Article Text

Abstract
AIMS/BACKGROUND Phacoemulsification is rapidly replacing conventional extracapsular cataract extraction (ECCE) as the method of choice for cataract surgery in the Western world. However, posterior capsule opacification (PCO) still remains the major postoperative complication, affecting 20–50% of patients, and results from persistent cell growth of epithelial cells remaining after surgery. This study aimed to compare cell survival and growth on capsular bags following ECCE and phacoemulsification surgery using an established human capsular bag culture system.
METHODS Sham ECCE and phacoemulsification cataract operations were performed on pairs of human donor eyes. Capsular bags were dissected free, pinned flat on a petri dish, and incubated with Eagle’s minimum essential medium (EMEM) alone or EMEM supplemented with 10% fetal calf serum (FCS). Ongoing observations were made using phase contrast microscopy.
RESULTS Cell growth was observed across the posterior capsule of all preparations studied. It was found that there was no significant difference in the rate of cell growth on the posterior capsule with the two extraction methods, such that 50% confluency was achieved in 7.0 (SD 1.8) (n=7) days for ECCE and 7.43 (2.1) (n=7) days for phacoemulsification surgery. The physical changes to the capsule as a result of cell growth, such as wrinkling and capsular tensioning, were also seen in both groups.
CONCLUSIONS Cell survival and growth is dependent on the donor, rather than the surgical technique performed. There is no significant difference between phacoemulsification and ECCE surgery on the rate and nature of cell growth on the posterior capsule in vitro.
- posterior capsule opacification
- phacoemulsification
- extracapsular cataract extraction
Statistics from Altmetric.com
In recent years there has been a pronounced increase in the use of phacoemulsification for cataract surgery, such that it is now the method of choice in North America, and a similar shift is occurring in the UK.1 This technique has a number of advantages over conventional extracapsular cataract extraction (ECCE), chiefly because a smaller incision is required.2 This is believed to reduce surgically induced astigmatism23 and enables stable refraction and rehabilitation of vision and daily activities.3 Additionally, phacoemulsification surgery shows reduced inflammation and breakdown of the blood-aqueous barrier than is observed with ECCE surgery.45 Clinically, phacoemulsification represents a more involved technique, with a steep learning curve, but even in the early phase of learning, does not appear to have a greater complication rate associated with it.67
The predominant problem associated with both ECCE and phacoemulsification surgery is posterior capsule opacification (PCO), affecting approximately 30% of patients.78 PCO originates from residual anterior and equatorial cells which remain after surgery. These cells subsequently grow onto the previously cell free posterior capsule and enter the visual axis. This growth results in wrinkling of the capsular bag and cell aggregation which leads to greatly diminished visual quality.7 Interestingly, the literature suggests there is no significant difference between the two methods of surgery and the incidence of PCO,9 but it should be noted that previous studies comparing ECCE and phacoemulsification surgery with PCO incidence were not performed concurrently and therefore comparisons should be interpreted with care.
In order to compare the effect of ECCE and phacoemulsification surgery, with identical postoperative conditions on human lens cell growth, an established human capsular bag culture system was employed.10 Using this system it was possible to perform both a sham phacoemulsification and ECCE operation on a pair of donor eyes and observe epithelial cell growth on the capsular bag in a controlled situation. We could, therefore, observe every aspect of cell behaviour on the capsular bag immediately following the two surgical procedures and throughout the duration of culture in a directly comparable manner.
