Article Text

Abstract
BACKGROUND Microbiological investigations of vitreous fluid (VF) and aqueous humour (AH) specimens have often failed to detect the infecting agent in infectious endophthalmitis, resulting in a clinical dilemma regarding therapy. In this study, the polymerase chain reaction (PCR) was evaluated in the diagnosis of bacterial andPropionibacterium acnes endophthalmitis.
METHODS 58 intraocular specimens (30 VF and 28 AH) from 55 cases of endophthalmitis and 20 specimens (14 VF and 6 AH) as controls from non-infective disorders were processed for microbiological investigations. Nested PCR directed at the 16S rDNA using universal primers for eubacterial genome was done. PCR for P acnes was performed on specimens microbiologically negative by conventional techniques but eubacterial genome positive.
RESULTS Of the 20 controls from non-infective cases, one (5%) was positive using eubacterial primers and none withP acnes primers. PCR for eubacterial genome showed 100% correlation with 20 (34.5%) bacteriologically positive specimens. Eubacterial genome, was detected in 17 (44.7%) of 38 bacteriologically negative specimens and nine (52.9%) out of the 17 were positive for P acnes genome. Among the 21 eubacterial PCR negative specimens, seven were fungus positive. By inclusion of PCR, microbiologically positive specimens increased from 46.5% to 75.8%. PCR on AH was as sensitive as that on VF for the detection of both eubacterial and the P acnes genome.
CONCLUSION PCR performed on AH and VF is a reliable tool for the diagnosis of bacterial and P acnesendophthalmitis particularly in smear and culture negative specimens.
- polymerase chain reaction
- bacterial endophthalmitis
- infectious endophthalmitis
Statistics from Altmetric.com
Bacterial endophthalmitis, the most severe form of vision threatening ocular infection may, follow surgery, trauma, bacterial keratitis, or may be of endogenous origin.1-3 Several Gram positive and Gram negative bacteria including anaerobic bacteria cause endophthalmitis.1 2 4 The value of culture of vitreous fluid (VF) and aqueous humour (AH) specimens in the diagnosis of infectious endophthalmitis is well established,5 6 but often negative cultures are encountered resulting in a clinical dilemma over the cause of the inflammation. A rational approach to the use of antibiotics and steroids necessitates determining whether the inflammation is infectious or sterile. Therefore, in such cases, an aetiological diagnosis is essential.
The new molecular biological technique polymerase chain reaction (PCR) has been evaluated in the diagnosis of several infectious diseases7-9 PCR, with universal eubacterial primers, possessing broad specificity for all Gram positive and Gram negative bacteria, has been found useful for detection of eubacterial genome in vitreous aspirates of delayed postoperative endophthalmitis cases in comparison with routine microbiological investigations. PCR, withPropionibacterium acnes primers, was also found to bea useful means of diagnosing P acnesdelayed onset postoperative endophthalmitis cases, when conventional bacterial culture was negative.10 There are many reports of P acnes causing delayed onset endophthalmitis11 12 and this bacterium may act as an adjuvant to promote the host’s immune response against lens protein.12 Owing to the localised nature of this infection in the capsular bag,12 the AH and VF might contain too few free bacteria to be detected by culture and so it was felt many of the cases of endophthalmitis that were culture negative could be due toP acnes.
Thus, the objective of this study was to evaluate the usefulness of PCR in the aetiological diagnosis of infectious endophthalmitis and, in particular, P acnes endophthalmitis by applying this technique in our clinical setting in the context of smear and culture negative intraocular specimens. We have also analysed the usefulness of PCR on AH compared with VF in this condition.
Materials and methods
CLINICAL SPECIMENS AND PATIENTS
Fifty eight clinical specimens (38 VF and 20 AH) were obtained from 55 endophthalmitis cases. Twenty clinical specimens (14 VF and 6 AH) from non-infective patients undergoing surgery for retinal detachment, vitreous haemorrhage, and diabetic retinopathy were used as control specimens.
COLLECTION OF VA AND AH
Uncontaminated VF was aspirated by syringe connected to the suction port of the vitreous cutter at the beginning of vitrectomy. A sterile disposable needle was fixed to the syringe, the air in it expelled carefully without causing aerosols; the needle was capped with a sterile rubber bung and sent to the laboratory immediately. After application of topical analgesia, AH samples (150–200 μl) were collected aseptically in a tuberculin syringe with a 30 gauge needle, and 100 μl of the sample were transferred into presterilised microfuge tubes and stored at −20°C for PCR. The rest was used for microbiological investigations.
