Article Text

Abstract
Topic To quantify the gain in visual acuity and serious side effects of ranibizumab, bevacizumab and aflibercept in age-related macular degeneration (AMD).
Clinical relevance There is an ongoing debate about the optimal treatment of AMD with these three antivascular endothelial growth factor (anti-VEGF) treatments.
Methods Network meta-analyses. (Pre)Medline, EMBASE, SCOPUS, Cochrane Library (until April 2013), Science Citation Index and reference lists were searched for placebo-controlled randomised trials or head-to-head comparisons. Outcomes were 1-year follow-up data of visual acuity (letters gained) and serious (vascular death, any death, stroke, myocardial infarction, transient ischaemic attack) and thrombotic events. Two investigators independently assessed eligibility and quality of included studies and extracted data.
Results 11 trials (enrolling 8341 patients) assessing five active treatments were included. Compared with placebo, all anti-VEGF treatments had a significantly higher percentage of letters gained: ranibizumab 0.3 mg 2.39% (95% CI 1.59 to 3.19; p<0.001), ranibizumab 0.5 mg 3.56% (95% CI 2.58 to 4.13; p<0.001), bevacizumab 1.25 mg 2.14% (95% CI 0.47 to 3.82; p=0.012), aflibercept 0.5 mg 2.91% (95% CI 0.99 to 4.82; p=0.003) and aflibercept 2 mg 3.44% (95% CI 1.73 to 5.14; p<0.001). Compared with placebo, serious side effects were higher in all other treatments: ranibizumab 0.3 mg 4.41% (95% CI 3.42 to 5.40; p<0.001), ranibizumab 0.5 mg 5.33% (95% CI 4.37 to 6.30; p<0.001), bevacizumab 1.25 mg 5.58% (95% CI 3.567 to 7.60; p<0.001), aflibercept 0.5 mg 5.65% (95% CI (3.28 to 8.02; p<0.001) and aflibercept 2 mg 5.29% (95% CI 3.18 to 7.39; p<0.001). Compared with placebo, systemic thrombotic events also occurred more often in all other treatments.
Conclusions The study revealed only a modest superiority of aflibercept 2 mg and ranibizumab 0.5 mg over other formulations and dosages.
- Macula
- Treatment Medical
Statistics from Altmetric.com
Background
The availability of new drugs in the management of patients with age-related macular degeneration (AMD) has raised a question about the optimal treatment strategy. The discovery of new molecules, inhibitors of angiogenesis, raised the hope for new treatment modalities with the potential to revolutionise the management of patients with AMD (reviewed in1 ,2). To date, three closely related antivascular endothelial growth factor-A (anti-VEGF-A) molecules are in the market. Ranibizumab and aflibercept are licensed for the treatment of AMD while bevacizumab is frequently used in an off-labelled manner in AMD.
In 2011, a large trial assessed ranibizumab and bevacizumab3 and in 2012 two prospective, double-masked, parallel-group randomised clinical trials compared the 5-year results of intravitreal aflibercept monthly or every 2 months with monthly ranibizumab (VIEW 1 and VIEW 2).4 Despite an increasing body of evidence, the book regarding the best treatment remains open. Several systematic reviews were unable to provide an answer about the most effective intervention in AMD management because they did not integrate all available randomised evidence into one analysis or did not assess all currently available treatments.
In this paper, we unify the results from two network meta-analyses assessing the various treatment options for AMD management. The approach allows the joint assessment of all randomised controlled trials quantifying the efficacy and serious side effects of these agents in a head-to-head fashion while fully respecting randomisation.5–7 The analysis includes all commonly prescribed treatments and quantifies the effects on visual acuity and serious (vascular death, any death, stroke, myocardial infarction, transient ischaemic attack) and thrombotic events. We provide charts benchmarking efficacy against serious side effects for all assessed medications and dosages.
Methods
This systematic review followed the PRISMA statement.8 Ethics approval was not required for this network meta-analysis because only published data were included.
Eligibility criteria for considering studies for this review
We included randomised controlled trials comparing aflibercept, bevacizumab or ranibizumab against placebo or in a head-to-head fashion. Studies had to include 1-year follow-up data of visual acuity and serious side effects.