Materials and methods
Following removal of corneoscleral discs for transplantation purposes, human donor eyes obtained from the East Anglian Eye Bank were used to perform sham cataract operations.1011 These included continuous curvilinear capsulorhexis and removal of the lens fibre mass, followed by irrigation and aspiration of residual lens fibres. The lens fibre mass was removed by hydroexpression or by hydrodissection followed by phacoemulsification using a Site TXR phacoprobe (Iolab/Site Microsurgical Systems, Inc, Horsham, PA, USA) at 20% power using the divide and conquer technique. The capsular bag was then dissected free of the zonules and secured on a sterile PMMA petri dish. Six to eight entomological pins (D1: Watkins and Doncaster Ltd, Kent) were inserted through the edge of the capsule to retain its circular shape. Capsular bags were maintained in 1.5 ml of unsupplemented Eagle’s minimum essential medium (EMEM) (Sigma, Poole, Dorset) or EMEM supplemented with 10% fetal calf serum (FCS). All media contained 50 mg/l gentamicin (Sigma, Poole, Dorset). Incubation was at 35°C in a 5% carbon dioxide atmosphere. The medium was replaced every 3–4 days. The extent of growth on the posterior capsule was evaluated by direct observation using a combination of phase contrast and dark field microscopy. The total area within the rhexis was first determined using an eyepiece graticule. The general outline of the growth front was established by measuring the radial distance of a number of loci on the front from the rhexis and then interpolating between the loci. This was repeated over a number of days by at least two members of the group and the final map was overlayed by a grid of 1 mm squares. The areas of the posterior capsule within the rhexis and successive growth fronts were then determined by counting squares. Complete cover or confluency representing 100%.