CONVENTIONAL MICROBIOLOGICAL INVESTIGATIONS
The specimens (VF and AH) were processed within 30 minutes after collection for culture of aerobic and anaerobic bacteria (Don Whitley Compact anaerobic work station, Thane, India) and fungus. The standard methods13-15 were followed for isolation and identification of both aerobic and anaerobic bacteria and fungus. Cultures for bacteria were incubated up to 10 days and for fungus up to 30 days for growth before they were discarded as culture negative. Cytospin (Shandon, USA) smears of VF and AH were stained by Gram’s method for detection of bacteria and 10% KOH-calcofluor white wet preparation for detection of fungus.
POLYMERASE CHAIN REACTION
PCR was carried out as described below.
DNA extraction
DNA was extracted from standard strains and laboratory isolates as described by Hykin et al.10 The DNA extraction from samples was done using a modification of the above method. Briefly, 50 μl of VF/AH was added to 150 μl of TE buffer (10 mM TRIS-HCl, pH 8.0, EDTA 1 mM) containing 8 μl proteinase K (20 mg/ml) and 0.5% SDS and incubated at 56°C for 1 hour. An equal volume of phenol:chloroform:isoamyl alcohol mixture was added and centrifuged at 15 600 g for 5 minutes. The aqueous phase was removed and DNA was precipitated with 3 M sodium acetate pH 5.2 (0.1 volume) and absolute ethanol (2 volumes). After 30 minutes at −20°C, the precipitated DNA was washed with 70% ethanol, dried, and reconstituted in 20 μl TE buffer and stored at −20°C until use.
Primers
Universal eubacterial primers10 which have a broad specificity for Gram positive and Gram negative bacteria were custom synthesised by Bangalore Genie Pvt Ltd, India. The sequence of primers used for the first round of eubacterial nested PCR were U1: 5′ TTGGAG AGTTTGATCCTGGCTC 3′ and rU4: 5′ GGACTACCAGGGTATCTAA 3′ which generated a 766 bp product. Primers for the second round were U2: 5′ GGCGTGCTTA ACACATGCAAGTCG 3′ and rU3: 5′ GCG GCTGGCACGTAGTTAG 3′ which generated a 470 bp product after amplification by PCR. Primers specific for P acnes used were for the first round Pa1: 5′ AAGGCCCTGCTT TTGTGG 3′ and rPa3: 5′ ACTCACGCT TCGTCACAG 3′ generated a 387 bp product, and primers for the second round were Pa1 and rPa2: 5′ TCCATCCGCAACCGCC GAA 3′ which generated a 160 bp product after amplification by PCR.
Prevention of contamination
To prevent contamination PCR preparation, DNA amplification, and analysis of the amplified product were done in separate laboratories. PCR preparation was performed on a laminar flow work bench with single use aliquots of reagent, and dedicated pipettes. Microfuge tubes and mineral oil aliquots were double sterilised.
PCR using universal eubacterial primers
A 50 μl reaction volume consisted of 1 unit of ampliTaq DNA polymerase (Perkin-Elmer, Cetus, USA), 5 μl of 10X PCR buffer (500 mM potassium chloride, 100 mM TRIS chloride, 15 mM magnesium chloride, gelatin 0.1%, pH 8.3), 0.36 μM of each primer, 200 μM of each deoxyribonucleotide triphosphate, and 5 μl of DNA template. Distilled water was added to make it up to 50 μl. The reaction was overlaid with 50 μl sterile mineral oil. One μl of the first round amplified product was used as DNA template in the second round of amplification.
PCR for P acnes was also carried out as described above except that the primer concentrations were 1 μM instead of 0.36 μM used for eubacterial amplification. The PCR was performed in a Perkin-Elmer (Cetus, USA) automatic thermocycler (model 480). The temperatures for denaturation, annealing, extension, and the number of cycles used were as described by Hykin et al.10
PCR specificity
Both the universal eubacterial primers and P acnes primers were tested for their specificity with DNA extracted from all the principal bacteria (Table1) known to cause endophthalmitis. Ten laboratory isolates, identified as P acnes, were also tested for specificity with P acnes primers.
PCR sensitivity
Tenfold serial dilutions of DNA extracted fromStaphylococcus epidermidis in water were amplified with the universal primers U1, rU4 and U2, and rU3. Tenfold serial dilutions of DNA extracted from P acnes were amplified withP acnes primers Pa1, rPa3, and Pa1, rPa2. The sensitivity of each PCR procedure was assessed after one and two rounds.
PCR analysis of clinical specimens
Five μl of DNA extracted from each clinical sample were added directly to the PCR reaction. Each clinical specimen was amplified in the presence of two negative controls—one for sample extraction and another as a reagent control and a positive control. The PCR products were separated by electrophoresis in 2% agarose gel containing ethidium bromide 0.5 μg/ml and visualised on a ultraviolet transilluminator at 302 nm wave length (Pharmacia, Uppsala, Sweden).
Results
PCR SPECIFICITY
The universal primers U1 and rU4 (one round), U2 and rU3 (two round) amplified successfully DNA from all the bacterial strains tested to give a 766 bp product after one round and a 470 bp product after two rounds respectively. The P acnes primers amplified DNA from all P acnes isolates only to give a 387 bp product after one round and a 160 bp product after two rounds respectively.
PCR SENSITIVITY
Eubacterial primers
DNA amplification after the one round amplification permitted the detection of 1 pg of S epidermidis DNA. With nested PCR (at the end of two round amplification) 40 fg of S epidermidis DNA was detected.
P acnes primers
DNA amplification after the one round permitted the detection of 1 pg of P acnes DNA, and 50 fg of P acnes DNA after two rounds.
Results of PCR and conventional microbiological investigations of clinical specimens
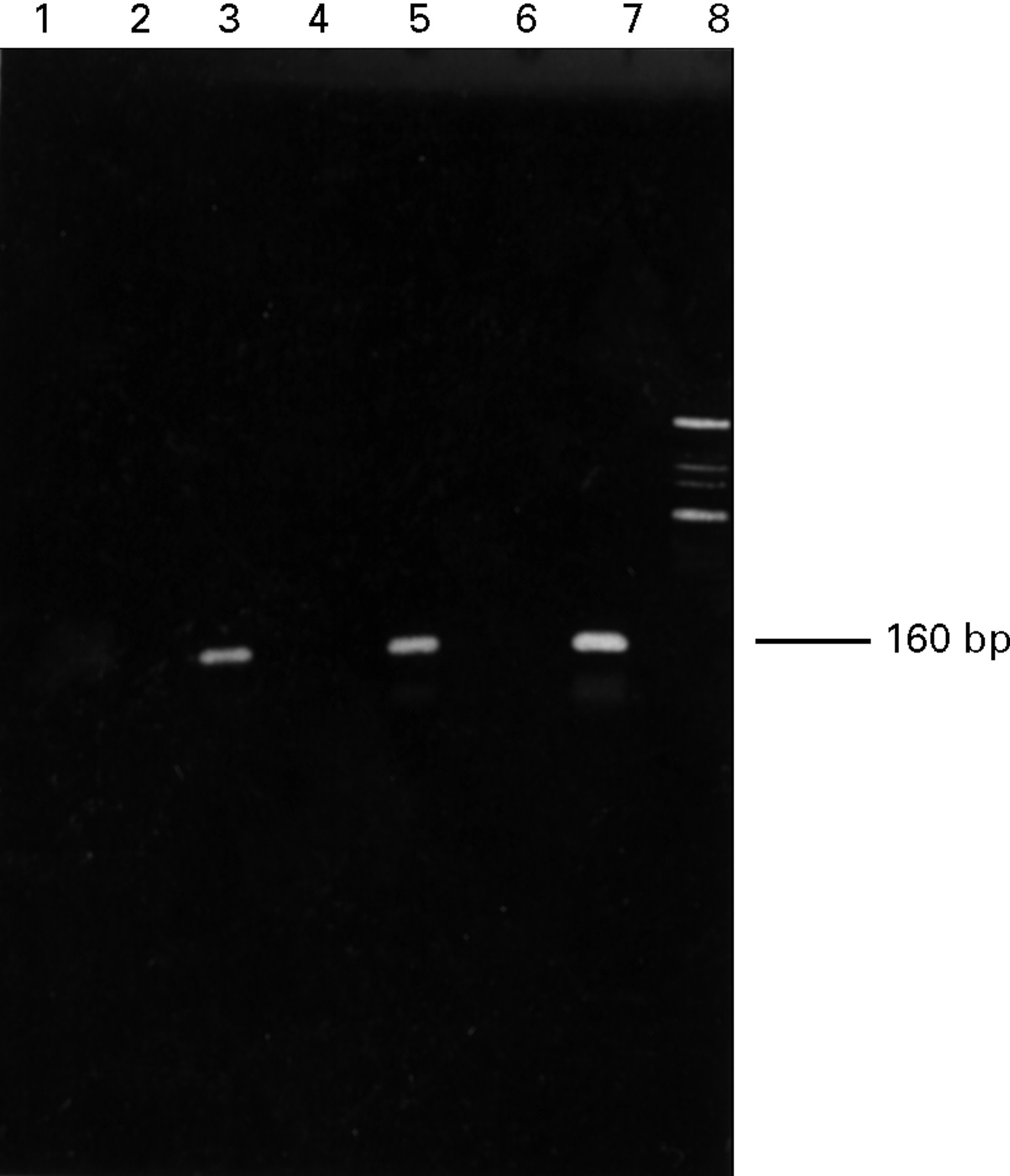
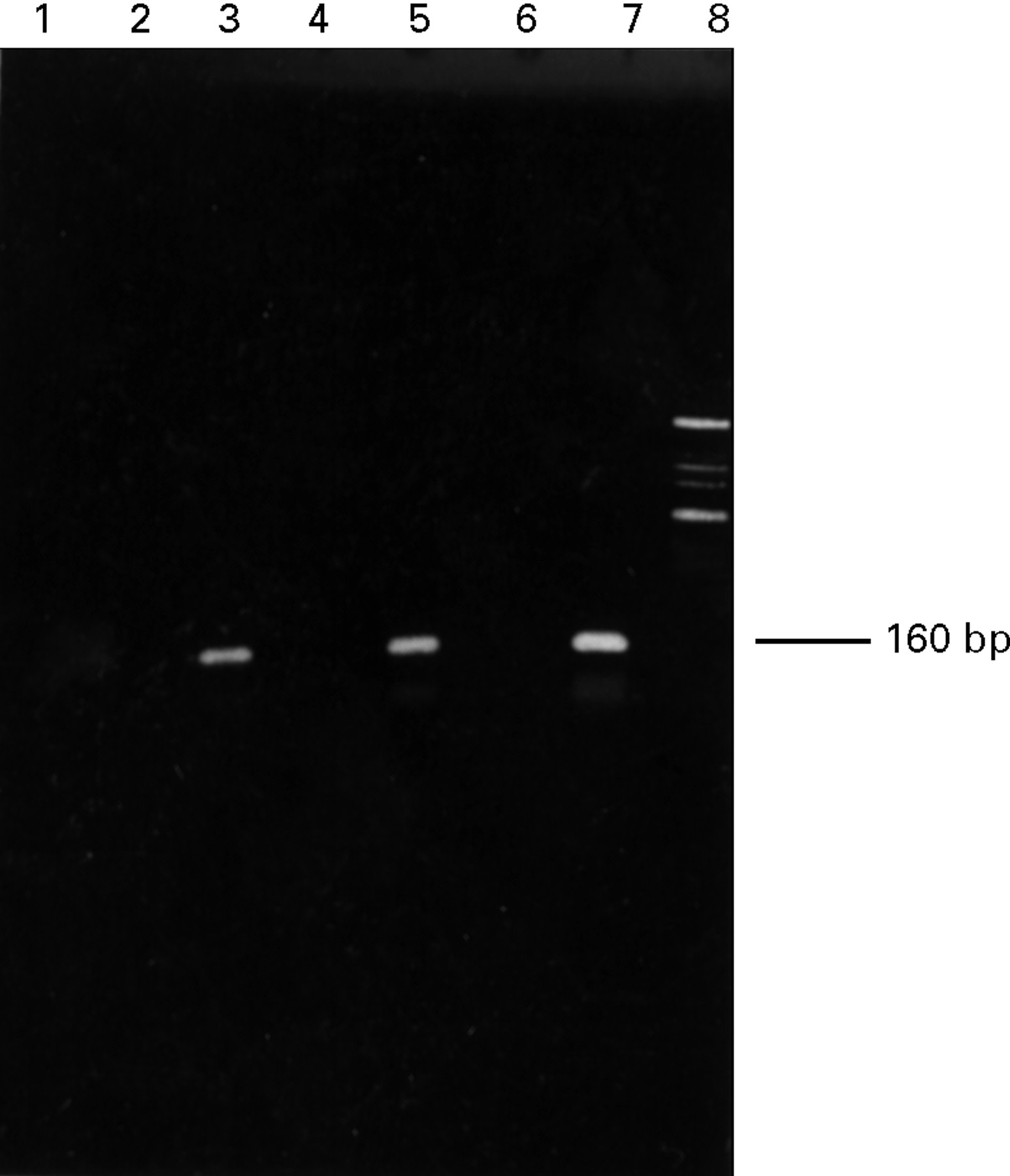
Among the 20 controls from non-infective cases, one (5%) was positive by nested PCR with universal eubacterial primers and none withP acnes primers. Hence, the specificity of PCR with eubacterial primers was 95% and 100% with P acnesprimers. The 58 specimens from patients with clinically evident infective endophthalmitis were divided into three groups based on clinical types of endophthalmitis and into four categories based on the results of conventional microbiological investigations (direct smears and cultures), as shown in Table 2. The majority of the endophthalmitis cases (36 (62.1%)) were in the postoperative group, followed by the post-traumatic (13 (22.4%)), and endogenous (nine (15.5%)) groups. Among these 58 specimens 27 (46.5%) were positive by culture, of which 20 (34.5 %) were positive for bacterial, seven (12%) for fungal aetiology, and 31 (53.5%) were microbiologically negative for infective aetiology by conventional methods (Table 2). Nested PCR for eubacterial genome showed positivity in 37 (63.8%) specimens and showed 100% correlation with the first three categories of specimens which were bacteriologically positive. Thus, PCR could detect eubacterial genome in 17 (44.7%) out of 38 bacteriologically negative specimens in the fourth category (Table 2), increasing the sensitivity from 46.5% to 75.8% for proving infectious aetiology in the specimens. The amplified products of some of the specimens are shown in Figure 1. Further PCR for P acnes with the 17 eubacterial genome positive specimens revealed the presence of P acnesspecific genome in nine (52.9 %) specimens (Table 3), indicatingP acnes to be the possible causative agent of endophthalmitis in those cases. The amplified products for P acnes at the end of two rounds of some of the specimens are indicated in Figure 2. The 21 PCR negative specimens included seven fungus positive specimens; in the rest of the 14 specimens negative by PCR and conventional microbiological techniques, infectious aetiology could not be determined. Thus, the sensitivity of detection of bacterial aetiology increased from 34.5% to 63.8% by inclusion of PCR.
Standard ATCC bacterial strains and laboratory bacterial strains used for standardisation of specificity of eubacterial and P acnes primers
Correlation of the results of conventional microbiological investigations and the PCR using universal eubacterial primers on 58 intraocular specimens from patients with clinical diagnosis of infective endophthalmitis and 20 intraocular specimens from non-infective disorders.

Nested PCR results with universal eubacterial primers U2,rU3. Lanes 1, negative control (reagents); 2, negative control (sample extraction); 3, M* 1162/96 (VF) negative; 4, M 1111/96 (AH) positive; 5, M 1537/96 (VF) negative; 6, M 59/96 (VF) positive; 7, positive control; 8, molecular weight marker (Phi X 174/Hinf 1 Digest). *M denotes the laboratory identification numbers.
Results of PCR for detection of P acnes genome in 17 smear and culture negative but eubacterial genome positive specimens
{kind=link}
{kind=link}
Nested PCR results with primers Pa1, rPa2. Lanes 1, negative control (reagents); 2, negative control (sample extraction); 3, M*1189/96 (AH) positive; 4, M 2512/95 negative (VF); 5, M 59/96 (VF) positive; 6, M 2964/96 (AH) negative; 7, positive control; 8, molecular weight marker (Phi X 174/Hinf 1 Digest). *M denote the laboratory identification numbers.
The analysis of the results of PCR on bacteriologically negative AH and VF separately showed that six (54.5%) of the 11 AH and 11 (55%) of the 20 VF were positive for eubacterial genome. Among the eubacterial genome positive specimens in the smear negative culture negative group, four out of six AH (66.66%) and five out of 11 VF ( 45.45%) were positive for the P acnes genome.
Discussion
In most recent studies approximately 75% of eyes with suspected endophthalmitis were culture positive from intraocular specimens.6 16 Our data (unpublished) on microbiological investigations of infective endophthalmitis during a period of 5 years (1989–94) indicated that 43.8% of intraocular specimens only were microbiologically positive including fungal aetiology and in the present study period it was 46.5%. The reason could be the prior antibiotic therapy, as most of our patients were referred to us after varying periods of treatment.
Postoperative endophthalmitis following cataract extraction is considered the most common form of endophthalmitis, accounting for approximately 70% of infectious endophthalmitis cases.17In our study also, the majority (62.1%) of the cases were from postoperative endophthalmitis and most (58.3%) of them were negative for bacteria by conventional microbiological investigations. However, PCR could identify 17 (54.8%) more cases with eubacterial genome, and 12 (70.5%) of them were in the postoperative group underlining the significant role of bacteria as the common cause of endophthalmitis in this group. It is a known fact that P acnes is a common causative agent in this group and our study also showed that theP acnes genome was detected in more cases from the postoperative endophthalmitis group than from the other two groups. Thus, bacteriologically positive specimens increased by 29.3% by inclusion of PCR among the laboratory techniques used in this study.
Non-infective postoperative inflammation has been attributed to many different causes, like lens design, surgical manipulation, retained soft lens matter, toxic lens syndrome, and phacogenic uveitis.18 19 In cases of post-traumatic endophthalmitis it is often difficult to differentiate the inflammation due to trauma from the superimposed infectious process and in such a situation the detection of the aetiology becomes imperative. Determination of whether a given case of endophthalmitis is infectious or sterile dictates the subsequent modification of therapy. The infective aetiology can be established only by demonstrating an infective agent in the intraocular specimen. In this study in spite of our best efforts P acnes could not be isolated in culture from any one of the specimens. However, PCR was helpful in detecting the P acnes genome in seven of the postoperative cases and two of the post-traumatic cases and thus was useful as a diagnostic test inP acnes endophthalmitis.
Previous studies1 6 20 have shown that the yield of cultures in endophthalmitis is greater from undiluted vitreous than from aqueous. Hence, it has been indicated that if infectious endophthalmitis is suspected clinically, it is essential to obtain a vitreous sample for culture.1 The reason cited is the ability of anterior chamber rather than the vitreous to eliminate infection.21 In our study, PCR on AH was equally sensitive to that on VF for detection of both the eubacterial genome and theP acnes genome in microbiologically negative specimens. These findings are extremely significant, as the anterior chamber tap is a simpler and safer office procedure compared with diagnostic vitreous aspiration. Hence, the anterior chamber tap could be the method of choice in the diagnosis of endophthalmitis when a highly sensitive molecular technique such as PCR is applied.
PCR has the potential advantages in that only a small sample is required for analysis and minute numbers of bacteria could be detected. PCR based detection of the eubacterial genome has been developed based on the conserved regions of the 16S rDNA/rRNA sequence of E coli by several groups.22 23 The small subunit of rRNA contains segments that are conserved at species, genus, and kingdom level. Universal primers chosen from 16S rDNA have a large amount of sequence information and highly conserved regions of the gene which allows for synthesis of primers that amplify a wide variety of bacteria. The specificity and sensitivity of eubacterial and P acnes primers used were very high and comparable with the previous study.10 In testing of the intraocular specimens PCR also showed 100% correlation with smear and culture results. In addition, by PCR bacterial infection could be attributed to 54.8% of bacteriologically negative specimens. In the study by Hykin et al,10 of 29 control vitreous samples, four were found to be positive for eubacterial genome by PCR. A similar positive result was found in one of the 20 (5%) control samples we tested. The false positive rate (5%) was much lower than in the previous study. As suggested by them, we also believe that it could be due to contamination with conjunctival ocular flora during collection of the specimen.
Further studies are needed to identify the specific eubacterial strains in the specimens positive for eubacterial genome, but negative forP acnes genome. Our study has clearly demonstrated that PCR on intraocular specimens, particularly in AH, is of great value as a diagnostic test and can be used as an alternative in bacteriologically negative specimens by conventional methods.