF was present on OCT for a median duration of 6 months (range 4–31 months) prior to treatment.
Baseline patient characteristics
Treatment tolerance
No patients experienced adverse events over the course of the study. There were no cases of endophthalmitis or retinal detachment.
Visual acuity
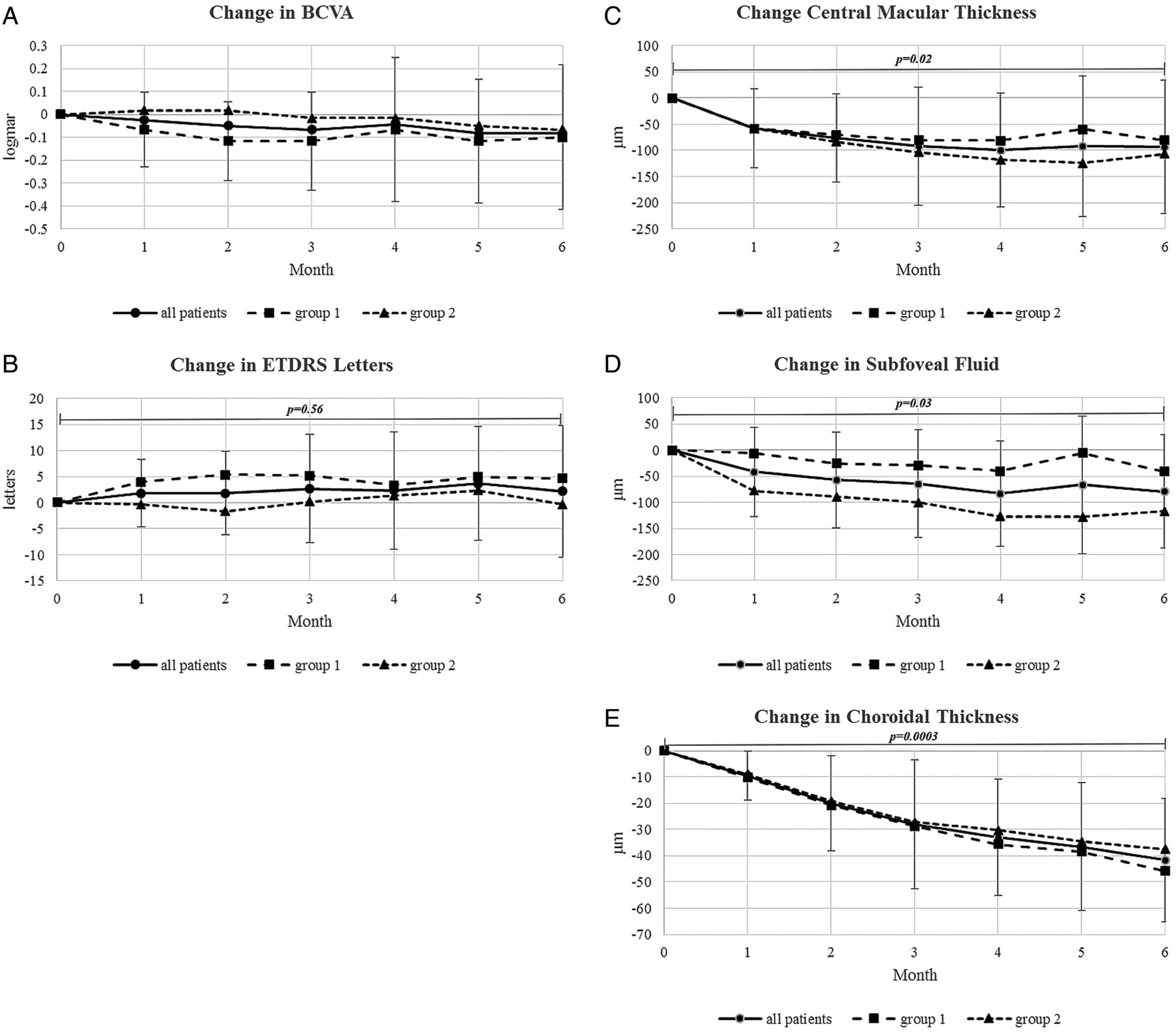
Baseline BCVA ranged from 20/25 to 20/160 (median 20/50), with a mean of 62 (SD=13) ETDRS letters. Post-treatment data are summarised in table 2. Final BCVA ranged from 20/20 to 20/200 (median 20/40), with a mean of 64 (SD=16) ETDRS letters (p=0.56; figure 1A, B). At baseline, three patients (25%) had BCVA of ≥20/40 versus seven patients (58%) at the conclusion of the study. Two patients gained at least 15 ETDRS letters and no patient lost more than 15 ETDRS letters. There was no statistically significant difference in visual acuity outcomes between group 1 and group 2 (p=0.5).
