Article Text

Abstract
AIMS To report the special clinical manifestations and determine the appropriate management of infectious scleral ulceration.
METHODS A retrospective study was performed on 30 eyes with infectious scleral ulceration. Information was recorded on patients’ age, onset and course of disease, pathogenic organism, clinical presentations, methods of diagnosis, treatment, and outcome.
RESULTS 10 cases (33.3%) were accompanied by corneal involvement. Subconjunctival abscess was noted in 16 cases (53.3%). 17 cases (56.7%) gave positive results of pathogen culture and all were Pseudomonas aeruginosa. Two cases had combined bacterial infections and one case was complicated by fungal infection. A total of 26 cases had surgical debridement in this series. Extensive involvement of the sclera with the presence of a ‘tunnel lesion’ or a ‘satellite subconjunctival abscess’ were found during debridement. All of the eyeballs involved were salvaged except one.
CONCLUSION The results of this study were contrary to the poor prognosis presented in previous reports. Early and repetitive surgical debridement is believed to be mandatory in the intractable cases to shorten the admission period and to save these eyes.
- scleral ulcer
- pterygium
- abscess, subconjunctival
Statistics from Altmetric.com
Infectious scleral ulceration has not been reported commonly in the USA and Europe. Most reported infectious scleral ulcers are associated with systemic infection1 including tuberculosis23 and syphilis,45 severe infectious endophthalmitis,67keratitis,8-10 scleral buckling surgery for retinal detachment,11-13 or unsutured small incision cataract surgery.1415 However, reports from the areas where pterygium has a high prevalence—for example, Australia, India, Japan, and Taiwan suggest that pterygium surgery is a common predisposing cause of infectious scleral ulcers. The poor prognosis of infectious scleral ulcers has been emphasised,6810 with frequent reports of loss of the involved eye. In our series, we report more satisfactory results after aggressive management.
Patients and methods
The records of patients with culture proved or presumed infectious scleral ulcer from July 1989 to June 1994 were reviewed. Scleral extension of corneal infection, bleb related scleral ulceration and scleral inflammation resulting from underlying connective tissue disorder were excluded. Those cases with scleromalasia or poor epithelialisation of conjunctiva after pterygium excision were also excluded from our series. A total of 30 patients were studied. All of the cases had deep scleral erosion and melting with discharge or subconjunctival abscess with inflammatory reaction. Information including patient’s age, onset and course of disease, pathogenic organism, clinical presentations, methods of diagnosis and treatment, and outcome were recorded.
Results
We collected 30 eyes of 30 patients (13 males, 17 females) of infectious or presumed infectious scleral ulcer, all with history of pterygium excision. The patients were aged 48 to 86 (mean age 64.3) years at presentation. Because all of the operations had been performed elsewhere, the characteristics of pterygium and surgical procedures were not available in our study. According to the description of patients, two cases received β irradiation after pterygium removal, and the use of topical mitomycin C, thiotepa, or radiation as an adjuvant could not be identified in the other 28 cases. The interval between pterygium excision and the onset of scleral ulcer varied from 2 weeks to over 20 years. Three cases (cases 19, 21, 22) had suffered since the first postoperative day, but 10 cases (33.3%) had not developed ulcers until 10 years later.
Of the 30 patients, 10 were accompanied by corneal involvement, and four (cases 9, 13, 16, 19) were complicated by scleral perforation. Endophthalmitis was found in case 2. Posterior synechiae and/or pupil distortion were noted in 13 cases (43.3%). Subconjunctival abscess was noted in 16 cases (53.3%) under biomicroscopic examination during debridement surgery. Most of the subconjunctival abscesses did not connect to main lesion which we have classified as satellite lesions. Secondary glaucoma was a complication in eight cases and cataract in six.
The admission period varied from 3 to 98 (mean 32.5) days. Readmission was noted in eight cases because of a complicated course. All except one (case 11) had aerobic, anaerobic, and fungal cultures from the scleral scrapes on admission and biopsies during the surgical debridement. There were 17 cases (56.7%) with positive results, all of which were Pseudomonas aeruginosa. Of the 17 patients, three had combined infections. Staphylococcus epidermidiswas cultured in case 4, and Serratia marcescens was grown in case 22. In addition, case 30 was complicated by fungal infection (Cladosporium).
Of the 12 cases which showed negative results after repetitive cultures, Gram stained, KOH stained, and acid fast stained scrapings of the ulcer were done in five. Gram stained scrapings showed many Gram positive cocci in case 21, and Gram negative bacilli in case 23. Atypical mycobacteria were disclosed on the acid fast stained scraping in case 24.
The medical managements included topical eyedrops, subconjunctival injection of antibiotic, systemic antibiotic, and local irrigation of antibiotic or normal saline. Selection of antibiotics was based on the drug sensitivity tests when available. Since Pseudomonaswas the most common pathogen, amikacin was most commonly selected. In consideration of superimposed infection, piperacillin was added to the treatment. Amikacin topical eyedrops were used alone in six cases, and 21 cases had received amikacin and piperacillin eyedrops at the same time. If the area of scleral ulceration became more extensive under medical treatment or subconjunctival abscess was suspected, surgical debridement was performed to remove the necrotic tissue and to expose the ulceration. Of 26 cases receiving surgical debridement, 10 (33.3%) received debridement only once, while repetitive debridement was necessary in the remaining 16.
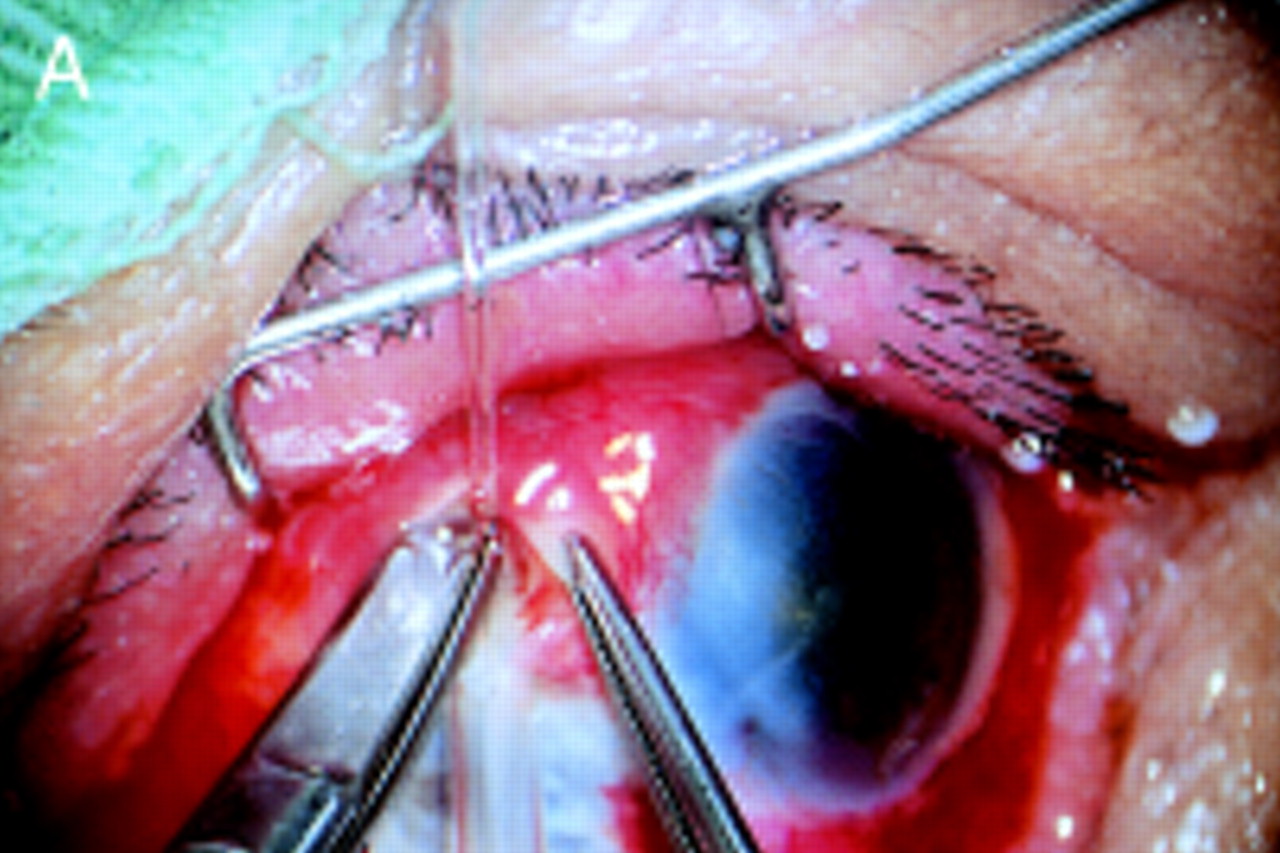
During the surgical debridement the area actually involved was generally much larger than the visible lesion under biomicroscope view (Fig 1). Case 28 may be taken as an example. In spite of the visible lesion limited to 45 degrees of sclera, 360 degrees scleral involvement was noticed during the debridement. Subconjunctival abscess and intrascleral spreading, (which we have termed a ‘tunnel lesion’) were noted where apparently healthy conjunctiva and sclera were undermined (Fig 2). In some cases, the conjunctival flap was closed completely after debridement. Unfortunately, recurrence of multiple satellite subconjunctival abscesses was noted under the closed conjunctiva. Twelve cases underwent debridement twice or more times because of recurrent abscesses. Judging from experience of several cases, we now leave the bare sclera alone rather than close the conjunctival flap after the necrotic tissue has been removed. We believe that residual micro-organisms behind the early reattached conjunctiva may cause the recurrence of infection and prolong the course despite daily local irrigation of antibiotic. Scleral transplantation and conjunctival autotransplantation were performed in seven cases. Conjunctival flap only and scleral graft only were performed in four cases and one case, respectively. All of the eyeballs involved were salvaged except in case 1, who had undergone enucleation at another clinic after she asked for discharge from our institution.

(A) The scleral ulceration was located at 9 o’clock position. Severe congestion and subconjunctival abscess were noted at 10 o’clock position under the biomicroscope. (B) After the surgical debridement, the scleral wound was left open. In comparison with (A) the involved area was more extensive. (C) Ten days later, the debrided area was healing.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) During the surgical debridement, a tunnel lesion was detected with spring scissors easily entering intrastromal space. (B) Removal of the necrotic scleral tissue with spring scissors under continuous irrigation and aspiration. (C) The area involved was much larger than the visible lesion before debridement.
Discussion
Post-pterygium excision infectious scleral ulcers have usually been reported following β irradiation,16-19 use of mitomycin C,19-24 and excessive cauterisation. In our experience, pterygium excision alone can also induce this condition. Vascular deprivation1425 has been suggested as the cause, but since the sclera is an avascular tissue with very little nutritional demand, ischaemia alone would not seem to be a main factor for this process. As David’s work has demonstrated,25when silicone was placed between episcleral plexuses and choroid and sclera to deprive both sides of the blood supply to sclera, it did not induce any scleral change, which meant ischaemia alone would not induce scleral degeneration.
Enzymatic degradation2627 may play some part in the massive invasion of scleral ulcer that developed immediately after pterygium excision. Tissue destruction during the pterygium operation and prolonged exposure of the bare sclera may stimulate enzymatic degradation by collagenases. Host derived proteoglycolytic enzymes may all be extensively involved. After the initial lysis, a defected epithelial defence mechanism can predispose to invasion by micro-organisms, and tissue lytic enzymes delivered from micro-organism—for example, protease from Pseudomonas, aggravate the process. Invading polymorphonuclear leucocytes and degenerating cells have all been proposed as possible sources of the various hydrolytic enzymes.10
Early unrecognised infectious scleral ulcer may be misdiagnosed as scleritis and treated with steroid. This can decrease the ocular defence mechanism and increase the lytic enzyme activity,27-29 and may also be a predisposing factor.
It is unusual for an operative site to be infected after a long and silent postoperative period without adjuvant management. For those cases, the trigger mechanism is still unknown for the development of scleral ulcer after a long latent period. But it is clear that necrotising scleritis can be activated after surgery.30The latent period between surgery and the onset of scleritis can be as long as 40 years.30 The situation is similar to the late onset of infectious scleral ulcer over 20 years after operation. The mechanism which induces the necrotising scleritis may be a prodromal factor to induce the infectious scleral ulcer. It can be postulated that after initiation of the necrotising scleritis, the micro-organism invaded and caused the late onset post-pterygium excision infectious scleral ulcer.
Most of the previous reports of infectious scleral ulcer pointed out that a very poor prognosis would result when micro-organisms invaded the sclera,6810 but this is not true in our cases. After managing a few cases, we soon recognised that, owing to the structure of dense collagen fibres and avascularity of sclera, antibiotic penetration of sclera is very poor, even through eyedrops, subconjunctival injection, or systemic use. We feel that debridement is mandatory in such cases. Removing the infected necrotic tissue with an open lesion is the only way to improve antibiotic treatment. A slender lesion extending only into the deep layer of sclera with the superficial overlying infection free sclera and conjunctiva was found during debridement; we call it ‘tunnel lesion’. Such lesions need careful opening and checking during debridement. A similar lesion has been reported by Raber et al 10 in their histopathological findings in cases of scleral ulcer extending fromPseudomonas corneal ulcer which was enucleated after the failure of treatment. They pointed out that medication was useless after bacterial invasion of sclera. Because Raber et alhad not identified such lesions earlier, the medical management was poor. In our experience in such cases, early debridement can save the eye. After debridement, irrigating the wound with or without antibiotic daily helped to clear the lesion. Irrigation removed the necrotic tissue, micro-organisms, and the proteolytic enzyme which usually accumulated in the deep furrow of the lesion after debridement.
We believe that early debridement and an open debrided wound are mandatory in the management of infectious scleral ulcer, no matter what the apparent size of the lesion. We emphasise the combination of medical management including systemic and topical antibiotics, subconjunctival injection of antibiotic at both ends of the scleral lesion, and wound irrigation first with antibiotic solution once or twice daily and then lactate Ringer or normal saline after improvement.
Acknowledgments
This study was conducted at Kaohsiung Medical College, Kaohsiung, Taiwan, ROC.
References
Clinical manifestations of the cases of infectious scleral ulceration