Search methods for identifying studies
To identify randomised controlled trials, we applied an iterative approach combining electronic database and hand searches. The search strategy was designed in collaboration with an information specialist. We searched papers in Medline, Premedline, EMBASE, SCOPUS and the Cochrane Library. Searches were performed separately for papers examining the efficacy and serious side effects of aflibercept, bevacizumab and ranibizumab in patients with AMD. The search was last updated in June 2013. From papers qualifying for inclusion we examined related articles using the related article function available on the PubMed Medline interface. Moreover, we checked for articles citing three seminal papers9–11 using the Science Citation Index Database. Examination of reference lists of included studies and review articles12–15 complemented our searches. The Medline search strategy is available in the online supplementary appendix.
Data collection and risk of bias assessment
In duplicate, we extracted salient methodological features (description of generation of random sequence and concealment of random allocation, blinding of patients and caregivers, whether the analysis was based on the intention to treat principle and the proportion of patient lost during follow-up), patient characteristics (patients’ age, previous laser treatment of AMD, type and size of membranes), and treatments and dosages of each paper. Discordant extractions were discussed. This was the case in 18 instances and was due to an over-reading.
Outcome measures
Efficacy
The most consistently reported efficacy outcome was increase in letters gained. We chose this outcome for this network meta-analysis.
Side effects
We initially extracted all reported serious side effects from each included study. In a second step, we selected those that were at least reported three times and were considered as serious. The analysis thus considered the following five outcomes: vascular death, any death, stroke, myocardial infarction and transient ischaemic attack. In a separate analysis, we looked at systemic thrombotic events.
Data synthesis and analysis
Details about this statistical approach and its application have been published elsewhere.7 ,16
Efficacy analysis
Results from intention to treat analysis were considered wherever possible.
We imputed missing SDs of mean changes for each treatment using the largest SD reported in the set of included studies for this outcome. This was necessary in four cases. For each participant, we simulated the outcome by sampling from a normal distribution with mean and SD of the outcome in a specific treatment arm as described in the study report. Due to chance, the mean and SD parameters could be different from the original values. We corrected these differences using a linear transformation. We generated such a dataset for all the treatment arms. This approach led to the same likelihood functions as that from the original data. To this new dataset, a linear regression model was fitted. Drug and dosage, creating a unique code for each treatment, were entered as covariates. An indicator variate for each study was entered to the model to preserve randomisation within each trial. This variate adjusted for all the possible differences (patients and design) between studies.
Side effects analysis
For each of the serious side effects and each of the treatment arms, the number of events was added up and then divided by the total number of patients in the corresponding treatment arm. Thus, the events per patient in each of the trials given a specific treatment and dosage were determined. The total score of serious side effects was calculated by adding up these estimates of all serious side effects. For the sum of serious side effects outcomes, a linear regression analysis was performed with drug, dosage and an indicator for the studies as covariates.7 As a substitute for the inverse of the variance, we weighted the analysis with the total number of patients in each treatment arm.
Trade-off analysis
For efficacy, we looked at number of letters gained. This efficacy parameter was each plotted against serious side effects and thrombotic events from the network meta-analysis. Results were calculated as percentage differences against placebo. Analyses were performed with the Stata SE V.11.2 software package (Copyright 1996–2010 StataCorp LP, 4905 Lakeway Drive, College Station, TX 77845, USA).
Results
Study characteristics
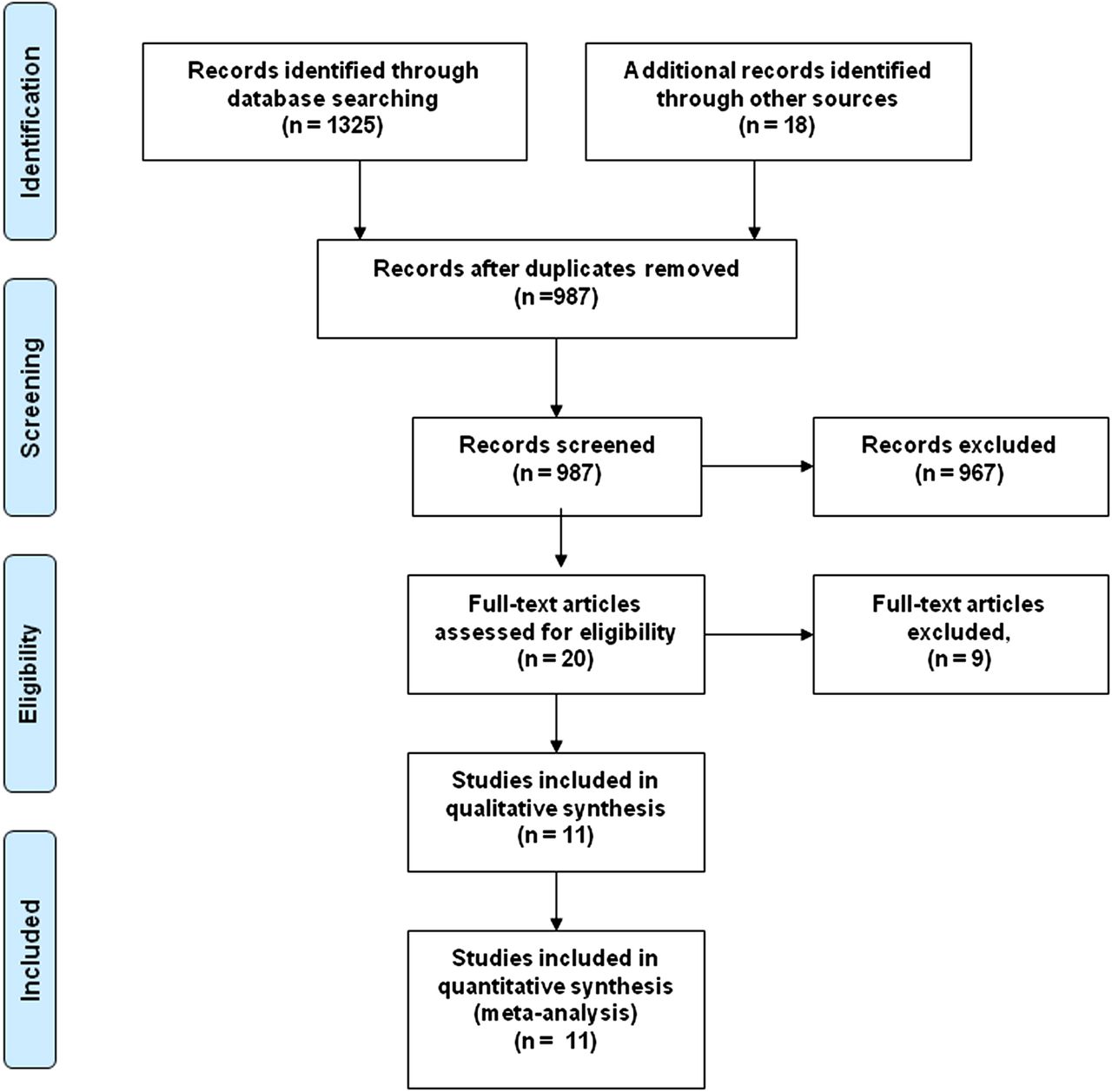
Eleven trials assessing five active treatments (ranibizumab 0.3 mg, ranibizumab 0.5 mg, bevacizumab 1.25 mg, aflibercept 0.5 mg and aflibercept 2 mg) were included enrolling 8341 patients3 ,4 ,9–11 ,17–21 (for details of records selection please see figure 1). On average, patients were 76.7 years old, and 57% of study participants were women. On placebo/sham treatment were 294 patients, ranibizumab 0.3 mg was assessed in 1782 patients and ranibizumab 0.5 mg in 3566 patients. Bevacizumab was assessed in 882 patients, aflibercept 0.5 mg in 597 patients and aflibercept 2 mg in 1220 patients (table 1).
Summary of included studies and treatments assessed
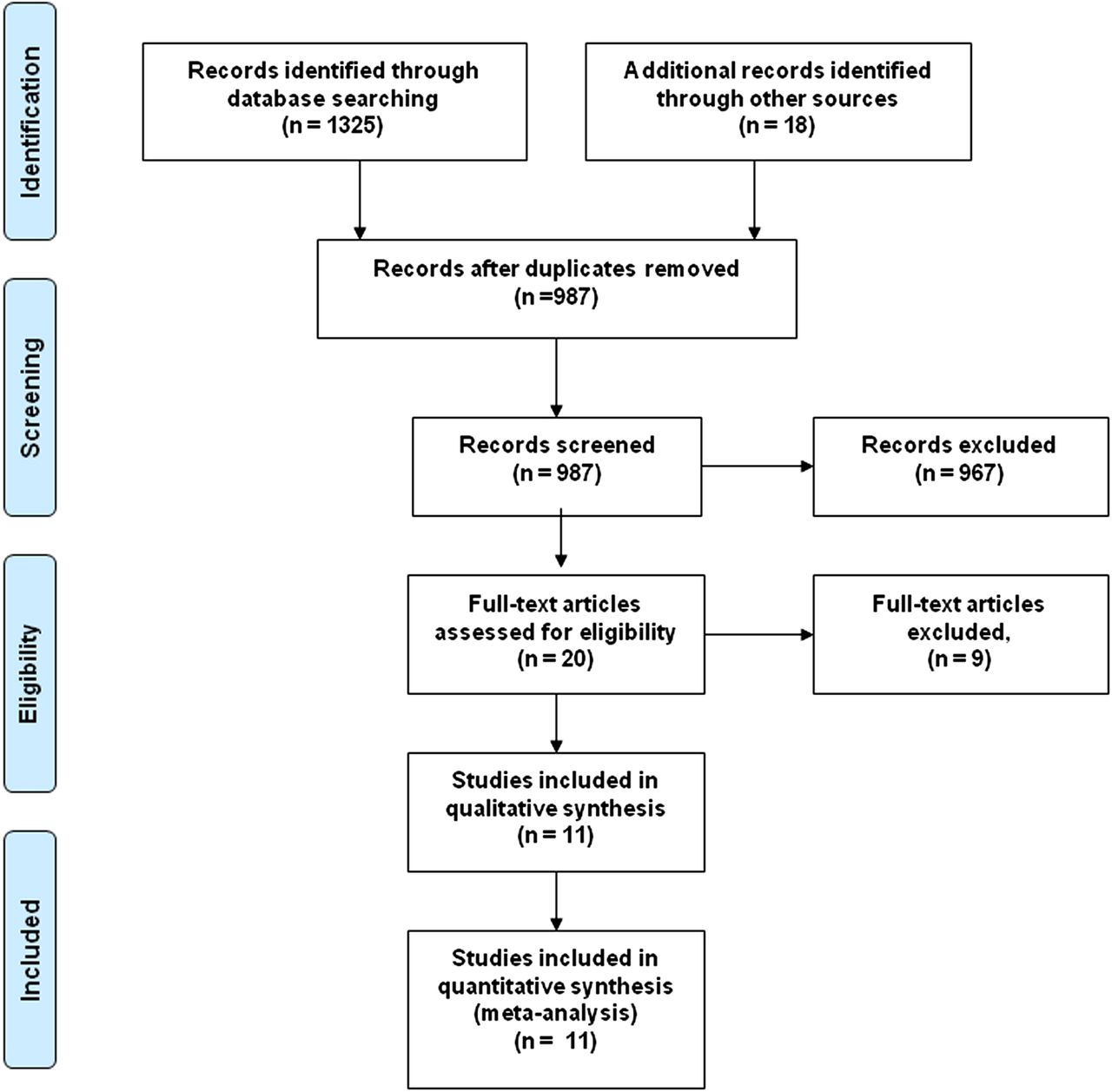
PRISMA flow diagram.
Efficacy and serious side effects
Letters gained
Compared with placebo, all anti-VEGF treatments had a significantly higher percentage of letters gained: ranibizumab 0.3 mg 2.39% (95% CI 1.59 to 3.19; p<0.001), ranibizumab 0.5 mg 3.56% (95% CI 2.58 to 4.13; p<0.001), bevacizumab 1.25 mg 2.14% (95% CI 0.47 to 3.82; p=0.012), aflibercept 0.5 mg 2.91% (95% CI 0.99 to 4.82; p=0.003) and aflibercept 2 mg 3.44% (95% CI 1.73 to 5.14; p<0.001).
Serious side effects
Compared with placebo, serious side effects were higher in all other treatments: ranibizumab 0.3 mg 4.41% (95% CI 3.42 to 5.40; p<0.001), ranibizumab 0.5 mg 5.33% (95% CI 4.37 to 6.30; p<0.001), bevacizumab 1.25 mg 5.58% (95% CI 3.567 to 7.60; p<0.001), aflibercept 0.5 mg 5.65% (95% CI 3.28 to 8.02; p<0.001) and aflibercept 2 mg 5.29% (95% CI 3.18 to 7.39; p<0.001).
Systemic thrombotic events
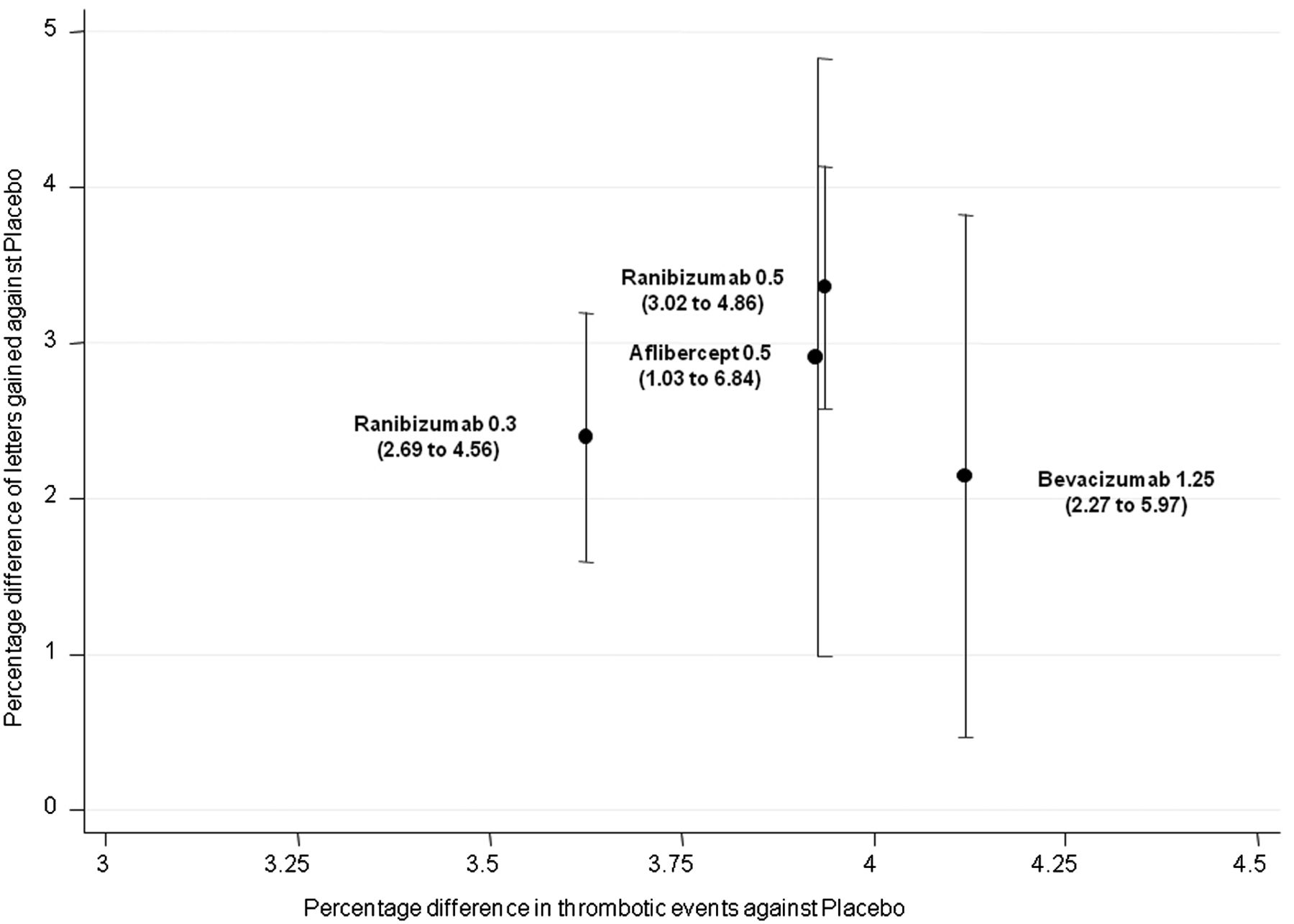
Compared with placebo, systemic thrombotic events also occurred more often in all other treatments: ranibizumab 0.3 mg 3.63% (95% CI 2.69 to 4.56; p<0.001), ranibizumab 0.5 mg 3.94% (95% CI 3.02 to 4.86; p<0.001), bevacizumab 1.25 mg 4.12% 95% CI (2.27 to 5.97; p<0.001) and aflibercept 0.5 mg 3.94% (95% CI 1.03 to 6.84; p=0.008). For aflibercept 2 mg, no estimates could be calculated.
Trade-off analysis
Figures 2 and 3 show the relationship between the efficacy and serious side effects for various treatments and dosages against placebo. In figure 2, contrasting the percentage gain of letters with the percentage difference in severe side effects, the two higher dosages of ranibizumab and aflibercept show slightly higher efficacy than ranibizumab 0.3 mg at the cost of higher percentages of serious side effects. While aflibercept 0.5 mg is slightly more efficient than ranibizumab 0.3 mg, bevacizumab 1.25 mg is not. Both formulations show higher percentages of side effects than all other treatments. Bevacizumab 1.25 mg has slightly higher albeit not significantly different rates (p=0.559) of systemic thrombotic events without being superior to any other treatment investigated (figure 3).

A trade-off chart of the relationship between letters gained and serious side effects (vascular death, any death, stroke, myocardial infarction, transient ischaemic attack) of various antivascular endothelial growth factor (anti-VEGF) treatments. Compared with placebo, all treatments show higher percentages of serious side effects. Aflibercept 2 mg and ranibizumab 0.5 mg show similar profiles. Values in parenthesis indicate 95% CIs for serious side effects.
{kind=link}
{kind=link}
{kind=link}
A trade-off chart of the relationship between letters gained and thrombotic events of various antivascular endothelial growth factor (anti-VEGF treatments)*. Values in parenthesis indicate 95% CIs for thrombotic events. *No effect sizes of aflibercept 2 mg could be estimated.
Discussion
Main findings
This trade-off analysis provides a comparison of efficacy and severe side effects for all currently used anti-VEGF formulations involving over 8000 patients with AMD. Upon review, there is no treatment clearly standing out. Differences between the various treatments are rather small. The study revealed only a modest superiority of aflibercept 2 mg and ranibizumab 0.5 mg against other formulations and dosages. Bevacizumab 1.25 mg showed no additional efficacy compared with ranibizumab 0.3 mg but had a higher rate of serious side effects.
Results in the context of other findings
We are aware of one previous network meta-analysis of five trials (ANCHOR, FOCUS, MARINA, VISION, ABC) published as a letter in 2011 assessing the efficacy of bevacizumab, ranibizumab, pegaptanib and verteporfin.22 The authors concluded that anti-VEGF treatment is superior to conventional treatment (photodynamic therapy and verteporfin) and that ranibizumab and bevacizumab showed no difference in effectiveness. While being partly in agreement with this study, our analysis provides further insight because it assessed all currently prescribed anti-VEGF formulations and also combined the efficacy information with severe side effects, which is seen as the most relevant difference between the various formulations. We found that bevacizumab has some disadvantages in severe side effects compared with the other anti-VEGF formulations that are licensed for AMD treatment. The efficacy and side effects profiles of ranibizumab 0.5 mg and aflibercept 2 mg are very similar.
Strength and limitations
The methods applied in this paper allow making steps beyond conventional reviews. The approach incorporates all available information from clinical trials while fully maintaining randomisation. Moreover, the combination of efficacy and serious side effects provides the evidence base for formal decision-analytic models.
The major limitation of this study lies in the reporting quality of some studies. For example, precision estimates (SDs and CIs) were missing for some papers and forced us to impute some value in order to use the data. For missing SDs of continuous efficacy outcomes, we decided to use the highest SD reported within a specific outcome domain resulting in a more conservative estimation of treatment effects. For the side effects analysis, the within study variance of the event scores were not available and, therefore, a customary meta- analysis investigating heterogeneity was not possible. To account for this, we assumed heterogeneity and allowed that the variance of the outcome parameter included the between and the within study variance.
Given that our data represent averaged severe side effects of the anti-VEGFs, it is unclear how predictive the mean values are for an individual patient. Likewise, we found no information about the number of patients experiencing two or more side effects. Therefore, we had to assume that the occurrence of a side effect was independent of the presence of another, although this might be more complex in clinical reality. Moreover, policy and completeness of side effects reporting differed between the trials. The impact of this variability on the results is impossible to determine, but under-reporting of side effects is possible. It is known that monthly treatment is the most effective treatment whereas all ‘as needed’ treatment schemes are less effective. In this analysis, we were unable to provide separate analyses of side effects for the two treatment schemes due to the level of reporting. The efficacy and side effect data represent a mixture of the two. Consequently, the analysis rather represents the regimen effectiveness than the drug effectiveness. Finally, due to an inconsistent reporting of letters gained per injection, we were unable to investigate whether the claimed advantage of aflibercept 2 mg of being equally effective than ranibizumab 0.5 mg with less injections actually materialises. In theory, aflibercept has an advantage over ranibizumab and bevacizumab since the last two require monthly review and/or an injection of drug while aflibercept after the loading phase requires two-monthly dosing in the first year of treatment. However, an analysis of the average frequency of injections in the second year of the VIEW studies revealed only a modest difference of 4.2 injections for aflibercept versus 4.7 injections for ranibizumab.4
Implications for research
Given the relatively small advantage of ranibizumab 0.5 mg and aflibercept 2 mg over bevacizumab 1.25 mg, formal economic evaluations considering all the available evidence on treatment efficacy and side effects would be very helpful. In 2007, Raftery and colleagues presented a cost-effectiveness model comparing ranibizumab with bevacizumab.23 ,24 More recently, the National Institute of Health and Care Excellence published a technology appraisal comparing aflibercept to ranibizumab, and the authors stated that the differences in total costs and QALYs were very small.25 Given the substantial difference in the first year treatment costs of $23 400 for ranibizumab and $595 for bevacizumab if provided on a monthly basis,3 or £1000 versus £17 per injection,24 we speculate that cost-effectiveness will not be reached. On the other hand, safety of bevacizumab in the treatment of AMD remains incompletely assessed. In a recent review, Schmucker and colleagues identified substantial methodological drawbacks of existing evidence, particularly related to the quality of side effects monitoring.26 Finally, our trade-off analysis was unable to address some clinically relevant topics due to the inconsistent reporting. An individual patient data meta-analysis could attempt comparing other efficacy endpoints, such as the proportion of patients losing fewer than 15 letters or gaining 15 letters or more from baseline. Also, changes in central macular thickness would be another useful endpoint to compare with for addressing a recent discussion about the possibility that ranibizumab has a stronger effect on subretinal fluid resolution than bevacizumab.
Conclusions
This trade-off analysis, combining efficacy with side effect profiles of various anti-VEGF molecules and dosages, will contribute to create rational decision-analytic models outlining the optimal therapeutic strategy in AMD.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
Footnotes
-
Contributions MKS, LMB, LF, AGK, OMJ and MAT all played a role in the conception and design, or analysis and interpretation of the data. LMB and MAT drafted the article and all authors revised it critically for important intellectual content and gave final approval of the version to be published. LMB is the guarantor of this paper.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.