Individual patient visual acuity and anatomic outcomes

(A) Mean change in best-corrected visual acuity (BCVA); (B) mean change in Early Treatment of Diabetic Retinopathy Study (ETDRS) letter score; (C) mean change in central macular thickness; (D) mean change in subfoveal fluid; and (E) mean change in choroidal thickness. Error bars represent SD for the all-patient data points. p Values are for mean differences between baseline and 6 months for all-patient data points.
Anatomic metrics
Mean CMT decreased from 400 µm (SD=104 µm) to 306 µm (SD=94 µm) (p=0.03; figure 1C), and measured mean SFF decreased from 159 µm (SD=93 µm) to 49 µm (SD=68 µm) (p=0.02; figure 1D). Mean subfoveal choroidal thickness decreased from 307 µm (SD=72 µm) to 263 µm (SD=63 µm) (p=0.0003; figure 1E). Six of 12 patients (50%) had complete resolution of SFF at the conclusion of the study (figure 2). The correlation coefficient (R2) between change in choroidal thickness and change in SFF was 0.21. Leakage on FA resolved in eight of 12 patients (75%). There was no statistically significant difference in any of the anatomic outcomes between group 1 and group 2 (p>0.4 for all OCT measurements).
{kind=link}
{kind=link}
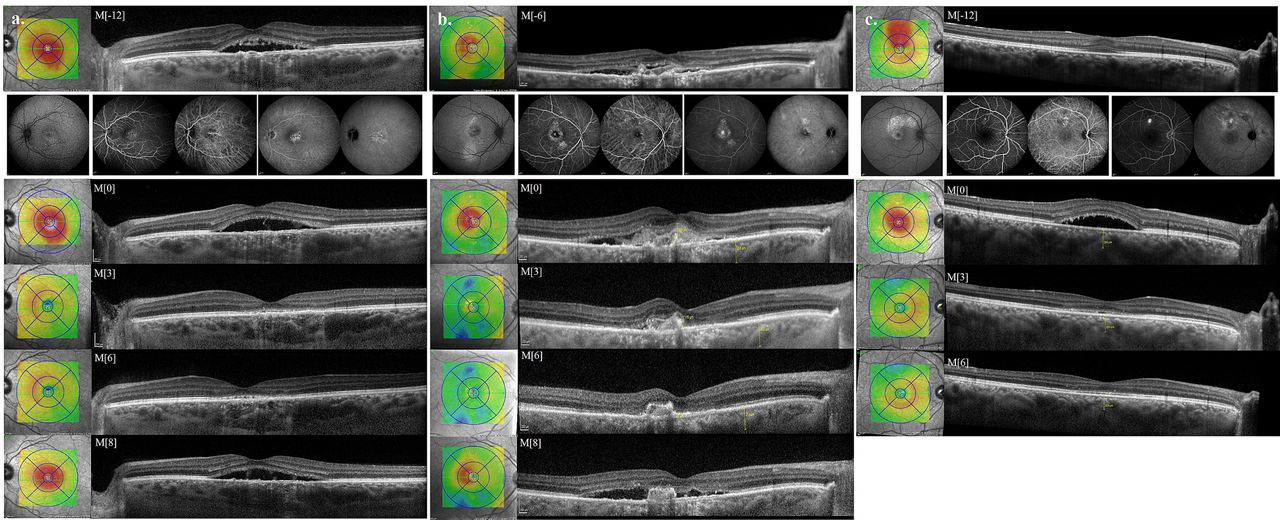
(A–C) Three patients with chronic central serous chorioretinopathy as demonstrated by persistent subfoveal fluid (SFF) at least 6 months prior to enrolment. All had resolution of SFF by month 3 (M[3]). Two of these patients (A and B) had recurrence of SFF 2 months following discontinuation of treatment (M[8]).