In all cases a pair of donor lenses were used such that phacoemulsification surgery was carried out on one and ECCE on the other. Fourteen capsular bags were cultured in serum free medium throughout and four were initially grown in serum free conditions for 4 days before addition of 10% FCS to the medium. All donors were aged >60 years. Normally the eyes were enucleated within 24 hours of death. The sham cataract operation was carried out within 24 hours of enucleation.
Results
The proportion of viable cells remaining on the anterior capsule following surgical manipulations was estimated by dark field and phase contrast microscopy, where the non-viable cells were apparent by their increased light scatter and prominent nuclei. It was found that the percentage of viable cells remaining was dependent on the condition of the donor tissue (including age) and ranged from 20% to 80%. However, cell survival in the majority of capsules was between 50% and 60% of the original cell population with no bias towards either technique.
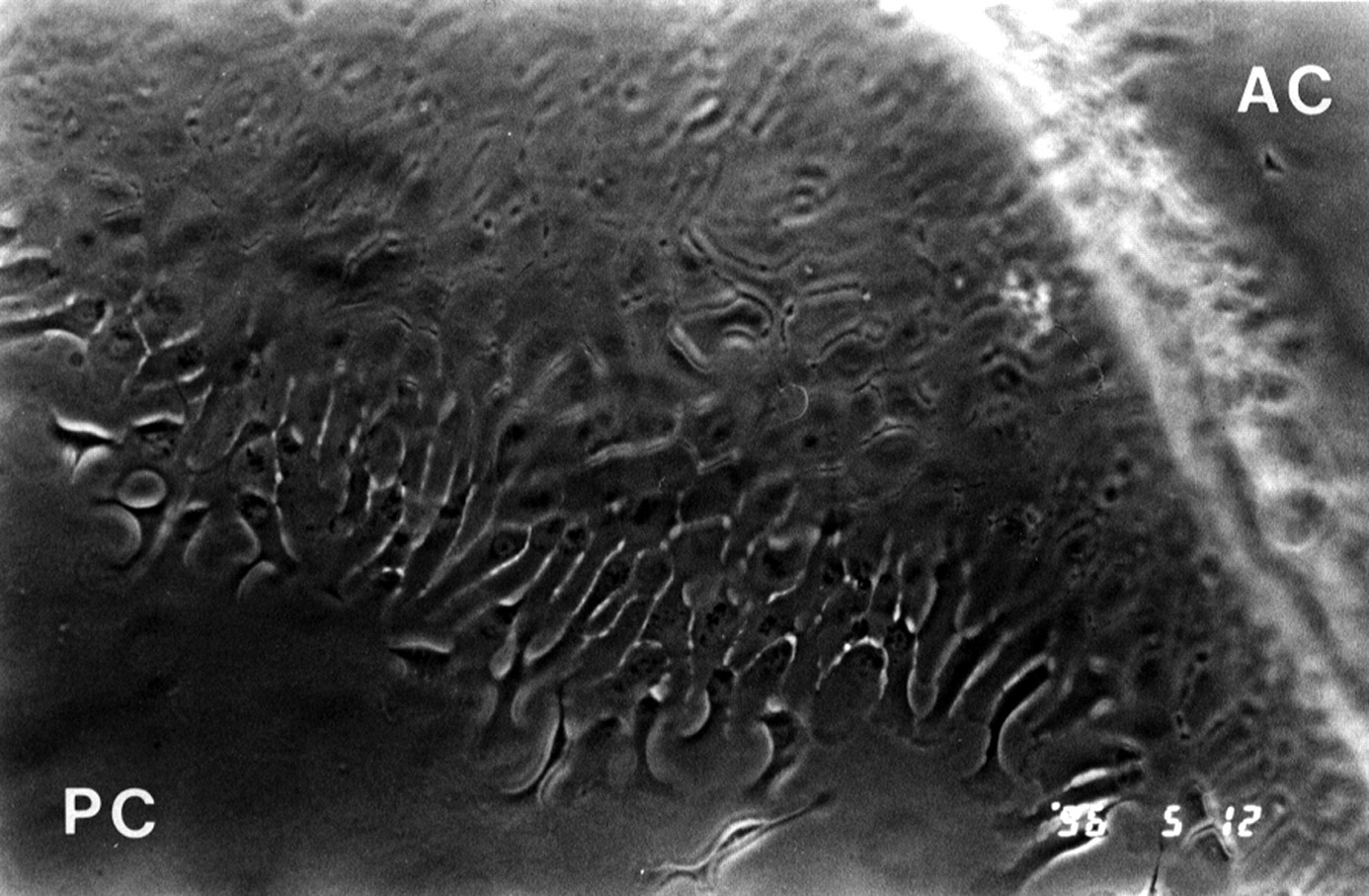
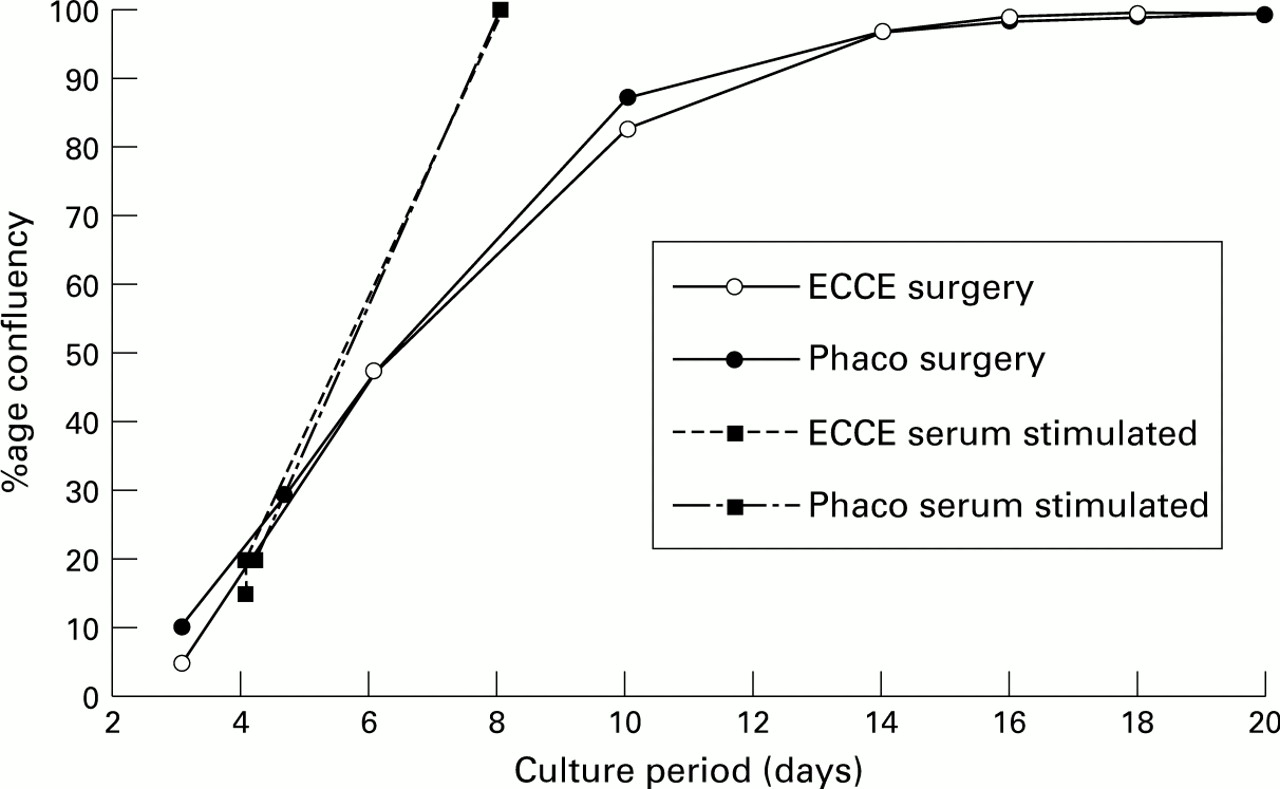
In each pair of capsules studied, the phacoemulsification and ECCE capsular bags followed a similar sequence of events as growth developed. The predominant area of study was within the confines of the rhexis as clear observation of the posterior capsule was possible. The first signs of growth in this region were observed within 2 to 6 days of culture, dependent on the donor. Following adherence at the rhexis region between the anterior and posterior capsules, cells were observed on the posterior capsule emerging from beneath the anterior capsule (Fig 1). Cells continued to move across the capsule in a relatively ordered manner, with large irregular looking cells at the growth edge and a neat pavement of cells behind. These cells ultimately covered the entire posterior capsule forming a confluent monolayer. The rate of growth is nearly identical for each donor regardless of which surgical technique was employed (Fig 2). Since ECCE was carried out on one donor eye from a pair and phacoemulsification on the other, then it was possible to carry out match paired analysis. The mean time to 50% confluency was 7.0 (SD 1.8) (n=7) days for ECCE and 7.4 (2.1) (n=7) days for phacoemulsification surgery. There was no significant difference between the two groups (p⩾0.05). When confluency was reached the capsules of both groups started to exhibit wrinkles on the posterior capsule (Fig 3) and in some cases there was a regression of cells away from the wrinkles.

Phase micrograph of cells growing on the posterior capsule (PC) in the region of the capsulorhexis (in the absence of IOL), 6 days after phacoemulsification surgery. The rhexis is the phase bright region and the anterior capsule (AC) and much of the posterior capsule is not in focus at the level of the growing edge. The micrograph represents a field of view of 1.1 × 0.75 mm.

Comparison of the rate of cell coverage of the posterior capsule, beyond the rhexis, following either ECCE or phacoemulsification surgery; 100% represents confluency. The pairs of capsules were either cultured continually in protein free medium (76-year-old donor) or were given a 10% serum supplement after 4 days of culture in protein free medium (65 years), after it was established that the initial serum free pattern was similar in both cases.

{kind=link}
{kind=link}
{kind=link}
Dark field illumination showing light scattering, associated with wrinkles near the centre of the posterior capsule. This micrograph taken 30 days after extracapsular cataract extraction represents a field of view of 3.6 × 2.4 mm.
Addition of serum supplements to the growth medium enabled capsules to reach confluency quicker (Fig 2). When serum was added, both phacoemulsification and ECCE capsular bags had reached a similar level of cover on the posterior capsule. The addition of serum induced the same response in both groups indicating that the receptors for growth agonists have not been altered by either surgical method.
Discussion
Previous studies have sought to compare the outcomes of phacoemulsification and ECCE surgery by analysing operations performed by a number of different surgeons at different institutions.9 Interpretations were further obscured by the fact that the patients were followed for different periods of time.9 In the present study the two procedures were carried out by one surgeon on a pair of eyes from the same donor and the two resulting capsular bag preparations were subject to identical culture conditions. Previous studies from this laboratory have in fact shown that human capsular bag preparations exhibit many of the characteristics of human lens cell growth in vivo1011and so are likely to provide an accurate insight into the behaviour of the capsular bags following the two types of operation.
Probably the most important finding to emerge from this study is that growth occurred on the anterior and posterior capsule in every case, and this is despite the fact that lens epithelial cells are very sensitive to mechanical trauma.12 Hence, independent of the surgical approach, a sufficient number of cells survived to provide a reservoir from which growth and migration could occur. This probably occurs because the cells that enjoy the greatest protection during surgery—namely, the equatorial cells, are exactly those which probably have the greatest potential for growth. For example, our earlier studies have shown that in the 24 hours following the operation, by far the highest number of dividing cells are located in the equatorial region and not adjacent to the wound.11 Under the conditions of the present experiments, cells are recolonising the anterior capsule and subsequently growing across the posterior capsule without additional exogenous stimuli. Under these minimal conditions both groups showed cell coverage of the posterior capsule at a similar rate and formed a confluent monolayer with later wrinkling. A confluent monolayer of cells within the visual axis is probably insufficient to cause visual deterioration.78 The peak incidence of PCO, which is clinically relevant, occurs approximately 2 years after surgery where light scatter has been ascribed to wrinkling (early), fibrosis, and pearl formation (later). The first of these has been observed in this study and further studies carried out with this model have shown that transdifferentiation of epithelial cells into mesenchymal myofibroblasts expressing smooth muscle actin also occurs at a later stage (Marcantonio JM, unpublished data). This process is probably important in initiating the clinically observed fibrosis of the capsular bag. The present model would therefore anticipate no difference in the rates of PCO development between the two types of surgery.
When 10% FCS was added to the culture medium a rapid stimulation of growth was observed. This indicates that not only do the cells have the necessary receptor and signalling systems in place, but they are also functioning normally after both types of surgical procedure. Aqueous humour and serum contain an abundance of growth factors—for example, EGF, FGF, and IGF, which have been shown to play a role in human lens cell growth.13-15 It should be noted, however, that while serum factors can stimulate growth they are not essential for growth to take place.11
The present series of in vitro experiments indicates that there is little benefit to be gained in terms of reducing lens cell growth or PCO by using phacoemulsification rather than conventional ECCE surgery and this does seem to mirror the clinical consensus.9However, any differences that possibly occur in the rate of PCO in different centres may be due to factors not included in this study. These could include differences in the amount of retained cortical lens matter, patient age,16 and disruption of the blood-aqueous barrier which has been shown to be greater with ECCE than with phacoemulsification by Pande et al.5 In vitro models provide a means of studying such clinically important factors. For example, Rakic et al17 have shown that retained fibres slow growth and our previous studies have shown both that capsular bags from young donors display a much greater cell growth rate than older capsules, and furthermore, the growth rate, at least in older capsules, can be greatly stimulated by additional serum factors.11 Such factors may be present in higher abundance in the first 24–48 hours in the aqueous humour of patients who have undergone ECCE surgery compared with phacoemulsification.5
Acknowledgments
The authors wish to thank Mrs Pam Keeley of the East Anglian Eye Bank and the staff of West Norwich Hospital, without whose efforts this study would not have been possible. We would also like to thank Drs Christopher Liu, Julia Marcantonio, and Thomasz Zarnowski for valuable discussions and Mrs Diane Alden for technical support. This work was supported by The Humane Research Trust and The British Council for the Prevention of Blindness.
References
Footnotes
-
↵Present address: Department of Ophthalmology, Addenbrooke’s Hospital, Cambridge