Discussion
Despite being well tolerated and theoretically beneficial in CSCR, published reports of the results of intravitreal anti-VEGF treatment for this condition have been inconsistent. A recent meta-analysis of controlled trials using intravitreal bevacizumab failed to reveal a benefit in either BCVA or CMT.20 A randomised trial using ranibizumab likewise demonstrated a suboptimal response in chronic CSCR, and ranibizumab was found to be inferior to PDT in improving both anatomy and vision in chronic CSCR.14 To the best of our knowledge, this is the first investigation of intravitreal aflibercept injection as a treatment for chronic CSCR.
Aflibercept is a fusion protein with some intrinsic differences from other anti-VEGF agents that affect its activity in vivo. Unlike ranibizumab, aflibercept binds the VEGF-B isoform, which plays a role in maintenance of blood vessels in some pathological conditions.21 It also binds PlGF 1 and 2, which have distinct expression patterns and mechanisms of action in human retinal development.22 ,23 Some molecular studies have suggested that PlGF may actually have the greatest pathological effect by preferentially occupying VEGF-R1 binding sites, allowing VEGF-A to activate VEGF-R2.24
Phase III clinical trials for AMD showed that bimonthly dosing of aflibercept was non-inferior and clinically equivalent to monthly ranibizumab, and that pro re nata injections at year 2 were less frequent than ranibizumab.25 Using this rationale, we randomised patients with chronic CSCR into two groups: (1) monthly aflibercept injections for 6 months (six total treatments) or (2) 3-monthly aflibercept injections (‘loading phase’), then one injection 2 months later (modelled after the ‘2q8’ dosing in the VIEW studies of aflibercept for AMD).
Our protocol included a total of 60 intravitreal injections of aflibercept to 12 patients over the duration of the study. No patient experienced any serious ocular or systemic adverse events. No patient withdrew from the study. No cases of endophthalmitis, retinal detachment, cataract progression or elevation in intraocular pressure were encountered.
Mean BCVA and ETDRS letter score did not change with treatment. This could be attributed to the chronicity of CSCR and longstanding and recurrent SFF in these patients. In the eyes with complete resolution of SFF, SD-OCT imaging continued to demonstrate disruption of the ellipsoid and interdigitation zones of the photoreceptor–RPE complex (figure 2). There may also be a component of delayed visual recovery lagging behind anatomic improvement, out of the scope of this 6-month pilot study.
Imamura et al26 first reported thickened subfoveal choroidal measurements with EDI-OCT in patients with CSCR. The pathophysiological mechanism of this finding and its relationship to the disease remain under investigation. We noted a decrease in choroidal thickness over the course of treatment with aflibercept. This trend corresponded to a reduction in CMT and SFF. Three patients had complete resolution of SFF by month 3 (figure 2), while three others were dry by months 4–6. This rate of improvement may be similar to that reported for PDT and potentially more rapid than reported for ranibizumab.14 There was no strong correlation between change in choroidal thickness and change in SFF.
This study is limited by the small sample size. Additionally, we did not randomise any patients to a control group. The natural history of acute CSCR is resolution of serous retinal detachment. We only enrolled patients with chronic CSCR as indicated by persistence of subretinal fluid for greater than 3 months duration (range 4–31 months). In this small study, a sham-injection group was not feasible.
Our study represents the first using aflibercept intravitreal injections as a therapy for chronic CSCR. Treatment was well tolerated with no adverse events. Visual acuity did not change significantly from baseline. Anatomic metrics may indicate some morphological activity, but larger controlled studies are needed. We did not detect any differences between dosing groups, suggesting that, following initial loading doses, a less than monthly treatment strategy may be sufficient.
References
Footnotes
-
Contributors All four authors were involved in the study design and execution as well as preparation of this manuscript.
-
Funding This study was supported by a grant from Regeneron Pharmaceuticals.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance